
Abstract
Adequate management of wounds requires numerous interventions, one of which is the appropriate use of antimicrobials to attempt to minimize the risk of excess morbidity or mortality without increasing toxicity or multidrug resistant bacterial acquisition. There are numerous recommendations and opinions for not only the use of systemic prophylactic antimicrobials, but also the agent, dose, route, and duration. To best address the implementation of systemic antimicrobials in a field scenario, one must weigh the factors that go into that decision and then determine the best agents possible. The epidemiologic triangle (ie, the host, the agent, and the environment) forms the basis for selecting the correct prophylactic antibiotic for field wound care. Extreme conditions can be encountered in both military and nonmilitary systems, requiring a unique selection process to make the right antibiotic choice. A modifiable weighted matrix, recommended previously for point of injury combat casualty care, assists in selecting the best oral and intravenous/intramuscular agent based on the epidemiologic risk determination.
Introduction
A cornerstone of infectious disease is the epidemiologic triangle, which consists of the interactions between the host (the who), the agent (the what), and the environment (the where) (Figure). Host factors are intrinsic risk factors that include the individual’s exposure, susceptibility, and response to the causative agent. Factors such as hygiene, nutritional or immunologic status, anatomic structure, presence of disease, and medication all play roles. The agent includes the microorganism that is not only present but also causes disease. The virulence and pathogenicity of the microorganism, along with inoculum, influence the infection rate. The environment includes extrinsic factors such as climate, sanitation, supplies, and availability of health services. The interaction of elements in the epidemiologic triangle provides a framework to assess the myriad issues that ultimately stratify a wound’s potential for infection, the identity of the microorganism, and potential outcomes. Understanding these interactions enables one to determine the best management options for field wound care to optimize outcomes.
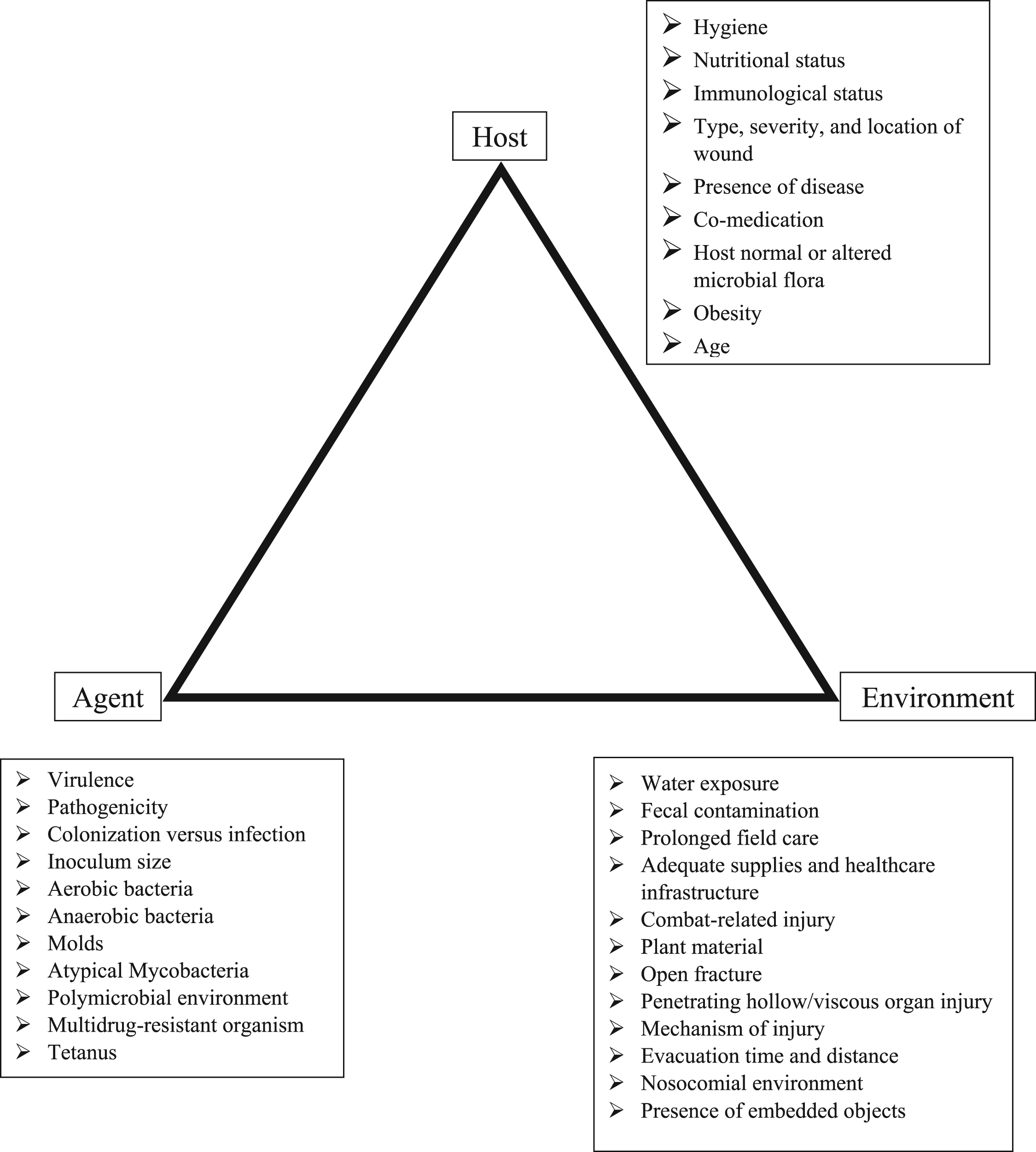
Epidemiologic triangle of the host, agent, and environment that leads to wound infection. 89
Many of the fundamentals of wound management as described in Homer’s The Iliad (∼900 BC) are still used today: Mechanically debride with removal of arrow, irrigate with water or wine, cover wound with bandage soaked in wine, apply analgesic, and apply styptic herbal drugs. 1
Clinical practice guidelines have been provided by the Infectious Disease Society of America (IDSA), the Wilderness Medical Society (WMS), the National Park Service (NPS), the International Committee of the Red Cross (ICRC), World Health Organization (WHO), and combat-related injury infections and tactical combat casualty care military committees (CoTCCC). 2 –9 Interventions recommended include wound irrigation and debridement, immunization for rabies and tetanus, wound preparation and closure, bandaging, stabilization, prophylactic topical or systemic antimicrobial therapy, and close clinical monitoring for signs or symptoms of infection. At the core of wound care during field conditions are the challenges associated with the extremes of the epidemiologic triangle, including poor hygiene, lack of supplies, and prolonged field care, among other extremes at the host, agent, or environment level.
This review will provide an overview of the incidence of traumatic wounds and infection rates, followed by examples of the epidemiologic triangle that influence wound infections. Antimicrobial options will then be provided, proposing a modifiable weighted matrix approach to assist determination of the ideal prophylactic antibiotic for field wounds. Overall emphasis is placed on extremity wounds and Food and Drug Administration (FDA)-approved antibiotics.
Traumatic wounds
Understanding the rates of traumatic wounds in austere settings is important in determining the ultimate need of field wound care and antimicrobial selection. During the spring climbing season of Mount Everest between 2003 and 2012, physicians in the clinical treatment area treated 2941 patients with 3569 diagnoses, of which 500 (14%) were trauma. 10 Lacerations comprised 21% of the trauma cases, with cellulitis in 21 cases and abscesses in 25 cases, but only 2 tibial/fibular fractures and 1 pelvic fracture. Search and rescue for 239 persons in the Adirondack Park in New York had soft tissue and skeletal systems as the most commonly reported traumatic injuries, with 98 (49%) and 56 (28%) reported, respectively. 11 Of 100,000 outdoor recreational injuries, 14.8% were lacerations. 12 Another study noted 4% of wilderness or outdoor activities were injuries to the skin or infection, with infection rates of 0.02–0.04 per 1000 participant days. 13 During a 10-day adventure race, there were 286 presentations for skin and soft tissue issues, of which avulsions/lacerations occurred in 2% of cases (n=9). 14 Differences in rates of trauma were also reported for urban versus rural expeditions, earthquakes, tsunamis, deserts, and flood-associated environments. 15 –21 Overall, wound infection rates vary but typically are reported at the 1% to 10% rate, based upon many factors. 22 Specific infections such as abscesses, necrotizing fasciitis, bacteremia, and endocarditis are rare but are reported, especially based upon mechanism of injury. 23
Among traumatic wounds to the extremities, open fractures are recognized as having a high potential for soft tissue infections and ultimately osteomyelitis. Gustilo and Anderson classified open fractures into 3 types with associated infection rates. 24 Type I fractures are defined as those with a laceration of less than 1 cm with minimal soft tissue damage and no gross contamination (0–2% infection rate). Type II fractures have lacerations of greater than 1 cm with moderate soft tissue damage (2–5% infection rate). Type III fractures are high-energy injuries, typically with bone comminution or loss. Type III fractures have 3 subtypes: IIIa, characterized by extensive soft tissue injury but with adequate soft tissue coverage (5–10% infection rate); IIIb, which includes extensive soft tissue injury along with bone exposure requiring soft tissue coverage (10–50% infection rate); and IIIc, which has extensive soft tissue damage and the need for arterial repair (25–50% infection rate).25,26 Twice as many tibia injuries appear to result in infection compared with other extremities. Other extremity injuries such as human bites or animal bites to the hand also have high infection potential.3,27
In addition to extremity injuries, other traumatic injuries are associated with infectious complications that were reviewed by a panel of civilian and military experts to determine posttrauma antimicrobial prophylaxis.7,28 The rate of posttraumatic empyema after chest injuries varies from 2% to 25%, with recent series having an incidence less than 5%. 29 Postinjury infection following penetrating abdominal injury ranges from 4% to 31%. 29
Civilian and military literature has reported varying rates of infections after central nervous system injury, with a military study describing 408 patients with closed or penetrating head trauma evaluated and managed at Walter Reed Army Medical Center or National Naval Medical Center in Bethesda, MD.30,31 There was a 9% rate of meningitis, with a rate of 26% in patients who had concomitant cerebrospinal fluid leakage from nose, ear, or wound. A recent meta-analysis of eye, maxillofacial, and neck injuries described combat injury incidences of 8% to 20% for the face, 2% to 11% for the neck, and 0.5% to 13% for the eye and periocular structures, with variable infection rates. 32
Burns comprised approximately 5% of injuries, especially early during the Iraq War, with infections being the primary cause of mortality. 33 Although combat-related injuries are the extremes of injury patterns, they allow for risk stratification of types of wounds that might benefit from early empiric antimicrobial therapy. Within combat, infections are a major issue with many lessons learned, but one must be cautious in making generalizations with the knowledge that military trauma has extremes of injury mechanism combined with higher rates of penetrating trauma. 34
The host
Injury patterns and individual patient risk factors are associated with infections. Among 3957 patients with lacerations in community and urban teaching hospitals, the infection rate did not differ. 35 Comorbid conditions such as diabetes mellitus are associated with increased rates of infection. 35 Massive trauma and large-volume blood transfusions are increasingly being recognized as markers of relative immunosuppression.36,37
Wound characteristics themselves are also associated with infectious complications. For example, lacerations to the lower extremities, grossly contaminated lacerations, and lacerations greater than 5 cm are more likely to become infected.35,38 Degrees of fracture as described above are risk factors for infection, along with hollow organ-penetrating injury. Contamination can occur through not only hollow organ penetration or rupture but also through host skin colonization and the environment. Methicillin-susceptible and methicillin-resistant Staphylococcus aureus (MSSA and MRSA, respectively) colonize humans approximately 25% and 3% of the time, respectively. 39 In addition, there have been increasing reports of skin and gastrointestinal tract colonization by gram-negative bacteria in healthy individuals. These include multidrug-resistant species, especially extended-spectrum, beta-lactamase-producing Enterobacteriaceae such as Escherichia coli and Klebsiella species.40,41
The agent
The complex interplay between the virulence and pathogenicity of a microorganism plays a central role in its ability to colonize and infect a wound. This interplay must be understood because it influences the selection of antimicrobials. The microorganisms most frequently associated with wound infections, regardless of the mechanism of injury and the environment, are the common skin pathogens S aureus and Streptococcus pyogenes.
However, other pathogens are also encountered based upon a number of parameters, so risk factors for their isolation should be sought by the clinician. For example, during World War I and World War II in Europe, wounds that were heavily contaminated with fertile soil and associated with prolonged evacuation times saw increased recovery of Clostridium species, Streptococcus species, Staphylococci species, and coliform bacilli.1,5 Of note, many wound-associated pathogens during the wars in Iraq and Afghanistan saw a shift from Acinetobacter to other gram-negative rods with multidrug-resistance to Enterobacteriaceae (eg, E coli, Klebsiella species) with extended-spectrum beta-lactamase production and Enterococcus.36,42 Evidence supports Acinetobacter as a nosocomial pathogen, rather than inoculation at the time of injury in Iraq.
Cultures from fresh wounds at the time of injury from Vietnam revealed an even mix of gram-positive and gram-negative bacteria, including coagulase negative staphylococci (CNS), Bacillus subtillis, and Enterobacter group. 43 After 5 days of therapy and antimicrobials, 84% of wounds grew gram-negative bacteria, primarily Pseudomonas aeruginosa. As is often the issue with many of these studies, initial anaerobic and fungal cultures were not obtained. In Iraq, a study of 61 fresh wounds revealed 32 CNS, 4 S aureus (2 of those MRSA), as well as Pseudomonas stutzeri, C meningosepticum, and E coli, but no multidrug-resistant gram-negative bacteria. 44 In a study of 14 mangled extremity wounds in Afghanistan, immediate culture revealed colonization with low-virulence, environmental, gram-negative bacteria, reflecting wound contamination. These isolates were not associated with subsequent infection. 45
A study of 213 open tibia injuries revealed that 27% were complicated by a deep infection. Of 145 surveillance cultures, Acinetobacter was recovered 61% of the time; Enterobacter cloacae 18%; and K pneumoniae, E faecium, and P aeruginosa each at 14%. 46 Of those tibias that became infected, S aureus was isolated in 35%, with Acinetobacter and CNS in 20%, K pneumoniae in 12%, and E faecium in 8%.
It is still important to know that nosocomial infection greatly influences these pathogens. Other pathogens associated with wound infections include obligate anaerobes, which were common during World War II but rarely seen during the wars in Iraq and Afghanistan. This is likely reflective of improvements in wound care, including early surgical intervention, delayed primary closure, differences in soil pathogens from Europe vs desert or mountainous regions, and possibly antimicrobial coverage. 47 Tetanus is rarely seen now for similar reasons. 34 Low-virulence pathogens like mycobacteria and fungi have rarely been described. 48 –50 Although Clostridium species and S pyogenes were seen less commonly during in Iraq and Afghanistan compared with prior wars, there was the trend toward increasing resistance, likely reflective of nosocomial infections.
Other unique exposures that affect the microbiology of wound infections should be noted. Dog and cat bites are associated not only with the typical pathogens of Streptococcus and Staphylococcus species but also gram-negative bacteria (to a lesser degree) and some unique, and potentially invasive, organisms, including Pasteurella multocida, Capnocytophaga canimorsus, and Weeksella zoohelcum. 27 Anaerobic bacteria include Fusobacterium, Bacteroides, Porphyromonas, and Prevotella species. Human bites and closed fist injuries are typically contaminated with Eikenella corrodens, S aureus, S pyogenes, and anaerobic bacteria. 51 Burn wounds experience a transition in bacteria over time, reflective initially of skin colonization and eventually the nosocomial environment, as shown with Acinetobacter. 52
Although very complicated and incompletely understood, pathogenesis, virulence, antimicrobial resistance, and inoculum effect are important aspects in the establishment of infection and therapy. 53 –55 This is likely reflective of why S aureus is commonly associated with infections, especially osteomyelitis, and why heavily contaminated wounds have higher rates of infection, especially with delayed therapy.
The environment
The environment influences many aspects of wound field care, including type of pathogens inoculated into the wound, care available based upon remote conditions, prolonged evacuation times, and supply limitations. Although the infecting pathogens are most commonly from the patient’s own skin flora being inoculated into the wounds, one must not minimize the importance of microorganisms in the environment.
Injuries associated with water exposure have increased rates of gram-negative pathogens, as evidenced by the tsunami in 2004. Most wounds were polymicrobial, including Aeromonas species, E coli, K pneumoniae, S aureus, Proteus vulgaris, and P aeruginosa. Anaerobic cultures were rarely performed to determine their role, but they were not associated with established infection on further monitoring.38,56 Most infections occurred 2–3 days after injury. Antimicrobial therapy within 1 day of the tsunami appeared to be protective. Higher rates of S aureus, Acinetobacter, and Enterococcus were reported after an earthquake in 2008 in China. These differences could reflect nosocomial or regional differences in host colonization or inoculation from the environment. 16 After the tsunami, other atypical infections were noted, including rapidly growing mycobacteria late after injury (3–11 months) along with other atypical pathogens that were noted early during initial wound management near the time of injury, such as Burkholderia pseudomallei and Cladophilaphora bantiana. 57
In addition to the above reports, marine and freshwater pathogens that have been described include Vibrio species, Aeromonas hydrophila, and other atypical pathogens like Plesiomonas species, Mycobacterium marinum, and Erysipelothrix rhusiopathiae. 58 Of note, other injuries have similar microbiology, including those sustained in boating accidents; propeller-related injuries; shark bites; and injuries related to alligators, crocodiles, barracuda, and moray eels. In addition, regional differences have been reported: V vulnificus in the Gulf of Mexico, Chromobacterium violaceiuim in the Western Pacific, and Shewanella species infections in the Mediterranean and Western Pacific. 19
Other distinct pathogens include environmental molds, which have been reported in natural disasters including tornadoes, hurricanes, earthquakes, and volcano eruptions and are reported to be associated with high mortality. 59 Invasive mold infections show the overlapping influence of the host, pathogen, and environment. During the war in Afghanistan, mold infections were associated with dismounted complex blast injuries in Helmand and Kandahar Provinces with high-level amputations and perineal injuries in patients requiring massive blood product support.49,60 In addition to geography, seasonality can also affect pathogen isolation. 1 During the Korean War, Clostridium, Streptococci, and Staphylococci were most commonly isolated in the winter months, compared with fecal coliforms in the summer. 1
Because the environment and access to care can affect timing of interventions, this can affect infection rates. Ongoing debate surrounds time to closure, with a report comparing closure before or after 12 hours showing no statistically different infection rate. 35 In addition, use of antibiotics along with aggressive debridement with primary suture appeared successful in many cases, but clinical follow-up of patient outcomes is unclear.38,61
Another issue is related to timing of antimicrobial administration, especially as it relates to early versus delayed surgical care. The combat-related injury working groups extensively reviewed this in their publications in 2008 and 2011.25,26 Studies supporting the protective role of antimicrobials within 3 hours of injury include the 1973 October War in Israel, the Falklands Campaign in 1982, the British military experience in Afghanistan, and civilian studies. A study examining the efficacy of point of injury antimicrobials by the US Army Rangers did not show decreased rates of infection, but reassuringly also did not show increased rates of multidrug-resistant colonization. 62 However, the study was limited by the low use of point-of-injury antimicrobials, likely reflective of inadequate training.
Two recent orthopedic surgery articles of severe open fractures reported conflicting outcomes of the effect of early antibiotics on rates of infection.63,64 Open fracture models in animals indicate the combination of early surgery and antimicrobials (within 2 hours for both) is key for preventing infection. 65 If antimicrobials are given within 2 hours and surgery is delayed 6 hours, there is an increased rate of infection; however, if surgery occurs within 2 hours but antimicrobials are delayed 6 hours, even higher rates of infection are noted. In animal models, other data indicate that although wounds take 3 days to develop clinical evidence of infection, therapy is ineffective if delayed 6 hours. 66 Overall inoculum effect (ie, dose of bacteria) is also able to override the impact of antimicrobials. Other animal models using weapons of various calibers revealed similar findings: Earlier antimicrobial exposure (1–2 hours compared with 6 hours postinjury) is associated with decreased infection rates. 67 Similar studies also revealed that penicillin was associated with less devitalized tissue in the wound, with an effect that may last 12 hours or more.68,69 As such, antimicrobial therapy is likely useful if surgery is delayed, but it is not a substitute for surgery, and increased bacterial load can possibly override the beneficial effect of antimicrobials, especially if blood flow to an area is limited by severity of injury or shock.
Antimicrobial weighted matrix
Foundational to therapy is determining when benefits of systemic antimicrobials outweigh the associated risks: potential antimicrobial-resistance pressure, C difficile-associated diarrhea; allergic reactions; drug-specific toxicities, including cardiac, hepatic, renal, and hematopoietic; and drug interactions. It also must be understood that timely irrigation and debridement is paramount to successful wound management. Appropriate closure of open wounds, bandaging, and close follow-up are also key.
It has been recognized repeatedly over time that reliance on antimicrobial therapy instead of good wound debridement and irrigation leads to excess morbidity and mortality. During World War I, Alexander Fleming stated, “All the great success of primary wound treatment have been due to efficient surgery, and it seems a pity that the surgeon should wish to share his glory with a chemical antiseptic of more than doubtful utility.” 70 During World War II, topical sulfanilamide became part of the standard of care after a lecture series about its success was attended by a team of Army and Navy medical personnel stationed in Hawaii just 36 hours before the attack on Pearl Harbor. However, this reliance on sulfanilamide powder replaced appropriate debridement, which had to be corrected after increased rates of infection were noted. 71 During the Yom Kippur War, the overemphasis on antimicrobials led authors to state that “this leads towards the temptation to ‘sterilize’ the wound with massive doses of antibiotics and favors a false security with less reliance on good surgical technique.” 72 The ICRC states that “the best antibiotic is good surgery.” 5 As such, it is paramount to risk stratify the wound’s potential for infection based on parameters addressed by the epidemiologic triangle, along with access to appropriate wound care and surgical intervention, if need be.
Recommendations regarding antimicrobials include those by the IDSA, ICRC, WMS, NPS, CoTCCC, WHO, and combat-related injury infection prevention guidelines (Table 1). 73 In comparison, Israelis reportedly use moxifloxacin, ceftriaxone, cephalexin, and/or metronidazole, while the British recommend penicillin or amoxicillin/clavulanate for cases that include abdominal injuries. 74 –77 These recommendations are based on factors reflected within the epidemiologic triangle. The differences in choices are based on availability of supplies, evacuation chains, severity of injury, site of injury, and so on. As such, there is a difference between the benefits of point-of-injury antimicrobials for a severe open injury with prolonged evacuation to care and a minor injury with surgical care available in 20 minutes. Risk stratification for field care or point-of-injury antimicrobials must take into account many factors, including if the care is provided by a physician, a medic, or the person himself or herself; severity of the injury; and timely access to appropriate wound care.
Recommended antimicrobials for field care and combat-related or disaster-associated extremity wounds that could be delivered at the point of injury or during care with increased medical assets
IV, intravenous; po, by mouth; q, every; IM, intramuscularly; QID, 4 times a day; DPC, delayed primary closure; TID, 3 times a day; CoTCCC, Committee on Tactical Combat Casualty Care.
If no dose or interval provided then it was not provided in the recommendation.
The key to the right antimicrobial in field care is simplicity of use, ease of transport and storage, reconstitution, administration, safety, duration of activity, spectrum of activity, and cost for the field environment (Table 2). This is typically maximized by an oral agent. The NPS and the CoTCCC recommend an oral fluoroquinolone for initial injury as part of a pill pack carried by the patients themselves. The NPS and the CoTCCC do not outline the indications for the antimicrobials. The combat-related injury infection guideline committee recommended in their 2008 and 2011 publications to provide point-of-injury antimicrobials if evacuation is delayed or not expected for more than 3 hours.7,78 The difference between the the TCCC and combat-related injury infection guidelines are recommendations for levofloxacin and moxifloxacin. Levofloxacin has better activity for gram-negative bacteria including P. aeruginosa and water pathogens, while moxifloxacin has no P. aeruginosa activity. 78 –81 Although moxifloxacin has more anaerobic activity than levofloxacin, it is associated with increasing rates of resistance to concerning intraabdominal bacteria, notably Bacteroides species. Both antimicrobials have adequate Streptococci and MSSA activity with some MRSA activity. Recently, the FDA has recommended against the use of even short-course fluoroquinolones, especially for sinusitis, bronchitis, and uncomplicated urinary tract infections, which have other treatment options. This is due to disabling and potentially permanent, serious side effects that can occur together. These adverse events can involve the tendons, muscles, joints, nerves, and central nervous system. Other oral agents such as penicillin, doxycycline, amoxicillin/clavulanate, ciprofloxacin, and cephalosporins have either inadequate coverage, are administered multiple times a day, or have adverse event profiles that limit their utility. Increasing multidrug-resistant bacteria present through environmental contamination and host colonization might increase the future need for broader coverage, but this is not the case with perioperative antibiotics yet.
Characterization of prophylactic antimicrobial agents for field wound care
Oral levofloxacin 750 mg po per day $0.275/day, moxifloxacin 400 mg po per day $2.23/day, amoxicillin/clavulanate 875 mg BID $0.264/day.
IV ampicillin/sulbactam coverage is the same as po amoxicillin/clavulanate.
DoD costs as of June 15, 2016.
IV, intravenous; IM, intramuscular; po, by mouth; BID, twice a day; DoD, Department of Defense.
The NPS recommends intravenous (IV) cefazolin for severe wounds (deep, crush, exposed tendon, heavy contamination, or open fracture) with an expected time from injury to definitive care of >3 hours, unless the injury is a burn, a shallow wound (ie, not through all layers of the skin), or wounds where the expected transport to definitive care is <1 hour (Table 1). The CoTCCC currently recommends intravenous/intramuscular (IV/IM) therapy with cefotetan or ertapenem for shock and for unconscious patients, with previous indications including abdominal injury for point-of-injury care. Other agents are recommended by various organizations for intraabdominal, chest, and central nervous system injury in addition to extremity wound injures when the patient reaches definitive care (Table 1). 4 –6,9 A single dose of IV antibiotics, benzylpenicillin, to be given only if evacuation is going to be delayed, such that surgical intervention is not possible within 4 hours, is recommended by British Military experts in the field. 17 This is to minimize the risk of multidrug-resistant bacteria while still covering the pathogens of historical concern, including Streptococcus species and Clostridium non-difficile species.
Based on the Ranger point-of-injury antimicrobial data and results of the Trauma Infectious Disease Outcome Study that indicated no difference between rates of subsequent isolation of resistant-bacteria after broad- versus narrow-spectrum antimicrobial coverage at the time of injury, it is unclear that short-duration antimicrobial selection pressure leads to collateral prolonged damage within the trauma population (unpublished data). 62 It is important to note that the current regimens appear to modify the commonly encountered infections with Streptococcus species and Clostridium species that have directed field wound antimicrobials in the past. However, other factors may be involved, including differences in the environment of injury or host colonization, in contrast to other wars. 82 Gas gangrene resulted in 3 of 15 deaths among warfare-related limb injury in the Chinese military. 83 The Chinese also reported cases associated with Wenchuan earthquake victims. 84 A modifiable weighted matrix was previously published for the indications of various IV/IM medication, including ertapenem, for point-of-injury care in tactical combat casualty care to augment the CoTCCC recommendation of cefotetan (Table 3). 85 Since that publication, data support that ertapenem can be delivered with a 5-minute infusion. 86 Also, intraosseous and IM delivery of ertapenem appear to be adequate. 26 Use of ertapenem and cefotetan in colorectal surgeries has been compared, with better outcomes with ertapenem. 87 Overall, activity of ertapenem is enhanced in comparison to cefotetan for streptococcal, MSSA, gram-negative bacteria, and anaerobic bacteria. Although ertapenem has limited activity against P aeruginosa, versus none with cefotetan, ertapenem is not an agent recommended for P aeruginosa because of high resistance rates.
Modifiable weighted matrix system for determining ideal field care antibiotics (higher score is better) utilizing the risk by host, agent, and environment to modify the weighted item and importance
BID, twice a day; TID, three times a day; QID, four times a day; IV, intravenous; IM, intramuscular.
Dictated by expected potential pathogen bacteria based upon type of exposure.
A study in Iraq of the role of antimicrobials and irrigation, which included 53 wounds, noted the lowest infection rates (2.6%) with the combination of antibiotics and irrigation. Wounds that received no antimicrobial but were irrigated had a 17% infection rate. Those with antimicrobials and no irrigation had a 40% infection rate, and neither therapy resulted in a 70% infection rate. 88 The agents used were parenteral ceftriaxone and/or oral fluoroquinolones predominantly, followed by second-generation cephalosporins or amoxicillin/clavulanate. Antibiotic course duration ranged from 7 to 10 days. One has to be cautious in the application of this study results given the use of 10 days of antimicrobials because it implies ongoing infection and not wound colonization, as well as the small numbers evaluated. However, the findings are intriguing given the field nature of care.
An examination of the use of early cephalexin and metronidazole in 2001–2003 in Gaza City is reported for 109 patients who received initial oral antibiotics and wound management soon after injury (29±11 minutes, maximum 60 minutes) with strict exclusion criteria. 74 Eleven had an infection, although the type of bacteria was not reported. Of those 11, 2 had purulence requiring redebridement.
Conclusions
Ongoing analysis of point-of-injury antimicrobials on outcomes from Iraq and Afghanistan is needed, along with randomized studies to adequately address the pros and cons of the ideal field antimicrobial, indications, and duration. Until this is done, it is ideal to combine the epidemiologic triangle, reflecting the risk of the patient, and selection of the right antimicrobial for the field care scenario under consideration. Leading agents might include oral levofloxacin and IV/IM ertapenem, based on many variables within the epidemiologic triangle, before surgical intervention, especially for severe injuries with prolonged evacuation time.
Disclaimer: The views expressed are those of the author and do not necessarily reflect the official views of the US Army Office of the Surgeon General, the Department of Defense, or the Departments of the Army. Mention of trade names, commercial products, or organization does not imply endorsement by the US government.
Financial/Material Support: None.
Disclosures: None.
Footnotes
☆
Presented at the Tactical Combat Casualty Care: Transitioning Battlefield Lessons Learned to Other Austere Environments Preconference to the Seventh World Congress of Mountain & Wilderness Medicine, Telluride, Colorado, July 30–31, 2016.