
Abstract
High altitude pulmonary edema (HAPE) is a life-threatening altitude illness that usually occurs in insufficiently acclimatized climbers in the first few days at altitudes above 2500 m. Acetazolamide is recommended for prophylaxis of acute mountain sickness, but a role for acetazolamide in the prevention of HAPE has not been established. We report a case of a trekker with previous high altitude experience who developed HAPE 8 d after arrival to altitude despite what was believed to be a conservative ascent profile.
Introduction
High altitude pulmonary edema (HAPE) is a life-threatening altitude illness characterized by fluid accumulation in the lungs. The symptoms of HAPE typically appear 2 to 3 d after reaching altitudes of 2500 m or greater. 1 The risk of HAPE increases with rapid ascent, higher altitude, respiratory tract infection, history of HAPE, male sex, decreasing temperature, and exertion. 2 The underlying pathophysiology is an increase in pulmonary artery pressure, secondary to hypoxic pulmonary vasoconstriction, which results in leakage of fluids into the alveolar spaces. 3 Gradual ascent is the primary recommendation for prevention of all altitude illnesses, including HAPE. Pharmacological prophylaxis with nifedipine is reserved for those with a history of HAPE. The utility of tadalafil, dexamethasone, and salmeterol for prevention of HAPE has not been established. Acetazolamide is effective for the prevention of acute mountain sickness (AMS) but is not presently thought to have a role in the prevention of HAPE. 4
Clinical features suggestive of HAPE are exhaustion, dyspnea on exertion, productive cough, tachypnea, tachycardia, and crackles on chest auscultation. Descent without exertion (either actual descent or simulated descent using a portable hyperbaric chamber), supplemental oxygen, and pharmacotherapy with nifedipine comprise the management of HAPE.2,4 After descent, symptoms and radiological findings should resolve rapidly. 5
We report a case of an experienced trekker without comorbidities who developed HAPE during his trek to Gokyo village (4800 m) in the Khumbu region of Nepal.
Case
During the 2017 postmonsoon trekking season, the author found a 41-y-old male Indonesian trekker short of breath near Gokyo Lake (4800 m). He was helped to the International Porters Protection Group (IPPG) rescue post at Gokyo village, 200 m away.
The patient had previously climbed Mount Kilimanjaro (5895 m) without incident. He had been well before starting the trek at Lukla (2860 m) and had followed what was believed to be an appropriate ascent profile. He reached Namche (3440 m) on his second trekking day and rested there for 2 d to facilitate acclimatization. His subsequent nights were spent at Mong La (3980 m), Dhole (4200 m), and Machermo (4470 m), and he reached Gokyo (4800 m) on the eighth day of his trek (Figure 1).
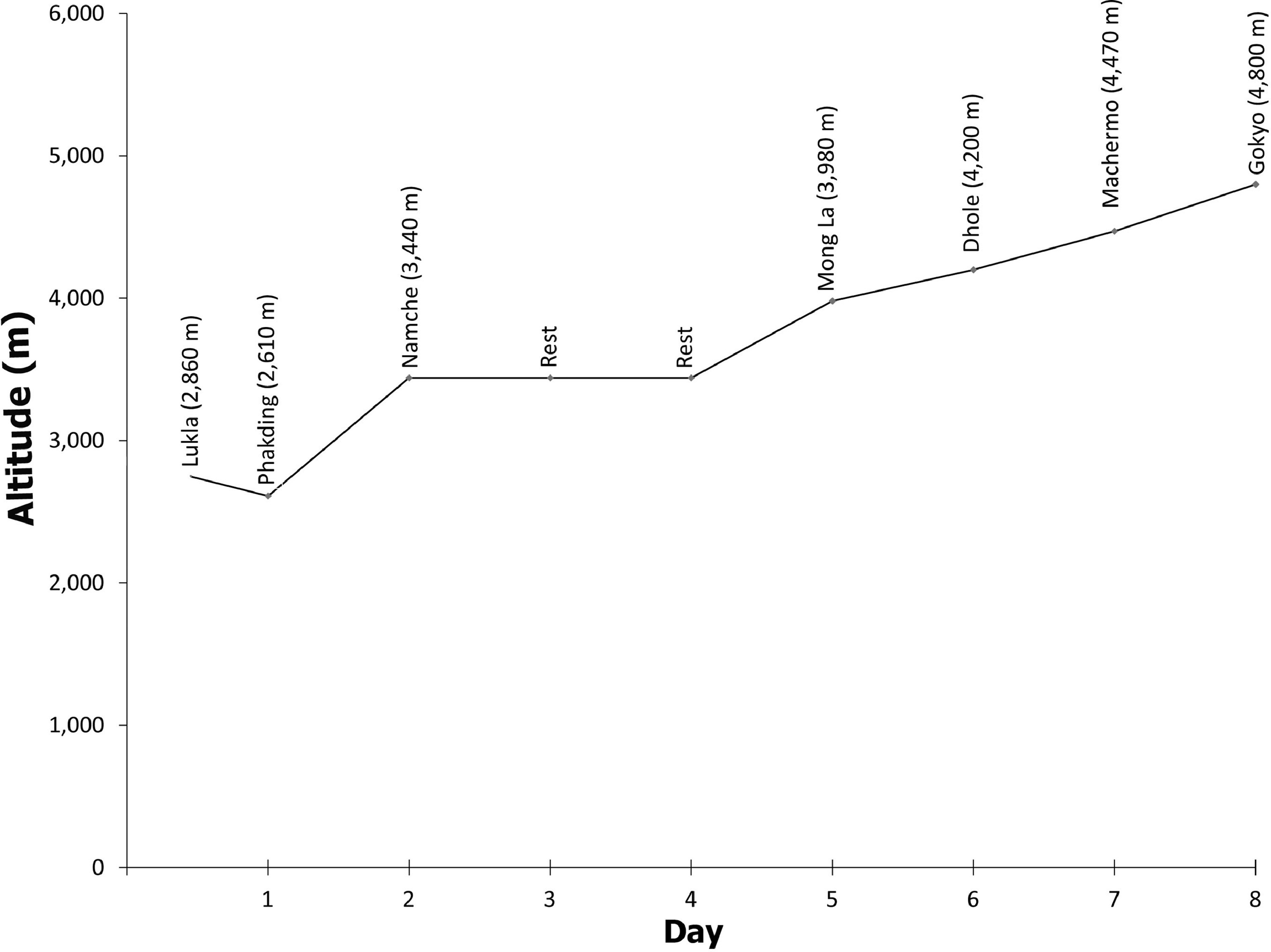
Ascent profile of the patient.
During his trek, he experienced a mild headache at Namche but developed none of the other symptoms of AMS. In response to the headache, he started oral acetazolamide 125 mg twice daily and continued it for the rest of his trek. By the time he had reached Machermo on the seventh day, he had developed a runny nose, dry cough, and dyspnea on exertion. Despite these symptoms, he continued his trek and reached Gokyo on the eighth day. His cough worsened at Gokyo, and he was dyspneic at rest. He stayed at Gokyo for 2 d but felt exhausted and spent most of the time sleeping. He tried an ascent of Gokyo Ri (5357 m) but was too breathless, so he returned to his lodge.
On arrival at the IPPG rescue post, he was coughing incessantly and was in severe respiratory distress. On examination, his pulse rate was 82 beats·min-1, respiratory rate was 30 breaths·min-1, blood pressure 120/80 mm Hg, temperature 36.5°C, and blood oxygen saturation was recorded as 46% on room air. Despite profound hypoxemia, he was alert and oriented with no evidence of ataxia. Auscultation of chest revealed infra-axillary and infrascapular crackles bilaterally.
With a clinical diagnosis of HAPE, he was started on supplemental oxygen at 6 L·min-1 via face mask and 20 mg of oral sustained-release nifedipine initially. His blood oxygen saturation increased to 80%, and his respiratory rate fell to 24 breaths·min-1 within 30 min. Later in the day, he was evacuated via helicopter to CIWEC hospital, Kathmandu (1400 m). He spent a day at CIWEC hospital. His hematological and biochemical markers were normal, and his chest radiograph showed heterogenous opacities in the middle and lower zones of his lungs bilaterally, suggestive of pulmonary edema (Figure 2).

Chest radiograph showing heterogenous opacities in the middle and lower zones of lungs bilaterally, suggestive of pulmonary edema.
Discussion
HAPE is a life-threatening form of noncardiogenic pulmonary edema. HAPE usually occurs in nonacclimatized people after ascent above 2500 m. Our patient's clinical course was different from that of the typical HAPE patient. Typically, symptoms start within 2 to 4 d of reaching high altitude; in our patient, they were significantly delayed.2,6 Our patient became symptomatic at Machermo. Had he rested or descended, he may not have progressed to HAPE. He had successfully ascended higher in the past and was a very fit and healthy individual. However, neither of these attributes would have been directly protective against HAPE. 7 Given what was expected to be a conservative ascent profile, his susceptibility to HAPE and his subsequent deterioration were likely related to his upper respiratory tract infection during ascent.
The patient started oral acetazolamide in Namche in response to a headache. Acetazolamide is effective for both the prevention and treatment of AMS, but it has no known role in prevention of HAPE. The best treatment for HAPE is descent. However, descent with exertion can further exacerbate pulmonary vasoconstriction, making the patient's condition worse. 8 The descent from Gokyo is not a smooth downhill path; there are many uphill sections before the trail reaches Namche. Because there was a suitable weather window, helicopter evacuation was the best option in this case.
We believed the starkest lesson for us, and indeed for the trekker, was that he did not seek help, either at Machermo or Gokyo, despite being within 5 min of a rescue post staffed by specialist altitude physicians in both locations. He was fortunate to have been found where he was. A survey done in Nepal found that about half of a group of 65 trekkers were unaware of the dangers of altitude illness, regardless of educational level or past experiences. 9 However, respondents also had an appetite for more information. The IPPG rescue post at Machermo and the Himalayan Rescue Association clinics at Manang (3519 m) and Pheriche (4371 m) deliver free daily talks on altitude illness and prevention for trekkers.9,10 Perhaps if he had attended a talk, he would have been more conscious of the potentially life-threatening consequences of altitude illness. The impact of these lectures on the behavior of trekkers at altitude still requires formal evaluation.
Conclusion
Our case report highlights that previous high altitude success, coupled with what was believed to be a conservative ascent profile and starting oral acetazolamide, does not rule out the development of altitude illness. Nifedipine remains the drug of choice for prophylaxis in HAPE-susceptible individuals, but trekker education regarding altitude illness may be equally important in preventing morbidity and mortality. Once a patient develops HAPE, it can be life threatening. Descent without further exertion is the treatment of choice.
Footnotes
Acknowledgments
The authors thank Drs Achyut Pokharel and Aakar Thapa for help in review of the case report.
Author Contributions: Management of case (AB); preparation and editing of the manuscript (AB, SA, JKY, and MW).
Financial/Material Support: None.
Disclosures: None.