
Abstract
Introduction
The utility of digital intubation, especially in an austere environment with limited equipment, has been previously described. However, evidence supporting best practices for its technique is limited. We seek to quantify the time to intubation and the rate of successful placement of the tube for digital intubation using different approaches and assistance devices.
Methods
Using a manikin, digital intubation was performed with an endotracheal tube alone, with an endotracheal tube and a 14-French stylet, or with a gum-elastic bougie. All 3 techniques were performed in a crossover fashion at the manikin's side and head. Three trials per technique and position were performed. Outcomes measured were the time to intubation and the successful placement of the tube.
Results
A total of 72 timed trials were performed. A significant difference did not exist between practitioners being positioned at the head vs side in terms of time or successful placement rate. There was no difference between the time to intubation in the tube-only and stylet-assisted groups, but the bougie-assisted group was significantly slower than the others. The stylet-assisted technique was significantly more successful than the other 2 techniques.
Conclusions
In a manikin model, stylet-assisted digital intubation was the most successful technique tested and allowed intubation to be accomplished just as quickly as with an endotracheal tube alone. Bougie-assisted digital intubation was slower and may not be as helpful as when it is used as an adjunct with direct laryngoscopy. Further research is needed to determine the utility of these adjuncts on live subjects.
Introduction
Although direct laryngoscopy is the preferred method of securing an airway, an emergency practitioner must have an armamentarium of techniques for the inevitable difficult airway case or resource-limited environment. Digital intubation is a seldom-used but important airway-management technique that an emergency practitioner should be aware of if preferred airway methods fail or are unavailable (indications listed in Table 1 1 ). During digital intubation, the epiglottis is digitally palpated, and the endotracheal tube is blindly guided anteriorly by the practitioner's fingers. 2 This technique usually involves the practitioner standing to the side of the patient or at the patient's head.
Indications and complications of digital intubation
Internal stylets and gum-elastic bougies are important adjuncts in direct laryngoscopy. An internal, bendable wire stylet can provide a frame for an otherwise pliable endotracheal tube and assist in directing it anteriorly toward the vocal cords. Alternatively, a bougie, which has been shown to improve outcomes in otherwise suboptimal conditions, can aid in success by providing not only a flexible adjunct to feed into the trachea but also tactile feedback of the tracheal rings in an otherwise blind procedure. 3
Bougie-assisted digital intubation was first detailed in a case report that described a novel approach resulting in successful intubation of the trachea: digitally palpating the epiglottis before passing a bougie anteriorly into the trachea and then passing an endotracheal tube over the bougie. 4 It was theorized that the bougie's smaller size and pliable nature, vs an endotracheal tube, allowed for easier passage and possibly less trauma than traditional digital intubation.
Although the utility of digital intubation is described in the literature, 5 –7 best practices for digital intubation technique lack evidence-based recommendations regarding assistance devices (eg, bougie, stylet) and practitioner position. Thus, the goal of our study was to quantify the success rate and time to insertion for assistance devices (eg, no aide, stylet, or bougie) as well as practitioner position (ie, at the head vs at the side of the patient).
Methods
A literature search was performed using PubMed. Keywords used were wilderness medicine, airway management, laryngoscopy, digital intubation, and blind intubation. The protocol was reviewed by the Baylor Scott & White Health institutional review board and deemed not to be human subject research.
To make the findings more generalizable to the wide range of expertise of those who may employee this technique under austere conditions, 4 practitioners at various levels of training were used in this study. They included 1 emergency medicine attending physician 3 years postresidency, 2 second-year emergency medicine resident physicians, and 1 second-year medical student. At the time of testing only the attending physician had performed digital intubation on a live patient. Intubation was performed on a Laerdal SimMan (Laerdal, Wappingers Falls, NY). After a brief (approximately 10 min) instruction period describing how to perform digital intubation, each practitioner performed digital intubation a total of 18 times. All participants used the same standard digital intubation technique for each intubation attempt; a video of this technique can be viewed at
The first set of nonblinded trials involved the practitioner standing at the manikin's head to attempt intubation 3 times with each of the following: a 7.0-mm endotracheal tube (Teleflex Sheridan, Morrisville, NC; Figure 1A) alone, a 14-French stylet (Cardinal Health, Dublin, OH; Figure 1B) prestaged in an endotracheal tube, and a 15-French × 60-cm Portex Endotracheal Tube Introducer Bougie (Smiths Medical, Minneapolis, MN; Figure 1C) followed by an endotracheal tube. The bougie was not prestaged inside the endotracheal tube because its most common usage is to be placed first between the vocal cords and then to be used to thread a tube into the trachea. The practitioner then moved to the left side of the manikin and repeated the previously outlined trials. After all of the practitioners had rotated through all of the permutations, each repeated all of the digital intubation positions twice more on a rotating basis to minimize learning effect. The order was not randomized. Outcomes measured were the time to intubation (ie, the time between beginning and completing intubation) and successful placement of the tube (ie, the ability to insufflate the manikin's lungs). Time to intubation and success rate were recorded by a nonintubating member of the study team.
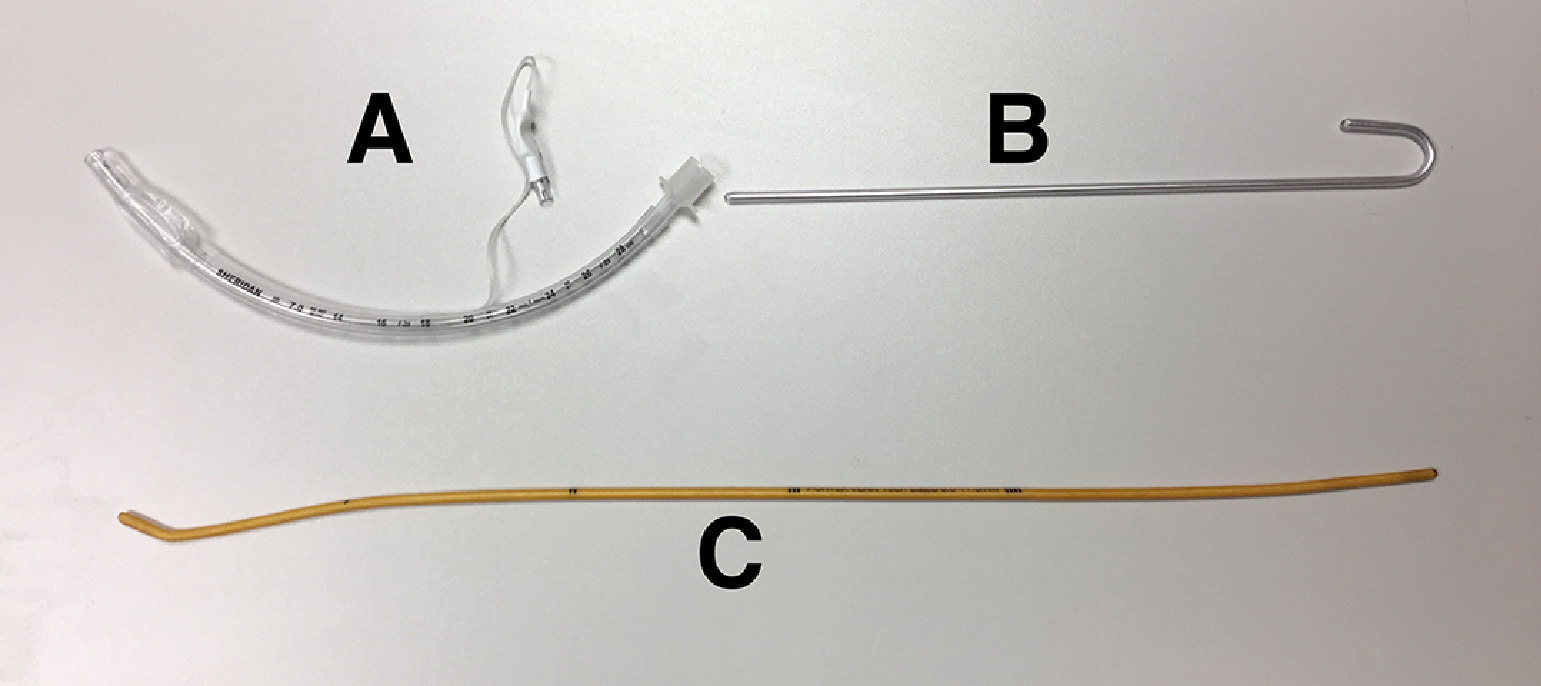
A, 7.0 mm endotracheal tube. B, 14-French stylet. C, Endotracheal tube introducer bougie.
Data were collected and analyzed using Microsoft Excel and R with R commander (R Foundation for Statistical Computing, Vienna, Austria). Continuous data were analyzed using either analysis of variance or t test, depending on number of categories. Categorical data were analyzed using χ2 contingency tables. A P value of 0.05 was selected before data collection to indicate significance. It was the hypothesis of the study group that the gum-elastic bougie would prove superior to the other methods because its utility had been established in other airway procedures, including cricothyrotomy and difficult direct laryngoscopy.8,9
Results
A total of 72 timed trials comparing practitioner position and each digital intubation technique were performed. The overall success rate for digital intubation was 93%, and the mean time to successful intubation was 22 s. A significant difference did not exist for 1) the success rate (P = 0.122) or the time to successful intubation (P = 0.596) based on the practitioner or for 2) the success rate (P = 0.164) or the time to intubation (P = 0.402) based on practitioner position.
Success rates among tube-only, stylet-assisted, and bougie-assisted intubation techniques were statistically significantly different (P = 0.011). The stylet-assisted technique produced significantly more successful attempts than expected (22 successful attempts expected, 24 successful attempts observed; subcomponent P = 0.025).
When analyzing time to intubation, the 5 unsuccessful attempts were eliminated to avoid skewing the outcomes with quick but unsuccessful attempts. A significant difference in time to intubation was found when comparing the assistance devices (Table 2; P<0.001). The bougie-assisted intubation technique was significantly slower than techniques using either an endotracheal tube alone (P<0.001; 95% confidence interval of difference in means: 15–23 s) or a stylet (P<0.001; 95% confidence interval of difference in means: 13–21 s). Comparing an endotracheal tube alone and the stylet-assisted technique did not reveal a significant difference in speed (Table 2).
Characteristics of intubation attempts by intubation-assist device
Discussion
Digital intubation is a useful method for those situations in which direct laryngoscopy has either failed or is unavailable. It is particularly useful for the wilderness medical practitioner who wishes to carry a definitive airway management tool but may not be able to accommodate the space, weight, or maintenance needed for a traditional direct laryngoscopy kit. Our study is the first to quantitatively describe best practices for digital intubation regarding practitioner position and assistance devices.
Our initial hypothesis that the gum-elastic bougie would be superior was disproven in this scenario. In a manikin model, digital intubation success rates can be boosted by using a standard stylet—a device shorter than a bougie and hence more easily stowed. This information may be useful for operators working in environments where medical equipment space is limited (eg, military, aeromedical, and emergency medical services). The lack of significant difference related to practitioner position speaks to the utility of digital intubation in austere environments where a practitioner may not be able to assume the standard head-of-the-bed position.
Stylet-assisted intubation increased success rates while maintaining the same speed as intubation attempts made with an endotracheal tube alone. This outcome is likely a result of the firm yet pliable metal of a stylet being better at holding the desired position in the glottic opening compared with the plastic of an endotracheal tube or the gum-elastic material of a bougie.
Bougie-assisted intubation increased the average time to intubation while maintaining the same success rate as intubation attempts made with an endotracheal tube alone. In looking at individual data points, several rather lengthy intubation attempts (>40 s) resulted in a larger standard deviation when compared with an endotracheal tube alone or stylet-assisted intubation. These attempts may represent difficulty deploying and directing a bougie. When compared with the maximum time to intubation using an endotracheal tube alone, it appears that the thin bougie might have “slipped” through the practitioners’ gloved fingers during several attempts, requiring extra time to regain control of the assistance device.
LIMITATIONS
The small number of data points and the variable levels of training of the practitioners may limit the validity of the outcomes. Use of novice learners could have introduced a steep learning curve to the study. Although each scenario was rotated through and repeated in an effort to minimize learning bias, the nonrandomized data collection could skew the results. The participation of several of the study authors as intubators may have introduced bias into the data collection, although the extent to which this bias was manifested in this study is unknown because our hypothesis was disproven. The use of a simulator under ideal conditions calls into question the applicability of these findings in a real-world scenario.
Conclusion
The use of the gum-elastic bougie appears to slow digital intubation and may not have as much use in this procedure as it does in other airway management skills. The stylet-assisted technique has the highest rate of success in digital intubation. An endotracheal tube and stylet are basic parts of any airway kit and are easily carried by the wilderness medicine practitioner. In a basic airway simulator model, using these 2 airway management tools in concert appears to increase accuracy of intubation without sacrificing speed when compared with using an endotracheal tube alone. Future studies using experienced providers performing the procedure on live or cadaveric subjects in a nonidealized environment may prove useful in further characterizing best practices for digital intubation techniques.
Footnotes
Author Contributions
Study concept and design (AJ, BO); acquisition of the data (AJ, BO, CR); analysis of the data (AJ, KM); drafting of the manuscript (KM); critical revision of the manuscript (AJ, KM); approval of the final manuscript (AJ, BO, CR, and KM).
Financial/Material Support: None.
Disclosures: None.