
Abstract
We report a series of clinical cases associated with parasitism by the Ornithodoros brasiliensis tick in a group of travelers in the Caxias do Sul municipality, Southern Brazil. These cases draw attention to underdiagnosed noninfectious syndromes caused by ticks with restricted local distributions.
Introduction
Ticks are blood-feeding parasites that are distributed worldwide. 1 They can cause a variety of damage to human and animal health, transmit pathogens, or induce severe injuries directly associated with the tick bite. 2 For instance, in North America, Dermacentor andersoni (Ixodidae) induces cases of paralysis in humans, 3 whereas Ornithodoros savignyi (Argasidae) is the causative agent of a severe and often lethal syndrome known as sand tampan toxicosis in Africa. 4 These syndromes seem to be associated with salivary toxins rather than infectious agents. For a comprehensive review of tick toxicoses, see the seminal work of Mans and colleagues. 5 In Southern Brazil, the Ornithodoros brasiliensis (Argasidae) tick is known to cause a noninfectious (toxicosis) syndrome that leads to systemic changes and severe lesions at the site of the bite. 6
Data on this tick species are scarce. To date, the known distribution of O brasiliensis is restricted to 2 municipalities in Rio Grande do Sul state (RS): São Francisco de Paula and Jaquirana. Recently, in a study compiling the reports of ticks on humans between 2004 and 2017 in RS, Brazil, 4 cases of human parasitism were reported, with ticks being collected directly from victims. 7 However, human parasitism by O brasiliensis seems to be highly underestimated and underreported: in 2013, a questionnaire-based study revealed at least 28 retrospective human cases in RS. 6 Furthermore, in addition to toxicosis syndrome, this tick species may be linked with pathogen transmission; a potential tick-borne microorganism (Borrelia brasiliensis) was once shown to be associated with O brasiliensis under laboratory conditions.6,8 Thus, this tick is important to public health given the apparent high rate of human cases with severe lesions, its potential to produce toxicosis, and its possible role in the epidemiology of Borrelia spp. Here, we report a case series associated with O brasiliensis tick parasitism involving 7 travelers after an ecotourism trail hike in the Southern Brazil highlands.
Case description
In April 2017, the travelers spent 1 night in tents at the entrance of a cave close to a waterfall, a tourist attraction in Caxias do Sul municipality (29°02'35.7"S 51°01'36.4"W; Figure 1A and B). The tourists reported that 7 people from the group woke during the night due to several painful bug bites. The guide of the group photographed one of the bugs and collected some specimens (Figure 2A).
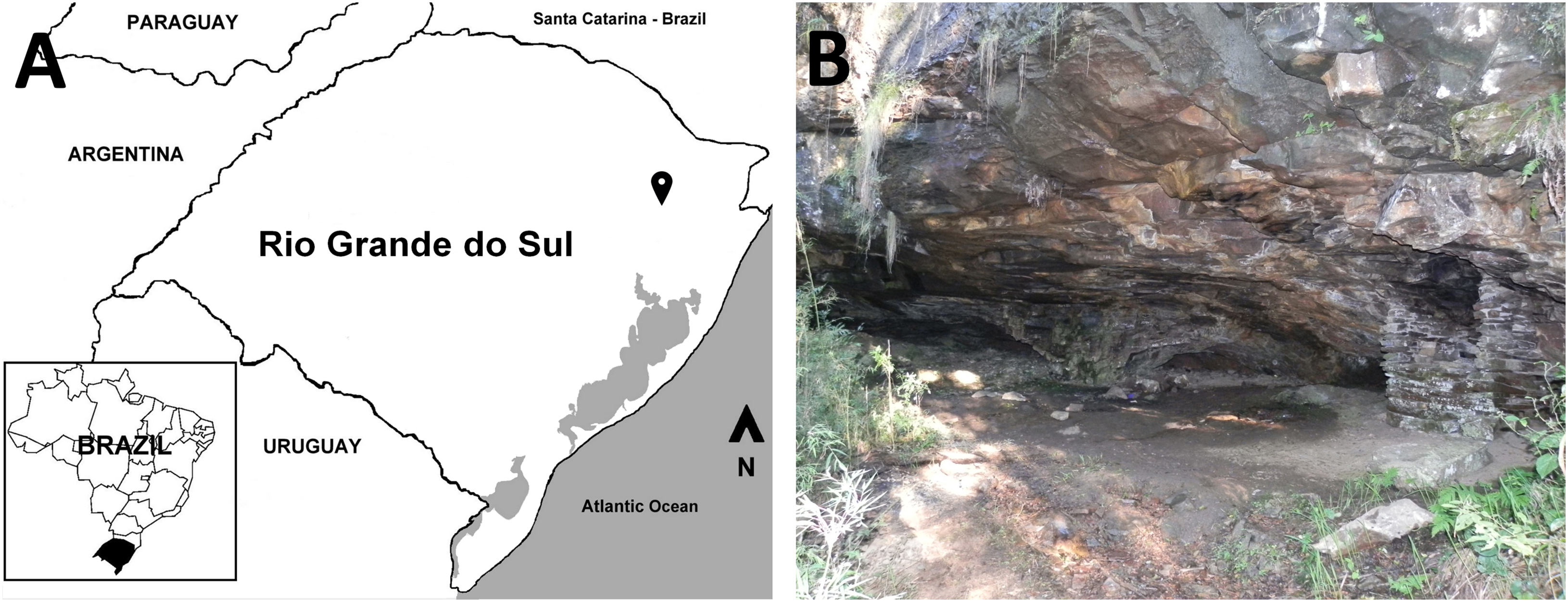
A, Rio Grande do Sul state, Brazil, and neighboring countries. Gray shading indicates bodies of water; the map-marker indicates the cave from Caxias do Sul municipality. B, Cave entrance where the tourists camped.
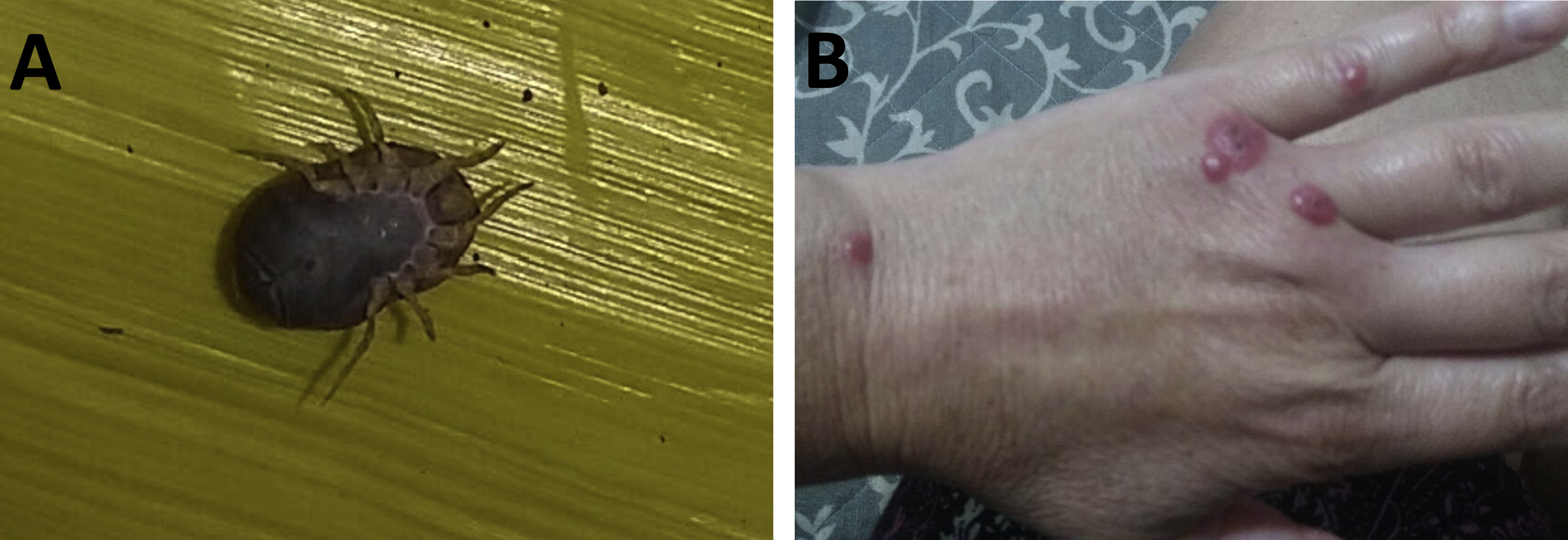
A, Specimen of O brasiliensis found attached to the body of case 1, collected and photographed by the patient. B, Lesions caused by the bite of Ornithodoros brasiliensis on the hand of case 3 at 4 wk after tick bites.
About 1 wk later, the guide (case 1, a 48-y-old man), who reported having been bitten approximately 50 times that night, sought medical attention at a municipal health center in Caxias do Sul. He reported intense pruritus at the bite sites and the formation of blisters. He was prescribed betamethasone dipropionate cream, topically. After 2 wk, the patient reported a complete recovery. The guide delivered the collected bugs to the medical center. The parasites were identified as 2 male specimens of O brasiliensis.
Four of the other 6 people who were bitten sought medical attention in their home cities. Cases 2 (a 19-y-old woman) and 3 (a 49-y-old woman; Figure 2B) were a daughter and mother bitten by approximately 20 ticks on their feet, legs, hands, arms, and neck. About 4 wk after the episode, because the symptoms had not resolved, they sought medical attention. They reported severe pruritus, erythema, edema, and blisters at the bite sites. The primary care physician in their home city told them that the tick bites were no reason for concern. They sought medical attention several additional times because of this issue. Patients 2 and 3 then received dexamethasone (intramuscular, 2 doses) and fexofenadine (oral, once a day, for 7 d). Because of the severity of her clinical presentation, patient 3 also received systemic antimicrobial therapy. Both patients reported that the lesions and symptoms remained for > 20 wk after the episode.
Patients 4 and 5 were a couple, a 31-y-old man and a 28-y-old woman. The male was bitten by 6 ticks, and the female was bitten by 3, both on their hands, abdomen, and neck. The female noticed severe pruritus, erythema, and bruises at the bite sites starting 2 d after the episode and lasting approximately 8 wk. Her husband noticed the formation of blisters and a loss of sensation around the bite site; the symptoms started about 4 d after the tick bites. He sought medical attention, and his physician prescribed systemic antimicrobial therapy for 6 d. His symptoms resolved after 7 wk. All patients who sought medical attention reported that all of their physicians said that they had never treated a victim of tick parasitism or tick-borne diseases, that they had never heard about a tick bite lesion lasting for such a long time, or that tick bites were no reason for concern.
Patient 6 was a 51-y-old man bitten by 35 ticks. He reported the formation of painful bruises around the tick bites. The symptoms lasted for approximately 4 wk. Case 7 was an 18-y-old man bitten by 3 ticks on the torso and neck. He did not report any symptoms associated with the tick bites.
About 2 mo after the parasitism episode, we visited the local area to search for ticks. A total of 2 females and 8 males of O brasiliensis were found. Ticks and patients’ blood samples were further submitted to pathogen investigation. A set of polymerase chain reaction tests for Borrelia spp and Rickettsia spp.9,10 were performed. All samples were negative on analysis.
Discussion
Locally known as mouro tick or “bicho mouro,” O brasiliensis is also designated a ground tick because of its habit of living buried in sand near host habitations, cellars, stables, and even human habitations.11,12 This tick species is responsible for severe host reactions in animals 13 and humans, 6 such as local pruritus, slowly healing lesions, local edema and erythema, focal skin rash, local pain, blisters, limb edema, malaise, headache, transient fever, and dyspnea. 6 However, to date, the salivary compounds that induce such lesions are not fully known. O brasiliensis salivary gland homogenates display potent inhibition of endothelial cell proliferation, a crucial step in wound healing. 2 In addition, studies in experimental animals (Wistar rats) have shown changes in eosinophil and basophil counts and increases in creatine kinase, the creatine kinase MB fraction, and fibrinogen level. Moreover, histopathologic analysis of bitten rats revealed edema and muscle degeneration at the tick attachment site. 14
To the best of our knowledge, this tick species had never previously been reported in the wilderness; it was only reported underneath or around human habitations in other municipalities of Southern Brazil, São Francisco de Paula and Jaquirana. 6 Herein, we reported the occurrence of O brasiliensis in a cave from Caxias do Sul municipality, which could be the natural habitat of this tick species, as previously observed for other Ornithodoros species.15,16 Both domestic and wild animals could act as food sources for O brasiliensis. 6 Thus, animals, particularly sinantropic species, could act as carriers of ticks, favoring the infestation of human habitations. According to anecdotal information from local inhabitants, periodically throughout the past decades, there have been several reports of people bitten by bugs in this area, which at least suggest that such bites may not be a recent problem.
It is important to note that Caxias do Sul is located in the main tourist region of RS, called “Serra Gaúcha,” popularly known for its beautiful scenery and immigrant culture. It also attracts several thousand foreign tourists each year, highlighting the risk of an emerging issue of imported cases of exotic tick-associated diseases. 17 In addition, Caxias do Sul is the second largest municipality in the state of RS, with an estimated population of > 500,000 inhabitants. This highlights the risk for novel cases of human parasitism.
Here, we observed a marked difference in the clinical presentation among the bitten patients, ranging from no symptoms to months of medical intervention. Of course, the number of tick bites should be taken into account; however, health practitioners must pay attention to the great individual variation in response to O brasiliensis bites and to other tick-induced syndromes.
At this time we cannot rule out that at least some of the clinical findings described here may be associated with a tick-borne infectious microorganism. We did not find Borrelia spp and Ricketsia spp DNA using the polymerase chain reaction analysis of ticks and patients’ blood. However, the blood was collected only 2 mo after the tick bites, and unfortunately only a low number of tick specimens were tested. Borrelia spp was once found to be associated with O brasiliensis in 1952, 8 but after this report, no studies have reported the microbiota of this tick species.
Although a toxicosis syndrome associated with O brasiliensis tick bites has been reported in retrospective studies with local inhabitants from Southern Brazil, to date, there have been no case reports describing it in detail. 6 The case series presented here has particular importance because it occurred with travelers. Medical practitioners should be aware that travelers, especially those returning from trails or camping, could present syndromes only known in locally restricted regions. Therefore, additional studies on the ecology (domestic and wild hosts, habitat, distribution) and potential pathogenic microorganisms in this species are peremptory, especially considering that medical authorities are usually not aware of human parasitism by this tick species.
Footnotes
Acknowledgments
We especially thank Mr. Clairton Júlio de Lima from the company Lobão Trilhas e Aventuras for the fundamental support in the execution of this work and Eduardo Kieling (SES-RS), Adriana Rhoden (Secretaria Municipal de Saúde de Caxias do Sul, Caxias do Sul, Brazil), Bruna F. Leal, Rovaina Doyle, and Fabrício Tibere Jardim (IPVDF) for their valuable help during field work.
Author Contributions
Study concept and design (BD, JR); obtaining funding (BD, JR); acquisition of the data (BD, DS, TP, PA, UAS, AW, GDS); analysis of the data (BD, DS, TP, PA, UAS, AW, GDS, CASF, JR); drafting of the manuscript (BD, JR); critical revision of the manuscript (BD, AW, CASF, JR); approval of final manuscript (BD, DS, TP, PA, UAS, AW, GDS, CASF, JR).
Financial/Material Support
This work was supported by the Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior(CAPES) and INCT em Entomologia Molecular.
Disclosures
None.
Presented at II Simpósio Nacional de Doenças Transmitidas por Carrapatos, October 16 and 17, 2017 in Rio de Janeiro, RJ, Brazil.