
Abstract

To the Editor:
There is much controversy and misdiagnosis in the dermatologic effects attributed to arachnidism in the United States. A modern lay press article quoted a physician who erroneously attributed a child’s necrotic leg wound to a black widow. That report highlights the persistence of confusion and misinformation among the general population and healthcare providers alike when it comes to spider envenomations. Black widow (Latrodectus sp) envenomation (BWE) can result in systemic effects known as latrodectism. Dermatologic findings including scarlatiniform rash and facial and periorbital edema are manifestations of latrodectism; however, this phenomenon may not be recognized by healthcare providers and is not mentioned in many modern references. We summarize a case of facial and periorbital edema from latrodectism that was misdiagnosed as an allergic reaction to remind clinicians of key dermatologic manifestations and appropriate management of systemic latrodectism.
A 9-y-old boy presented after a BWE. The parents found a black spider with a bulbous abdomen but did not bring the specimen to the healthcare facility. The patient described several bites to the left shoulder. Thirty minutes later, he developed severe diffuse muscular pain and spasm involving the trunk and extremities, profuse diaphoresis, diffuse erythematous rash, tachycardia (136 beats·min-1), hypertension (160/85 mm Hg), tachypnea (30 breaths·min-1), tremor, and nausea consistent with systemic latrodectism. Opioids and benzodiazepines were administered for pain and muscle spasms. A midazolam infusion at 2.4 mg·h-1 and hydromorphone 0.5 mg IV prn were administered. Tremors and muscle spasms improved with midazolam, and the dose was tapered and discontinued 3 h later. The patient’s pain, muscle spasms, tachycardia, tachypnea, and hypertension recurred, and midazolam infusion was restarted. Additional medications administered included calcium gluconate and ketorolac.
Twelve hours after the bite and 8 h after initial medication administration, facial and periorbital edema and persistent diffuse erythematous blanching rash of the lower extremities were noted (Figure 1). Hydromorphone and midazolam were discontinued, and racemic epinephrine was recommended owing to concern for anaphylaxis. Methylprednisolone, famotidine, and montelukast were administered. No wheezing, oropharyngeal edema, throat tightness, urticaria, or signs of allergic reaction occurred.
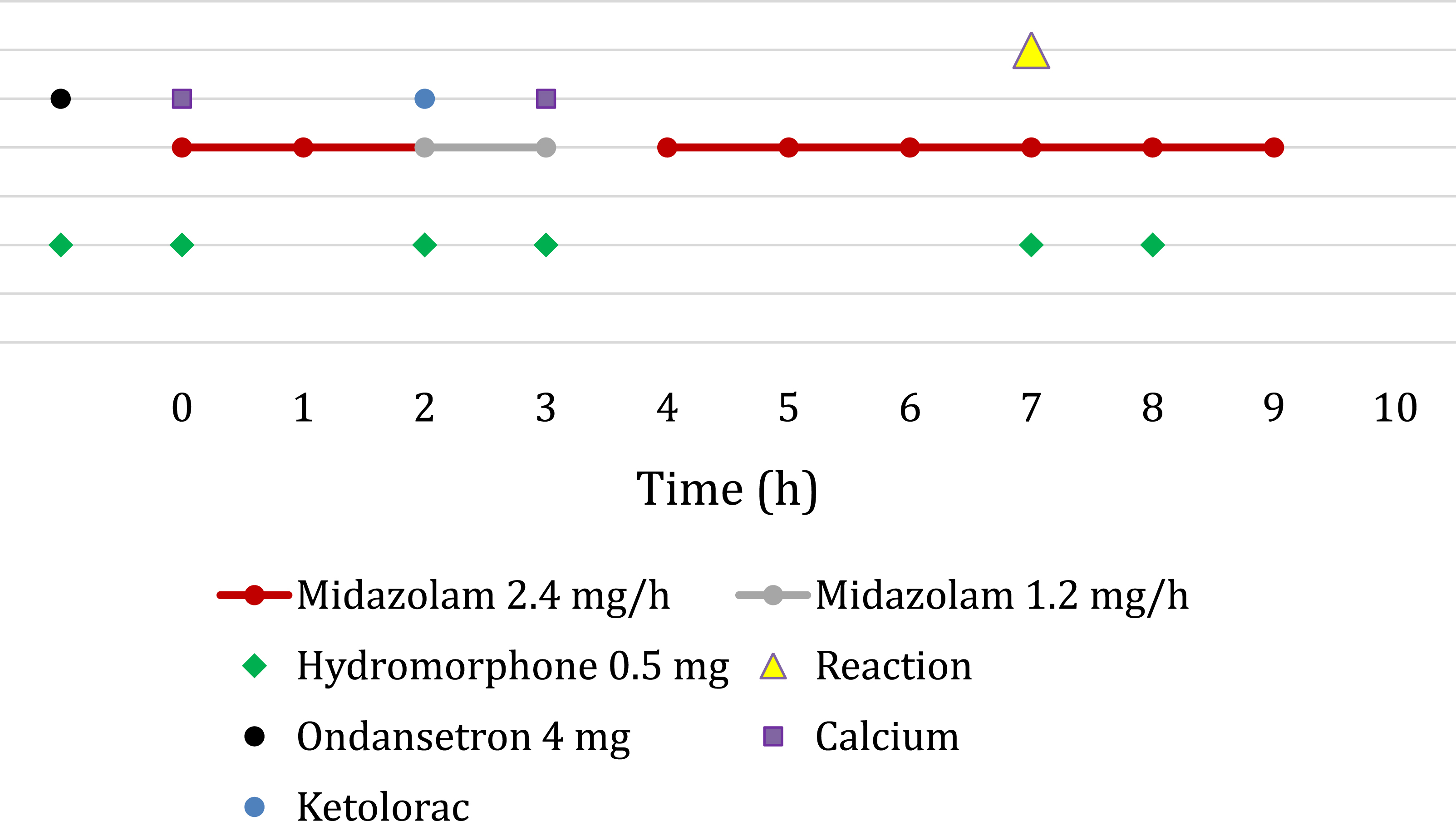
Medication administration in relation to adverse reaction after black widow envenomation.
Twenty-two hours after envenomation, the patient was transferred to our toxicology service at a tertiary care hospital, and administration of epinephrine was averted. Physical examination revealed a heart rate of 125 beats·min-1, blood pressure 140/82 mm Hg, diffuse diaphoresis, tremor, mild erythema with central clearing at the bite site (Figure 2), significant periorbital and facial edema (Figure 3), and blanching erythematous lower extremity rash. The presentation was consistent with cases of latrodectism previously encountered by the toxicology team, with the severity of diaphoresis being notable. Latrodectus antivenom was not available. Midazolam 2 mg IV q 1-h prn (total: 2 mg) and fentanyl 40 microgram IV q 30 min prn (total: 160 micrograms) were used to control symptoms, which resolved 48 h after the bite. Anaphylaxis did not occur.

Left shoulder with local erythema at black widow bite site.

Periorbital edema as a feature of systemic latrodectism after black widow envenomation.
This case serves as an important reminder of key dermatologic manifestations of systemic latrodectism that are notably absent from many modern texts. 1 –3 α-Latrotoxin is a key component of black widow venom that binds presynaptically to the calcium-independent receptor for α-latrotoxin and neurexin I-α. This binding results in transmembrane pore formation and massive exocytosis of neurotransmitters including acetylcholine and norepinephrine. The resultant envenomation syndrome ranges from local pain to diffuse pain with truncal muscle spasms and abnormal vital signs. Large muscle groups of the chest, abdomen, and back are often affected, and BWE can mimic a surgical abdomen or myocardial infarction in some patients. Rarely, priapism and seizure are reported. 2 –6 Latrodectism can present a diagnostic challenge, particularly in the pediatric population. Systemic envenomation usually resolves spontaneously within 48 to 72 h, although a more protracted course may occur.
Details of this case include report of a large black spider, discrete sensation of a bite, and classic manifestations of latrodectism evolving over the expected time frame, all supporting the diagnosis of BWE. Lack of familiarity with some of the dermatologic findings of BWE led clinicians to presume periorbital and facial edema was from anaphylaxis secondary to iatrogenic drug administration. Clinicians are often familiar with the common and well-described target lesion and localized diaphoresis. Diffuse diaphoresis, as seen in this case, is also well described in the literature. 4 Detailed description of other classic, but less common dermatologic manifestations, including facial and periorbital edema and scarlatiniform rash, is often absent from modern references 1 –3 but is described in older articles.7,8 Additionally, the term “facies latrodectismica” highlights classic features such as the grimaced, contorted expression and spasm of facial muscles. Historically the term also included the facial and periorbital edema typical of systemic latrodectism.9,10 Confusion surrounding the expression may have resulted in clinicians and modern references failing to identify periorbital and facial edema as a manifestation of latrodectism.
Latrodectus antivenom, though effective, is a whole IgG immunoglobulin and confers a significant risk of allergic reaction, and death from antivenom administration has been reported. Given this risk and the limited availability of antivenom, it is typically reserved for patients who are unresponsive to symptomatic treatment or have severe complications of BWE. Supportive care and titration of opioids and benzodiazepines may be the only treatment option available. Importantly, it should be noted that the patient in this case did not develop any signs suspicious for anaphylaxis. Urticarial lesions, bronchospasm, subjective or objective airway edema, dyspnea, hypoxia, and pruritus were all notably absent. Also key, the drugs suspected of causing anaphylaxis were not temporally related to the reaction as demonstrated in Figure 1. Despite this, opioids and benzodiazepines were withheld for approximately 10 h, resulting in inadequate symptomatic control and increased patient discomfort. Furthermore, the misdiagnosis of anaphylaxis nearly resulted in administration of epinephrine, which is particularly concerning in BWE because catecholamine excess is principal to the pathophysiology of latrodectism, and exogenous catecholamines could worsen the clinical syndrome.
In summary, this case of BWE highlights the importance of distinguishing expected findings of latrodectism, including periorbital and facial edema, from anaphylaxis. The failure to recognize dermatologic manifestations of latrodectism may contribute to misdiagnosis that may lead providers to withhold appropriate treatment and inappropriately administer potentially deleterious medications. Facial and periorbital edema, erythematous rash, and diaphoresis after BWE should raise concern for latrodectism, rather than anaphylaxis.