
Abstract
Cardiac ischemia or myocardial infarction after pit viper envenomation is rare. Few case reports have been published, none describing cases reported after crotaline snake envenomation in the United States. We report a case of ST-segment elevation myocardial infarction (STEMI) occurring in a 73-year-old man after an envenomation by a juvenile canebrake rattlesnake (Crotalus horridus). The man was bitten on the left index finger and subsequently developed localized edema followed by hypotension, chest pain, and altered mental status. His initial electrocardiogram revealed ST-segment elevation in the inferior and lateral leads. His hospital course included emergent left heart catheterization with thrombectomy and cardiac stent placement. This case captures the unique medical situation involving the approach to treatment and management of a patient with a severe crotaline envenomation complicated by a STEMI.
Keywords
Introduction
Crotalus horridus, commonly known as the timber rattlesnake, is regionally distributed in the northeastern, southeastern, and eastern portions of the central United States (Figure 1). Use of the common name, canebrake, prevails and refers to the southeastern timber rattlesnake.

Crotalis horridus type A canebrake rattlesnake. Photograph courtesy of Scott Pfaff, Curator of Herpetology, Riverbanks Zoo and Garden, Columbia SC.
Around 5000 venomous snakebites are reported to poison centers in the United States each year, most of which are caused by pit vipers. 1 Envenomation syndromes from timber rattlesnake bites can include local tissue effects, hematologic toxicity, and other systemic effects. Crotalidae polyvalent immune Fab antivenom therapy is available for envenomation syndromes, particularly those that entail more severe symptoms, such as progressive edema, pain, and ecchymosis from the bite site; coagulopathy, thrombocytopenia, hypofibrinogenemia, hypotension, mental status changes, and other systemic symptoms. Less commonly seen are neurotoxic effects, such as weakness, parasthesias, and altered mental status, which should also be considered in an envenomation. 2 Venom analyses have found regional populations of canebrake rattlesnakes may contain differing combinations of hemotoxic and neurotoxic factors in their venom. 3
It is known that non-American pit viper envenomation syndromes do include myocardial ischemia, infarction, and even cardiac arrest. 4 –21 In these rare cases of ST elevation myocardial infarction (STEMI), only 2 cases have been documented in the literature as undergoing percutaneous coronary intervention.4,19 This case will outline the course and management of a North American pit viper envenomation complicated by a STEMI.
Case
A 73-year-old man was bitten by a juvenile canebrake rattlesnake on the left index finger while attempting to handle the snake at a local hunting club. The snake was captured and placed in a half-liter (20-oz) plastic bottle for identification. It had an estimated total length of 25–30 cm, but other features of the snake were not recorded. The patient rapidly developed edema, pain, and some ecchymosis in the digit and hand. The 911 system was used, and the hunters transported the patient by private vehicle to a local landmark to meet medics. Upon arrival at the emergency department, the patient was found to be hypotensive, lethargic, and diaphoretic and reported chest pain. Intravenous fluid resuscitation and oxygen therapy was initiated during transport.
Initial vital signs in the emergency department were temperature of 36.3°C, pulse of 89 beats·min-1, respiratory rate of 28 breaths·min-1, blood pressure 96/72 mm Hg, and 100% oxygen saturation on non-rebreather mask. Physical examination revealed an elderly white male in moderate to severe distress. He was diaphoretic and pale with rapid shallow respirations. There was edema of the left hand with a single puncture mark on the dorsal surface of the middle phalanx second digit. Edema with some erythema was noted to include the thumb, second, and third digits and to extend proximally into the mid-metacarpal level. He was oriented to name only with verbal prompting but was otherwise disoriented, lethargic, and confused. He was given a Glasgow coma scale of 12 with a single point off for all categories. These mental status changes prevented further history from being obtained. He had dilated pupils to 6 mm and was incontinent of both bladder and bowel while in the emergency department.
An electrocardiogram obtained revealed an acute inferolateral myocardial infarction. There was 2 mm of ST segment elevation in leads II, III, and aVF and V4–6 (Figure 2). Reciprocal changes were observed in leads aVL, aVR, V1, and V2. Laboratories demonstrated a platelet count of 524 k·µL-1 prothrombin time of 12.3 s, international normalized ratio of 0.9, partial thromboplastin time of 28.9 s, fibrinogen 712 mg·dL-1, and a point of care troponin I 0.00 ng·mL-1. The patient was resuscitated with another liter of 0.9% saline followed by 5000 units of intravenous heparin, rectal aspirin 300 mg, and 6 vials of Crotalidae polyvalent immune Fab antivenom. Hypotension resolved with fluid resuscitation and subsequent blood pressures ranged from 110 to 130s mm Hg systolic. Because of his continued altered mental status and evidence of acute myocardial infarction, he was taken emergently to the cardiac catheterization suite for coronary angiography.
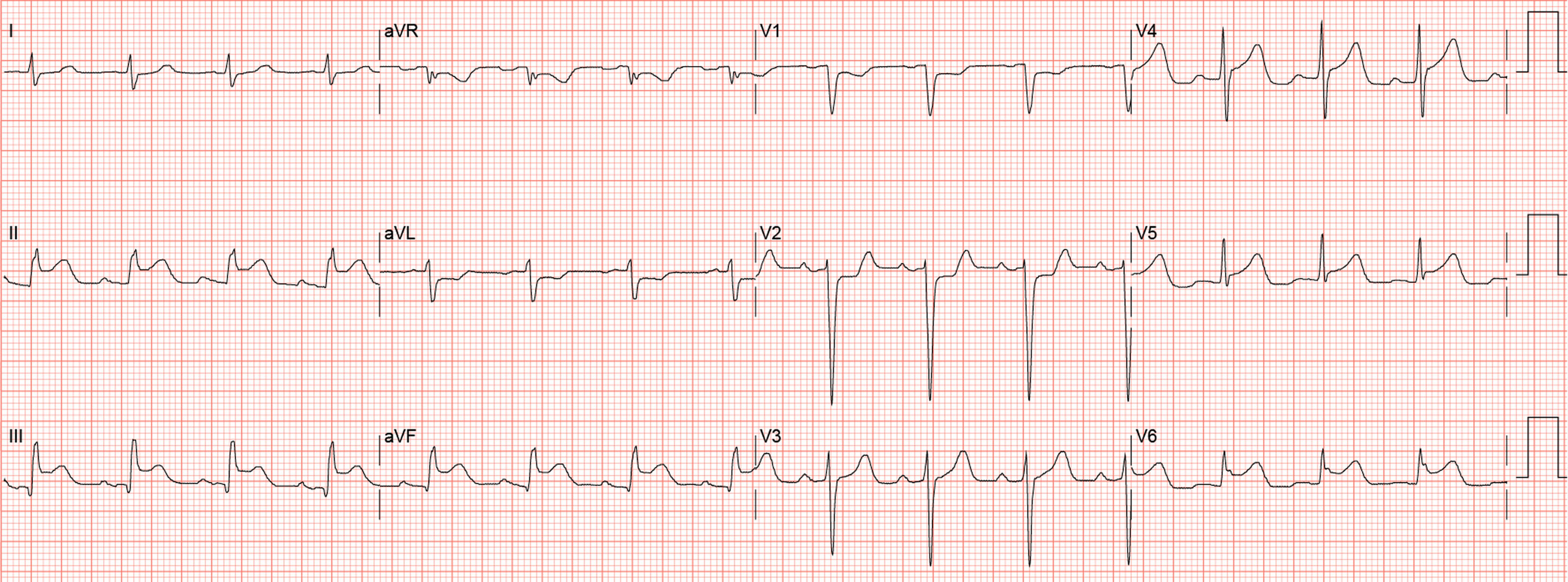
Initial patient electrocardiogram.
The cardiologist started the patient on a nitroglycerin continuous infusion. The patient was intubated in the cardiac catheterization suite by a rapid sequence intubation protocol by anesthesia due to significant hypoxemia after administration of sedative medications for left heart catheterization. During the catheterization, the patient was given eptifibatide 180 micrograms·kg-1 bolus followed by initiation of a continuous 2 micrograms·kg-1·min-1 infusion for the next 18 hours. Cardiac angiography demonstrated a 70–80% midvessel stenosis of the circumflex artery with thrombus formation. Thrombectomy followed by primary stent implantation with a 3.5 × 23 mm XIENCE drug-eluting stent was performed with no residual obstruction visualized. The remainder of the catheterization procedure revealed no significant coronary atherosclerosis. The patient was admitted to the intensive care unit. Initially, there was no progression of envenomation-related symptoms and maintenance dosing of Crotalidae polyvalent immune Fab was administered for a total of 6 additional vials with 2 vials given every 6 hours.
On reassessment during hospital day 2, the patient had edema, erythema, and warmth expanding to the left upper extremity. Mental status was not easily assessed due to sedation. Another 2 vials of Crotalidae polyvalent immune Fab was administered, in addition to initiation of antibiotics with vancomycin followed ultimately by oral cephalexin. Clopidogrel was also begun on hospital day 2 after discontinuation of the eptifibatide infusion. The patient began following commands and was successfully weaned from the ventilator and extubated by the end of hospital day 2. By hospital day 3, the patient had improving erythema and edema of the hand, and there were no findings suggestive of developing compartment syndrome. Troponin I peaked at 19.18 ng·mL-1 at 24 hours status postenvenomation. Platelet count dropped to 386 k·µL-1 and stabilized at 325 k·µL-1 on hospital day 2. International normalized ratio remained stable, as did fibrinogen, throughout the hospitalization. The patient was discharged on hospital day 6 without development of any clinically significant coagulopathy, thrombocytopenia, or hypofibrinogenemia.
Discussion
The pathophysiology of STEMI in the setting of a North American pit viper envenomation has not been fully elucidated. Several proposed mechanisms have been proposed for snakebite-related STEMI by other authors, essentially divided into direct toxin effects vs indirect mechanisms causing coronary spasm or cardiogenic shock. 4 ,5,15,16,20 STEMI in this patient cannot be attributed solely to the Crotalus horridus envenomation; rather, this case suggests that multiple factors, including prior cardiovascular disease, the experience of a stressful incident, and hypotension, ultimately led to coronary thrombosis, as evident from subsequent percutaneous coronary intervention (PCI). There are also varied results concerning the effects of rattlesnake venom on the heart. One study involving 15 patients found no myocardial damage associated with creatinine kinase elevations in canebrake envenomations. 22 Other research in rat populations has suggested there is potential for direct myocardial damage. 23
This case presented a unique challenge in medical management given the theoretical dilemma of standard STEMI treatment with anticoagulation and antiplatelet therapies while concomitantly treating a crotaline envenomation with the potential for coagulopathy and thrombocytopenia. Initial standard emergency medicine management of STEMI includes adjunctive therapies of aspirin, nitrates, oxygen, morphine, anticoagulation medications, antiplatelet therapy, and definitive PCI or fibrinolytic administration. Expert recommendation has outlined a general approach to treatment of a crotaline envenomation in the United States that aids in antivenom administration decisions. Antivenom is indicated for patients with progressive local tissue effects such as edema and pain, hematologic toxicity, and other systemic symptoms. 24 We would consider STEMI a systemic symptom and severe complication that should be treated with antivenom, especially in the presence of any hematologic toxicity and because of the therapeutic dilemma presented by the need for medications commonly used during emergent heart catheterization. Repeat bolus dosing of antivenom may be required until “initial control” is obtained when hematologic laboratories are improving or the patient is clinically improving by way of resolution of systemic symptoms or cessation of progression of the local tissue effects. Maintenance therapy is typically recommended following initial control of a severe envenomation syndrome. A delayed or recurrent coagulopathy may develop in patients who are treated and stabilized with antivenom within 2 to 7 days or even longer after dosing.25,26 Continued monitoring of coagulation studies, hemoglobin, and platelets is recommended. It is appropriate to consult a poison control center with specific expertise in the management of crotaline envenomation, especially when involving a case with such a rarely associated complication like myocardial infarction.
Given the severity of our patient’s initial presentation with hypotension and altered mental status, he was treated with antivenom and received antiplatelet and anticoagulant medications along with adjunctive and definitive therapy with PCI and primary stent implantation. This patient never developed a clinically significant coagulopathy or thrombocytopenia from the envenomation, but the same antivenom treatment approach would be beneficial and even more important in the setting of associated hematologic toxicity from the venom. There would need to be consideration of adjustment in standard antiplatelet and anticoagulant medications used during cardiac catheterization if significant thrombocytopenia or coagulopathy were present from a crotaline envenomation. Also, transfusion of products like fresh frozen plasma or platelets rarely has sustained effects unless adequate doses of antivenom are administered and may introduce significant risk. This is likely due to premature renal clearance of the Fab antivenom and the slow, sustained release of unbound venom proteins from the soft tissues into the circulatory system. 26 The potential harm of significant hemorrhage from thrombocytopenia or coagulopathy following a crotaline envenomation in addition to the antiplatelet effects from aspirin and GIIb/IIIa inhibitors and anticoagulation with heparin was not realized in our patient but could represent a complicated treatment dilemma.
Our case demonstrates that managing a STEMI in the setting of a C horridus envenomation can present unique challenges in treatment. This is such a rare event that very little in the medical literature exists on the topic. Case reports exist; however, none deal with the native North American pit vipers, and therapy in these reported patients is quite limited, with only 2 patients receiving PCI. Questions still exist regarding whether fibrinolytic therapy could even be considered in this setting in the situation where PCI was not available. Certainly, the risks and benefits of standard STEMI therapies should be weighed in the context of the individual patient’s presentation, especially when complications of bleeding could be more likely. Our patient had a good outcome with concomitant therapy of Crotalidae polyvalent immune Fab and PCI with thrombectomy and primary stent implantation after standard antiplatelet and anticoagulation therapies.
Author Contributions: Drafting of the manuscript (CHS); critical revision of the manuscript (VJL, GSS, WHR); approval of final manuscript (WHR)
Financial/Material support: None.
Disclosures: None.
Footnotes
☆
Poster presentation (Swartzentruber GS, Cibik LA, Richardson WH, Lloyd VJ. ST elevation myocardial infarction presenting as complication of Crotalus horridus envenomation) at the ACMT Annual Scientific Meeting, March 30, 2014, Phoenix, AZ.