
Abstract
Mountains are home to numerous organisms known to cause skin disease. Bites, stings, poisons, chemicals, toxins, trauma, and infections all contribute to this end. Numerous plants, animals, fungi, bacteria, viruses, and protozoa are responsible. This paper aims to review skin illness and injury sustained from organisms in the mountains of North America. Other factors such as increased ultraviolet radiation, temperature extremes, and decreasing atmospheric pressure along with human physiologic parameters, which contribute to disease severity, will also be discussed. After reading this review, one should feel more comfortable identifying potentially harmful organisms, as well as diagnosing, treating, and preventing organism-inflicted skin pathology sustained in the high country.
Introduction
Mountainous terrain covers approximately 22.5% (1.8 million square kilometers) of the contiguous United States (Figure 1). Globally, 20% of Earth’s lands are mountainous, with an estimated 400 million permanent human residents. 1 Additionally, mountains attract a large number of visitors for work, recreation, and religious reasons. 1 Outdoor recreation, including hiking, skiing, mountaineering, climbing, and rafting have become very popular in the past century. 2 Both permanent residents and visitors are exposed to common and unique dermatological injuries and illnesses. This paper reviews skin disease caused by fungi, bacteria, Animalia, protozoa, and viruses in the mountains of North America.
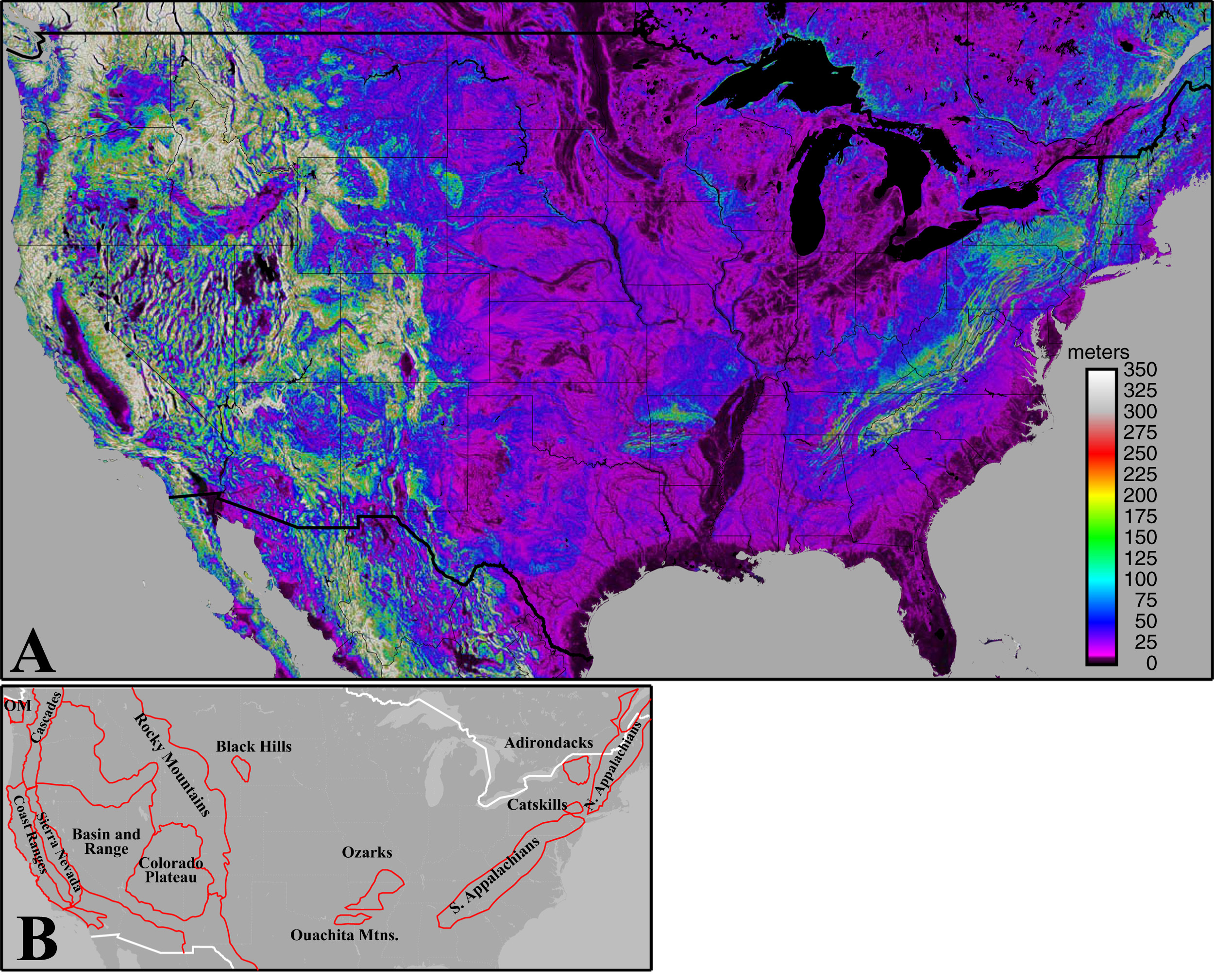
A, Topographic relief within a 3 km (∼1.9 mile) radius, defined as the elevation of each point on a 0.5 x 0.5 arcsecond grid minus the lowest elevation of any grid point within 3 km. Low-relief areas (eg, river valleys, lakes) plot as black. Mountainous areas plot as green to white. B, Outlines of mountainous areas in the conterminous United States. OM, Olympic Mountains. Topography data from:
Plants are responsible for a number of skin reactions including contact and irritant dermatitis, urticarial rashes, phytophotodermatitis, and rashes secondary to Euphorbiaceae and saponin plant toxidromes. 3 –6 Tick-borne vector illnesses including anaplasmosis, ehrlichiosis, Lyme disease, and rickettsial illnesses such as Rocky Mountain spotted fever, tularemia, tick-borne relapsing fever, and Colorado tick fever are also known to cause rash. 7 –9 As skin pathologies from plants and tick-borne vector illnesses represent extensive topics and are already well-cited in the medical literature, they have been omitted from this review. Please reference the above cited sources for more information on these interesting topics.
No universally accepted criteria exist with regard to what constitutes a mountain, hill, or mountainous terrain. In this review, the authors defined mountainous areas according to topographic relief. Any increase of ≥100 m (330 feet) elevation over a horizontal distance ≤2 km (1.24 miles) met criteria for mountain terrain (Figure 1). This definition is intentionally inclusive and does not exclude terrain based on absolute altitude. These environments are, among themselves, highly variable ranging in elevation from sea level to 6190 m (20,310 feet; Denali, Alaska) in North America. 10 As such, the degree of exposure to weather and ultraviolet radiation, along with potentially harmful organisms encountered, differ substantially between ranges and even within habitats on a given mountain. Some organisms are unique to the mountain wilderness, while others may be encountered in multiple outdoor settings.
Exposure to ultraviolet radiation increases roughly 1% for every 30 m of elevation gain. Temperatures drop approximately 1°C for every 150 m of elevation gain. The atmospheric pressure decreases with altitude, therefore lowering the amount of oxygen available for respiration. At 2000, 4000, 6000, and 8000 m, respectively the available oxygen is only 79, 63, 49, and 37% of that at sea level (about 1% less per 110 m gain to 5000 m). Relative humidity also decreases with elevation while weather, including wind speed, temperature gradients, precipitation, and overall exposure are often more severe, more difficult to predict, and highly variable. 1 ,11,12 All of these factors often contribute to make skin pathology more severe and difficult to treat in the mountain environment.
Fungi: Mushrooms
Contact dermatitis (CD) from the Toxicodendron species (poison ivy, oak, and sumac) and other varieties of plants is the most common cause of CD, thought to be responsible for greater than 50 million cases per year in the United States. 3 Much less well-known is CD from mushrooms, the fruiting bodies of fungal organisms, when handled by susceptible individuals. 13 The pruritic rash is typically reported as erythematous swelling at the site of contact. Rashes develop in 1 or 2 days and last about 1 week. 13 No treatment is necessary and either avoidance or use of rubber gloves is recommended for prevention. 13 Culprit genera include Ramaria, Paxillus, Lactarius, Boletus, Agaricus, and Suillus. Suillus granulatus (Figure 2) can be found after summer rains on the pine-covered foothills of the Rocky Mountains. 14

Suillus granulatus. Source: Leif Goodwin (
Bacteria: Staphylococcus, Streptococcus, and Yersinia
In recent epidemiological studies, cellulitis represented 2 and 4% of total illnesses among participants in National Outdoor Leadership (NOLS) classes.15,16 Abscesses, carbuncles, furuncles, pyoderma, erysipelas, and wound infections are also known to occur in the mountain wilderness.1,17 Causal bacteria are generally Staphylococcus and Streptococcus species. 18
While such infections are common outside of the mountain environment, several factors combine to make bacterial skin infections more common, harder to treat, and often more severe at high altitudes (>2500 m). 1
Reduced atmospheric pressure, hypoxia, increased ultraviolet solar radiation, extremes of temperature, wind, and low humidity have a detrimental effect on the host immune system. 1 Overcrowding and poor sanitation, often found in high mountain camps, also play a role in certain instances. 1 The frequency of soft tissue injuries in mountainous recreation (11–23% of total incidents 19 ) from skin punctures, lacerations, and abrasions provide constant potential nidi for infection. Finally, those participating in wilderness outings, such as mountaineering, endure prolonged physical exertion coupled with inadequate sleep, further compromising host response. 20
Hypoxia reduces the number of CD4 cells and functionality of T lymphocytes in general. 1 Since T lymphocytes instruct the adaptive immune response, the functionality of other immune cells may also be affected. Innate immune cells, such as neutrophils and macrophages, do not appear to be directly affected by hypoxia. 1 While the precise physiologic mechanisms are poorly understood, rates of bacterial infection, severity, response to therapy, and antibiotic resistance are all affected by altitude.
Abscesses should be incised and drained. Cellulitis, erysipelas, and wound infections should be treated with appropriate antibiotics. 18 Any wounds, including lacerations, avulsions, and abrasions, should be cleaned thoroughly with copious potable water under 6 to 12 psi. 20 Foreign bodies and dirt should be removed. 20 Petroleum jelly can be applied to improve wound healing parameters, along with a sterile dressing to help keep wounds clean. 21 Descending to a lower altitude may be required if wounds and bacterial infections do not respond appropriately to the above treatments. 1 Tetanus boosters should be obtained, as indicated, prior to any mountainous travel as Clostridium tetani may contaminate open wounds. 1
Zoonotic bacterial infections can spread via arthropod vectors. 7 For instance, the gram-negative rod, Yersinia pestis is transmitted to humans via the bites of fleas (and, rarely, respiratory droplets from infected individuals) that live on cats, prairie dogs, squirrels, rabbits, and other rodents. 22 From 1900–2012, approximately 1006 cases of plague (80% bubonic) have occurred in the United States, mostly in rural western states. 23 The 4 corners area where Colorado, Utah, Arizona, and New Mexico meet represents the geographic epicenter. 23 Even with appropriate antibiotics, such as doxycycline or fluoroquinolones, 16% of cases are fatal. 22 The most common form of the disease, the bubonic plague, is characterized by the development of painfully swollen lymph nodes, or buboes (Figure 3), in the first few days of illness. Fever, malaise, nausea, and vomiting are other common symptoms. 22 Avoiding animals that are known carriers, along with insect repellant on clothing and skin, are excellent precautions. Flea control for pets should also be utilized. 22

Buboes. Swollen, ruptured inguinal lymph node in a patient with bubonic plague. Source: CDC (public domain). Reproduced with permission.
Arachnida: Spiders, Ticks, Mites, and Scorpions
This diverse class of organisms are ubiquitous throughout the world, and can be found in varying numbers to elevations as high as 6750 m (22,145 ft), for example, Euophrys omnisuperstes, the Himalayan jumping spider. 24 Some of these 8-legged arthropods are capable of bites, stings, envenomation, and the spread of vector-borne diseases.
Spiders are blamed for numerous bites every year, but are probably responsible for only a small percentage of claims. 25 Many species of spiders may bite humans, but only a few are medically relevant. 26 For example, bites from black widow spiders (Latrodectus spp.) predominantly cause painful muscle cramping and localized diaphoresis without surrounding cellulitis or necrosis (Figure 4). Bites from the brown recluse spider (Loxosceles reclusa), on the other hand, cause a localized skin necrosis in about 40% of individuals (Table 1). 26 This species can be found throughout the Appalachian and Ozark Mountains, as well as the surrounding flat lands. Other species of spiders (eg, wolf spider) have been reported to cause mild local reactions as well. 27

Black widow bite with associated localized diaphoresis. Source: Peter Pons, MD.
Dermatologically significant venomous animals found in the mountains of North America
Hard ticks (Ixodidae spp) are common in the summer months throughout North America’s mountains. These parasites latch onto victims, taking blood meals for up to several days, sometimes spreading diseases, and even rarely injecting small amounts of venom, which can cause transient paralysis.26,28 Ticks should be removed by pulling them out perpendicular to the skin, without twisting, using a forceps or other similar device. 26 Tick removal methods that utilize heat, nail polish, and petroleum jelly can cause harm, as the animal may regurgitate infectious stomach contents back into the host. 26 In the summertime, individuals should check their skin frequently for ticks and remove them immediately. Prompt removal significantly reduces the transmission of Lyme disease, tick paralysis, as well as other vector-borne illnesses. 26 If Lyme, rickettsial, or other bacterial tick-borne vector illness are suspected, prompt initiation of a suitable antibiotic, such as doxycycline, is recommended. 7 Light-colored clothing can make ticks easier to spot before they are able to latch. Foreign body granuloma from retained body parts, secondary infections, irritant, and contact dermatitis are other dermatological lesions caused by ticks. Soft tick (Argasidae) bites can cause vesiculobullous lesions, necrotic ulcers, and significant edema. 7
Mites (subclass: Acari) have adapted to nearly every environment on earth. 29 Chiggers, the larval form of mites, as well as the common name for the Trombiculidae family of mites, are very familiar to hikers who travel through tall grasses in summer months. These small arachnids travel to areas of tight-fitting clothing (eg, socks and underwear) and bite. 26 Their saliva, along with ticks, can trigger an immunoglobulin E, Th2 response, causing erythematous-edematous pruritic papules, which are almost always excoriated (Figure 5). 30 Other families of mites are also dermatologically relevant. Scabies (Sarcoptes scabiei) may be present in overcrowded high mountain camps. 1 The red spider mite (genus: Tetranychus) feeds on plant material, and possibly algae, in and around many of the natural hot springs found in the mountains of Idaho. 30 ,31,32 These mites bite and lay their eggs in the skin of soakers. The human immune system removes any eggs left. 30 However, an erythematous, very pruritic, excoriated rash develops 1 to 2 days after exposure. Rash is self-limited and usually resolves in 1 to 2 weeks.

Chigger bite on the leg. Source: Desiree Davis, RN. Reproduced with permission.
Scorpions are nocturnal animals highly associated with the American Southwest, but extend as far north as Canada, and are found on every continent except Antarctica. 33 Three species, the Northern scorpion (Paruroctonus boreus), the Northern desert black hairy scorpion (Hadrurus spadix), and the common striped bark scorpion (Centruroides vittatus) are found in Colorado, the state with the highest mean elevation in the union. 34 It is likely that scorpions sting more the 20,000 Americans every year, as 2009 saw 17,154 poison center calls.33,34 The Arizona bark scorpion (Centruroides exilicauda, formerly sculpturatus, Figure 6, Table 1) is the only truly dangerous species in North America, capable of killing small children. 6 ,30,33 Avoidance and symptomatic treatment including oral analgesics and cold compresses should be utilized with regard to most scorpion stings. 6

The bark scorpion (Centruroides exilicauda). Source: Rich Wagner of WildNaturePhotos (
Insecta: Ants, Bees, Wasps, Flies, and Mosquitoes
Moths, butterflies, bees, wasps, ants, flies, mosquitoes, termites, lice, and fleas are all members of the class Insecta (Table 2). 35 Bites are the most likely manifestation of an unfavorable encounter, but stings, contact, and irritant dermatitis may also occur (eg, moth contact dermatitis 36 ). Bites cause local trauma, minor inflammatory reactions, pruritus, and discomfort mostly in late spring, summer, and early fall (Figure 7). 26 In almost all cases, symptoms are self-limited. Organisms should be removed manually or with water, and pruritus can be controlled with calamine lotion, cold compresses, and oral antihistamines. Severe reactions to bites may be ameliorated with topical and, rarely, oral steroids. General avoidance, proper barrier clothing potentially treated with permethrin, nets, and repellants such as 20 to 50 % N,N-diethyl-3-methylbenzamide (DEET), 20% Picaridin, and 30% PMD (oil of lemon eucalyptus) are proven methods to prevent bites. DEET is safe in the second and third trimester. 37 Frequent reapplications are required for efficacy, and slow-release formulas are available.
Insecta: dermatologically relevant orders in North America’s mountains

Unspecified arthropod bite with central punctate and surrounding erythema.
It should be noted that insects, and especially mosquitoes, are responsible for hundreds of millions of cases of vector-borne illnesses worldwide including malaria, Zika, yellow fever, and Ebola every year. Furthermore, mosquitoes are responsible for more human deaths than any other organism, other than humans, with estimates of over a million per year.9,38 The altitude and supratropical latitude of most of North America’s mountains afford almost complete protection from the above mentioned vector-borne threats, however.
Reptilia: Lizards and Snakes
Snakes (Serpentes) and lizards (Lacertilia) will bite humans, particularly if handled, cornered, or surprised. Most North American species are nonvenomous, but secondary infection can occur. 39 The use of broad-spectrum prophylactic antibiotics, such as ampicillin-sulbactam is controversial, and may be highly dependent on the particular species. 39 Proper wound care, including copious irrigation with potable water, should always be utilized. 40 Two species of venomous lizard, the Gila monster (Heloderma suspectum) and the beaded lizard (Heloderma horridum), can be found in North America’s desert Southwest, including the mountains of this region. 41 United States poison centers had received 105 total calls for Gila monster bites in humans as of 2014. 42 Symptoms are mostly systemic, but dermatological manifestations including swelling and urticaria from anaphylaxis can occur (Table 1). 41
Worldwide, venomous snakes are responsible for 50,000 to 100,000 human deaths annually. 43 In the United States and Canada, approximately 5 to 8 people are killed every year by venomous snakes, though an estimated 3000 venomous snake bites occur annually. 40 Two families of venomous snakes, coral snakes (Elapidae) and Old and New World pit vipers (Viperidae) can be found in North America. 40 Coral snakes, relatives of the cobra, are found in the American Southeast, Texas, and Arizona. Coral snakes are not typically found in mountainous terrain, but rattlesnakes are.
North American rattlesnakes, copperheads, and water moccasins (cottonmouths) belong to the subfamily Crotalinae (New World pit vipers), and all possess heat-sensing pits located between their nostrils and eyes. 40 Water moccasins are not found in the mountains, but copperheads (genus Agkistrodon) can be found throughout the Appalachian and Ozark Mountains. 40 Rattlesnakes (genera Crotalus and Sistrurus) can be found in Mexico, the United States, and southern Canada to elevations as high as 3000 m, and are responsible for the vast majority of venomous snake bites in these countries. 40 Rattlesnakes commonly encountered in mountainous ecosystems include the timber rattlesnake (Crotalus horridus – Appalachian mountains), prairie rattlesnake (Crotalus viridis – Rocky Mountain foothills and valleys), black-tailed rattlesnake (Crotalus molossus – Oaxaca to northern New Mexico, Figure 8), and the Northern and Southern Pacific rattlesnakes (Crotalus oreganus and viridus – Sierra Nevada mountains). 44 –46 Dermatologic effects, such as erythema, swelling, tenderness, and, occasionally, bullae and purpura, are the most common physical manifestations of pit viper envenomation (>90% of cases, Figure 9). 40

A black-tailed rattlesnake (Crotalus molossus) coiled and waiting for prey. Source: Rich Wagner of WildNaturePhotos (

Rattlesnake bite: severe dermatologic reaction with bulla and purpura. Source: Christopher Hoyte, MD, and Department of Toxicology, Good Samaritan Regional Medical Center. Reproduced with permission from Christopher Hoyte.
Copperhead and rattlesnake venom is a complex mixture of proteins and polypeptides. Venom components vary considerably, even geographically, between species.40,43 Furthermore, the amount of venom injected also varies, with approximately 20 to 25% of bites being completely dry.6,40 In general, bigger snakes inject greater quantities of venom. 6 Symptoms include local swelling, erythema, pain, hematologic derangements, nausea, vomiting, fasciculation, diaphoresis, and shock. 6 Clinical treatment only differs for a few species, which contain presynaptic neurotoxins such as the Mojave rattlesnake (Crotalus scutulatus). 40 Species identification is key, and a picture from a safe distance may be very helpful (avoid a second bite). Evacuation to formal medical care and blood tests including a complete blood count (CBC), prothrombin time/international normalized ration (PT/INR), fibrin, D-dimer, creatinine kinase (CK), and urine blood are indicated. 6 Basic treatments are listed in Table 1. 47 For more comprehensive recommendations and treatment algorithms, see the Kanaan et al study. 40 Many myths exist regarding venomous snake bite management. Oral or mechanical venom suction, intentional laceration of the bite wound, tourniquet, pressure bandaging, cryotherapy, and electricity should all be avoided. 40
Protozoa: Trypanosoma, Leishmania, and Giardia
Protozoal parasites including Schistosoma, Onchocerciasis, and Trypanosoma are common causes of dermatological illness in both mountainous and nonmountainous regions. 17 Fortunately, these organisms are essentially nonexistent in North America, though rare cases of Chagas have been reported in the southwestern United States.17,48 Thirty cases of cutaneous Leishmaniasis from the bite of the sand fly (Lutzomyia) have been reported, mostly in Texas and other nonmountainous areas. 48
Giardia lamblia, a flagellated protozoa, typically causes diarrheal illness when these parasites colonize the upper gastrointestinal tract. 48 These organisms can be found in high mountain streams and lakes throughout North America, when large mammals carrying the parasite excrete cysts into water sources. 17 While exposure to Giardia is often asymptomatic, around 19,000 cases of giardiasis are reported annually in the United States. 48 Giardiasis generally consists of anorexia, abdominal cramping, and explosive foul-smelling diarrhea 1 to 2 weeks after ingestion. 48 While cutaneous manifestations are rare, 1 case report did demonstrate granuloma annulare skin lesions in a patient with giardiasis that subsequently cleared with treatment. 49 As many infections go unreported or are not published, it is not known how often such skin manifestations occur. Of interest, 1 small study in Egypt found that 7.4% of Giardia infections in children were associated with atopic disease. 50
About half of the individuals infected with Giardia will clear the parasite spontaneously. Those that do not require nitroimidazole compounds, such as metronidazole (95% cure rate). Prevention of giardiasis can be effectively achieved by properly sterilizing water before ingesting. 17
Mammalia: Bison, Mountain Lions, and Bears
Large mammals including bison, moose, elk, mountain lion, brown bears, and black bears are responsible for attacks on humans every year in the mountains of North America. 17 ,51–54 While the number of encounters between humans and animals increases yearly, incidents are rare. 52 Some attacks are thought to be unprovoked, but the vast majority occur after agitating or startling animals (Figure 10). 17 ,51–53 Serious cutaneous injuries from teeth, claws, horns, antlers, and hooves often result. 17 Table 3 lists the frequencies of confirmed attacks, fatalities, locations, and bacterial infections that may result from the bites of bison, bears, and mountain lions. Some have attributed other “missing persons” to bear and mountain lion attacks, but such claims are difficult to substantiate. Injuries sustained from mammals necessitate copious irrigation and excellent wound care to avoid infection.17,20 Appropriate antibiotics may also be required, depending on the species and severity of traumatic injury. 17 The size and power of these large mammals often results in considerable pathology, necessitating hospitalization and surgical management.

Photographer dangerously close to a male American buffalo (bison); Jackson, Wyoming. Source: Kevin Capps. Reproduced with permission from Dan Capps.
Mammal attacks and fatalities in specific locations throughout North America, 1890–1997
Viruses (Nonvector): Rabies and Hantavirus
Smaller mammals can also cause traumatic skin lesions. The rabies virus is extremely rare in North America. However, bats, raccoons, skunks, and foxes are known reservoirs for the virus (Figure 11). 20 As such, any wound sustained from one of these animals should be copiously irrigated, ideally with a virucidal solution (eg, povidone-iodine), closure should be delayed, and prompt post-exposure prophylaxis (PEP) should be initiated. 20 PEP includes wound care, local rabies human immunoglobulin, and multiple doses of the rabies cell culture vaccine. 20

Bats are known reservoirs of the rabies virus. This family was found nestled in a popular rock climbing crack; Clear Creek Canyon, Colorado. Source: Tom Califf, MD and William Brandenburg, MD. Reproduced with permission.
Rodents may serve as reservoirs for hantavirus, a group of viruses in the bunyavirus family. 55 Many can cause disease in humans when the stool and urine of infected animals is aerosolized and inhaled. Bites are also thought to be responsible in rare cases. 55 Sin Nombre virus, a type of hantavirus carried by the deer mouse, causes hantavirus pulmonary syndrome (HPS), a devastating disease characterized by nonspecific symptoms like fever, muscle aches, and fatigue. Four to 10 days later, infected individuals develop coughing and shortness of breath from pulmonary edema secondary to increased vascular permeability, which can be fatal.56,57 HPS manifests 1 to 8 weeks after exposure and had a mortality rate of 38% in the 690 reported US cases (as of 2016, 96% in Western states). 57 HPS occurs throughout North and South America from multiple hantaviruses, and, importantly, rash carries negative predictive value for the disease. In Europe and Asia, different strains of hantavirus cause hemorrhagic fever with renal syndrome, which often causes a petechial rash. 56 Those who live in rodent-infested housing are at greatest risk, but hikers and backpackers who share campsites and trail sheds with infected rodents are also vulnerable. 57 Treatment is supportive, and, as for all of the above-mentioned life-inflicted injuries and illnesses, avoidance is the best preventative practice.
Conclusions
The mountains of North America represent a myriad of ecosystems that house a vast number of different organism, many of which are dermatologically relevant. Bites, stings, envenomation, toxins, and sometimes even just contact with potentially harmful species, may lead to traumatic skin lesions, rashes, reactions, and infections. Whereas, many encounters cause only temporary discomfort, others can be fatal (Table 4 does not include domestic animals, or those found outside of the mountains, such as alligators and sharks). 58 Pain, pruritus, or both appear to be the most common symptoms associated with unfavorable encounters, while clinical signs vary greatly. When possible, avoidance is the best intervention and also the most environmentally correct.
Human fatalities caused by animals in the Unites States, 1999–2015
Increasing outdoor activity in mountain wilderness areas will almost certainly lead to increased encounters between humans and other living inhabitants. This review highlights some well-known, interesting, and unique skin pathologies caused by organisms in the mountains of North America. A considerable number of species and dermatologic manifestations are covered in this paper. However, many more life-inflicted skin pathologies exist, are yet to be documented, and likely are yet to be discovered. As encounters between humans and many species are rare, the authors strongly encourage any outdoor enthusiasts who contact living organisms, and subsequently develop skin or other such pathologies, to share their findings. Case studies represent the most logical approach for such reports.
Acknowledgments: The authors thank the United States Geological Survey for providing the software and data files used in making Figure 1. Thanks also to Dan Capps for sending the first author newspaper clippings and articles concerning animal inflicted human attacks and fatalities weekly for the past 12 years.
Author Contributions: Study concept and design (WB); acquisition of the data (WB, WL, TC, CM, CL); analysis of the data (WB, WL, CM, CL); drafting of the manuscript (WB, CM, CL); critical revision of the manuscript (WB, CL); approval of final manuscript (WB, WL, TC, CM, CL).
Financial/Material Support: None.
Disclosures: None.
Footnotes
Submitted for publication October 2016.Accepted for publication February 2017.