
Antihypertensive therapy with angiotensin-converting enzyme inhibitors (ACEIs) has long been associated with facial and oropharyngeal angioedema and reflexive coughing, which are attributed to increased bradykinin levels from antagonism of the enzymatic degradation of bradykinin by ACEIs. 1 –3 More recently, antihypertensive therapy with ACEIs has been associated with severe allergic reactions, including anaphylaxis, after hymenopteran stings and venom immunotherapy for hymenopteran venom allergies, which are again attributed to systemic accumulation of bradykinin. 4
The angiotensin receptor antagonists or blockers (ARBs) were developed as a newer class of antihypertensive medications that avoided inhibiting both the angiotensin I–converting enzyme and the kinases of bradykinin by blocking the interaction of angiotensin II at one of its 2 receptors (AT1). 3 Figure 1 depicts the mechanisms of action of the ACEIs and the ARBs on the renin-angiotensin pathway.
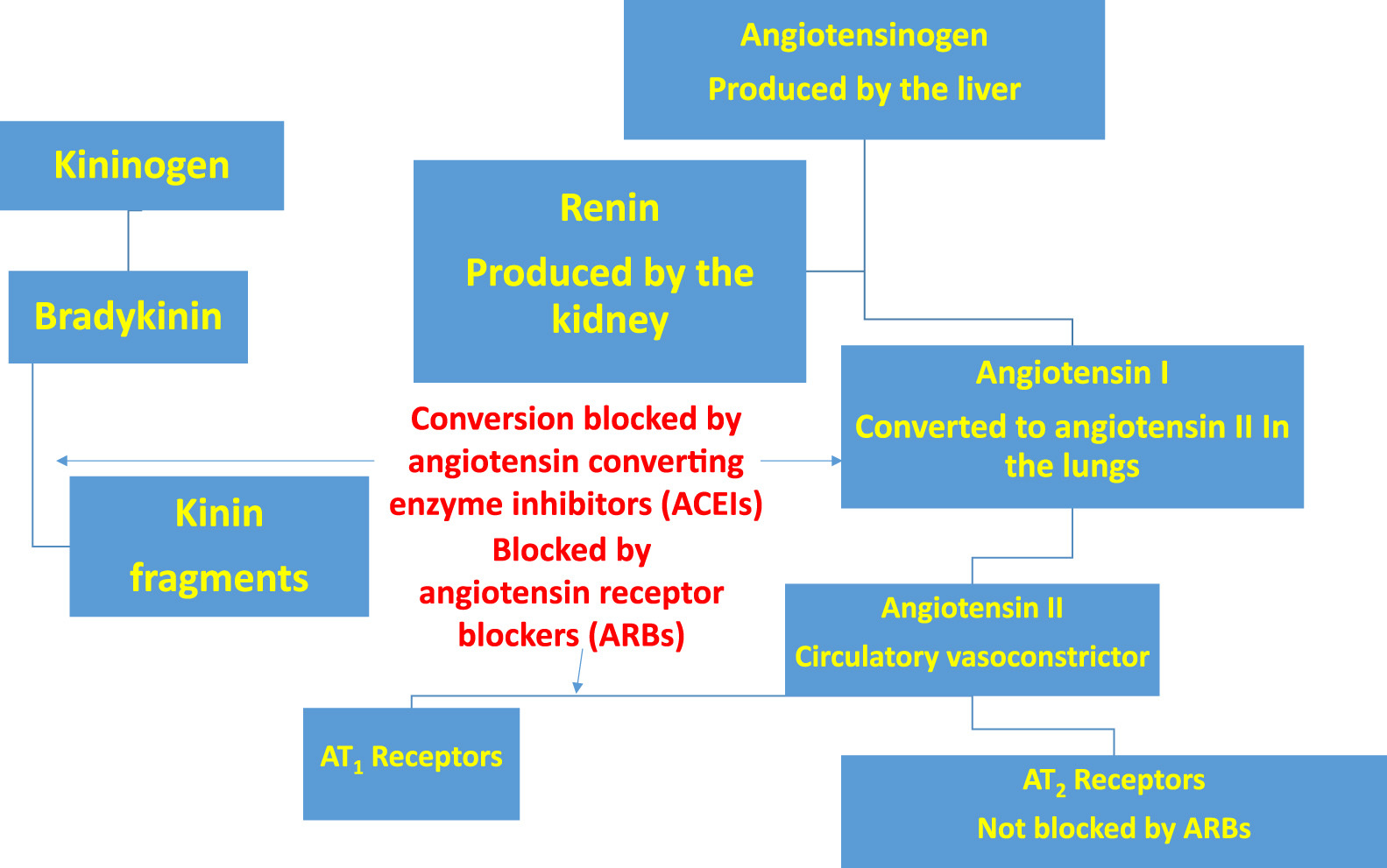
The mechanisms of action of the ACEIs and the ARBs on the renin-angiotensin pathway. ACEIs, angiotensin II-converting enzyme inhibitors; ARB, angiotensin receptor (AT1) blockers.
Although angioedema has now been reported in patients taking ARBs, primarily losartan, significant hymenopteran venom allergy has not been reported. 1 –3 I report a case of type I hypersensitivity reaction to a single southern yellow jacket (Vespula squamosa) sting in a previously nonallergic patient taking the ARB losartan for hypertension.
Case report
The author, a 67-year-old physician, was prescribed losartan, 10 mg orally daily, as initial therapy for essential hypertension. He was in excellent health otherwise. He reported no known allergies and, as an avid outdoorsman, had been stung repeatedly in the past by bees and wasps, including yellow jacket wasps, without significant reactions.
The patient was walking down an outdoor staircase when he placed his right hand on top of a resting southern yellow jacket worker that he had not noticed (Figure 2). He was stung 1 time on the right thenar eminence. The stinger did not detach in the wound site, which became hot, painful, and intensely pruritic immediately. Within 4 hours, significant edema had developed in the right thumb, thenar eminence, and wrist, to such an extent that the patient could not close the watchband on his right wrist (Figures 3 and 4). After 4 days of treatment with diphenhydramine for itching, 25 mg orally every 6 hours, and ibuprofen for painful swelling, 400 mg orally every 6 hours, the edema resolved enough for the patient to close his watchband on his right wrist.
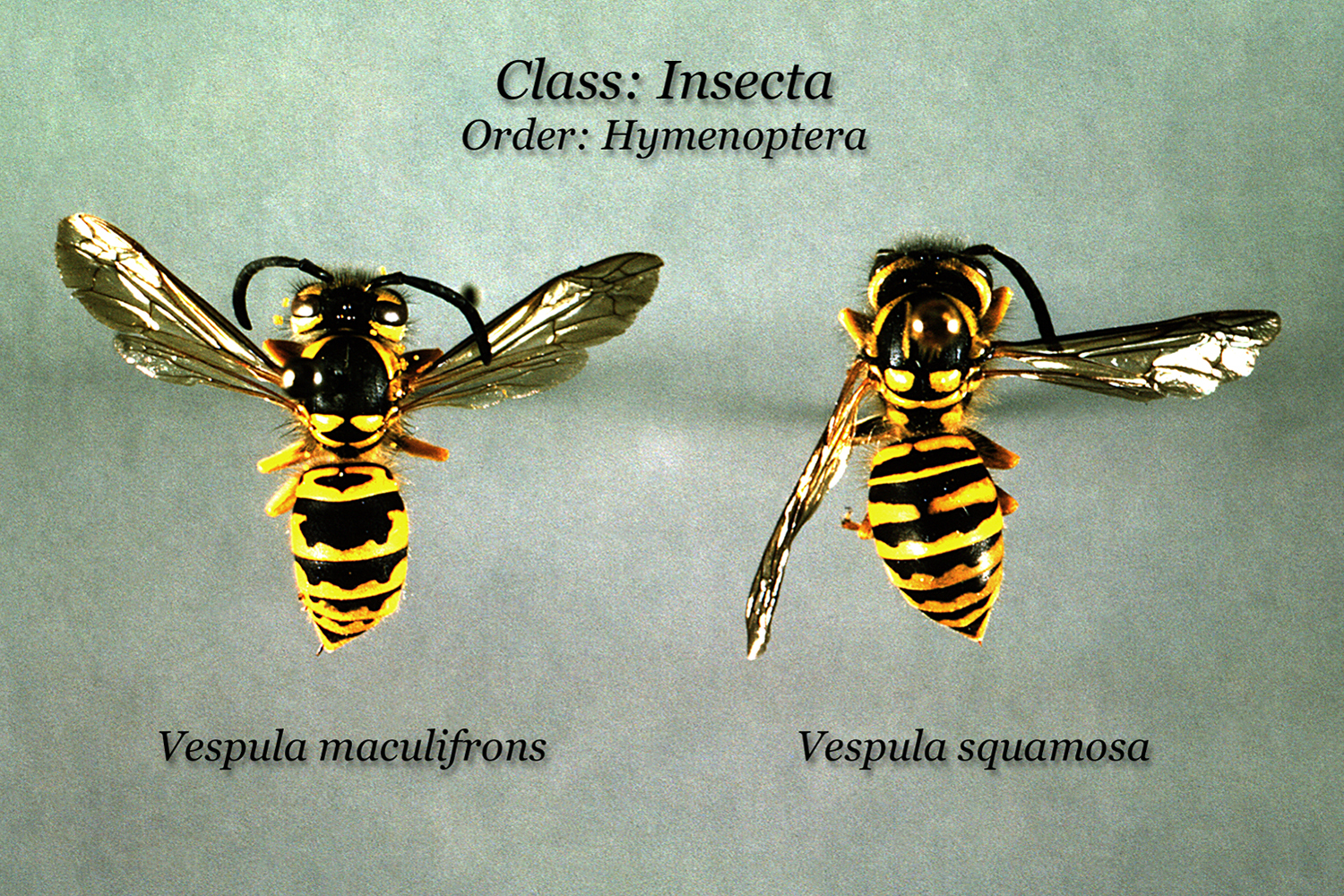
Yellow jacket wasp workers. Common species of yellow jacket wasp workers in the southeastern United States include the eastern yellow jacket, Vespula maculifrons (left), and the southern yellow jacket, Vespula squamosa (right). The worker wasps are all females, are equipped with modified ovipositors or stingers, and can sting repeatedly. Yellow jacket nests can be very large and are typically concealed underground in hollow logs, tree stumps, and soil cavities. Source: US Centers for Disease Control and Prevention, Public Health Image Library (PHIL), PHIL ID # 6340. Photographer, Dr. Pratt, CDC. (Public domain).

Type I hypersensitivity reaction 4 hours after a yellow jacket sting on the right thenar eminence. Significant edema developed in the right thumb, thenar eminence, and flexor surface of the wrist to such an extent that the author could not close the watchband on his right wrist. The swelling of the flexor surface of the right wrist hid the superficial wrist veins. Source: Author’s personal photograph.

The dorsal aspects of both hands with swelling and redness of the right hand dorsum and wrist four hours after a yellow jacket sting on the right thenar eminence in a previously nonallergic patient taking the angiotensin II receptor blocker losartan for hypertension. The swelling on the radial side of the dorsum of the right hand hid the superficial hand veins. Source: Author’s personal photograph.
Discussion
Although hypersensitivity reactions to hymenopteran stings have been reported in patients taking ACEIs, this case was the first to demonstrate a type I hypersensitivity reaction to hymenopteran venom in a patient taking the ARB losartan. Unlike the ACEIs, the ARBs were designed to inhibit only angiotensin II receptors and not enzymes, such as angiotensin converting enzyme and kinases. However, the hypersensitivity reaction described in this case shows that ARBs can also inhibit the enzymatic degradation of bradykinin.
With the full onset of the allergic response manifesting within 4 hours of envenomation, the resulting reaction in this case met the case definition for a delayed type I hypersensitivity reaction. Type I hypersensitivity reactions may occur within minutes of an antigenic challenge, such as a bee or wasp sting, and result in systemic anaphylaxis. Alternatively, the full effect of type I hypersensitivity reactions may be delayed by hours and cause local inflammatory responses, as in allergic rhinoconjunctivitis. Type I reactions are mediated by immunoglobulin E antibodies produced by B-lymphocytes in response to antigenic venoms that attach to and sensitize basophils and mast cells to degranulate and release their vasoactive chemical mediators, including histamine, leukotriene, and prostaglandins.
Hymenopteran stings, primarily by bees and wasps, account for more annual deaths in the United States than any other envenomation. 5 Many people who engage in outdoor occupations, including arborists, beekeepers, carpenters, heavy equipment operators, farmers, outdoor guides, landscapers, nurserymen, painters, and roofers, are predisposed to hymenopteran stings and potential hypersensitivity reactions. 5 Other preexisting risk factors for hymenopteran venom allergies include atopic history, severity of preceding immunologic reactions, mastocytosis or increased baseline mast cell numbers, increased serum tryptase concentrations, and antihypertensive therapy with ACEIs.5,6 Mastocytosis is a very rare disease characterized by increased numbers of mast cell in the skin, lungs, and other organs and increased mast cell secretory activity as reflected by elevated baseline serum tryptase concentrations. 6
In conclusion, antihypertensive therapy with ARBs may increase the risk of allergic reactions to hymenopteran stings via a mechanism that is similar to that of the ACEIs. Patients who manifest angioedema or hymenopteran venom allergy during ACEI therapy should probably not be treated with ARBs. 1 ACEI and ARB therapy should be discontinued, at least temporarily, in patients undergoing venom immunotherapy for hymenopteran venom allergy to prevent any adverse reactions during venom injections. 4
Acknowledgment: Support provided by departmental and institutional sources only.