
Abstract
Objective
Hamate hook fractures are rare injuries, comprising 2% to 4% of all carpal fractures. Climbing athletes seem to be affected more frequently than others, as they strain the passive and active anatomical structures of their hands and fingers to maximum capacity during training or competing. This stress is transmitted to the hook of the hamate by tightened flexor tendons, which creates high contact pressure to the ulnar margin of the carpal tunnel. Injuries of the hamate hook, caused by contact pressure of the anatomical structures, are rare and occur nearly exclusively during climbing.
Methods
We diagnosed 12 athletes with hamate hook fractures who presented with diffuse pain in the wrist joint, which occurred either during or after climbing. Radiographs or computed tomography revealed fractures in the hamate bones in most of the patients; therapy consisted of consequent stress reduction.
Results
Follow-up investigations found that all athletes were free of symptoms after 10.7 ± 5.1 (6–24) (mean ± standard deviation with range) weeks. Resection of the hamate hook was necessary in 3 patients. All patients regained their preinjury climbing level.
Conclusion
Climbers with an unspecific, diffuse pain in the wrist need to be examined by radiograph and
Introduction
Hamate fractures due to sports are usually caused by repetitive direct trauma (eg, during mountain biking [direct impulse from the handle bars] or from a direct hit through a grasped object [baseball bat or golf club]). 1 –4 Direct impact to the hamate bone is rare during rock climbing; tightened flexor tendons create high contact pressure on the hamate, especially the hamate hook. 1 In our center, we currently see hamate fractures more frequently than in the past, and they seem to be an important differential diagnosis for wrist and carpal pain in rock climbing athletes. 1
Hamate fractures are grouped according to Milch’s classification, which separates fractures into 2 main groups (Figure 1). Type I fractures affect the hamate hook, whereas type II fractures are located within the body of the hamate. 3 ,5,6 Further classification according to the location of the fracture within the hamate body is described by Hirano et al. 6 Hamate hook fractures can also be subclassified according to Xiong et al 3 : type I(I) fractures are avulsion fractures at the tip of the hook, type I(II) represents fractures in the middle of the hook, and type I(III) fractures are located at the base of the hook (Figure 1). 2 ,3,6
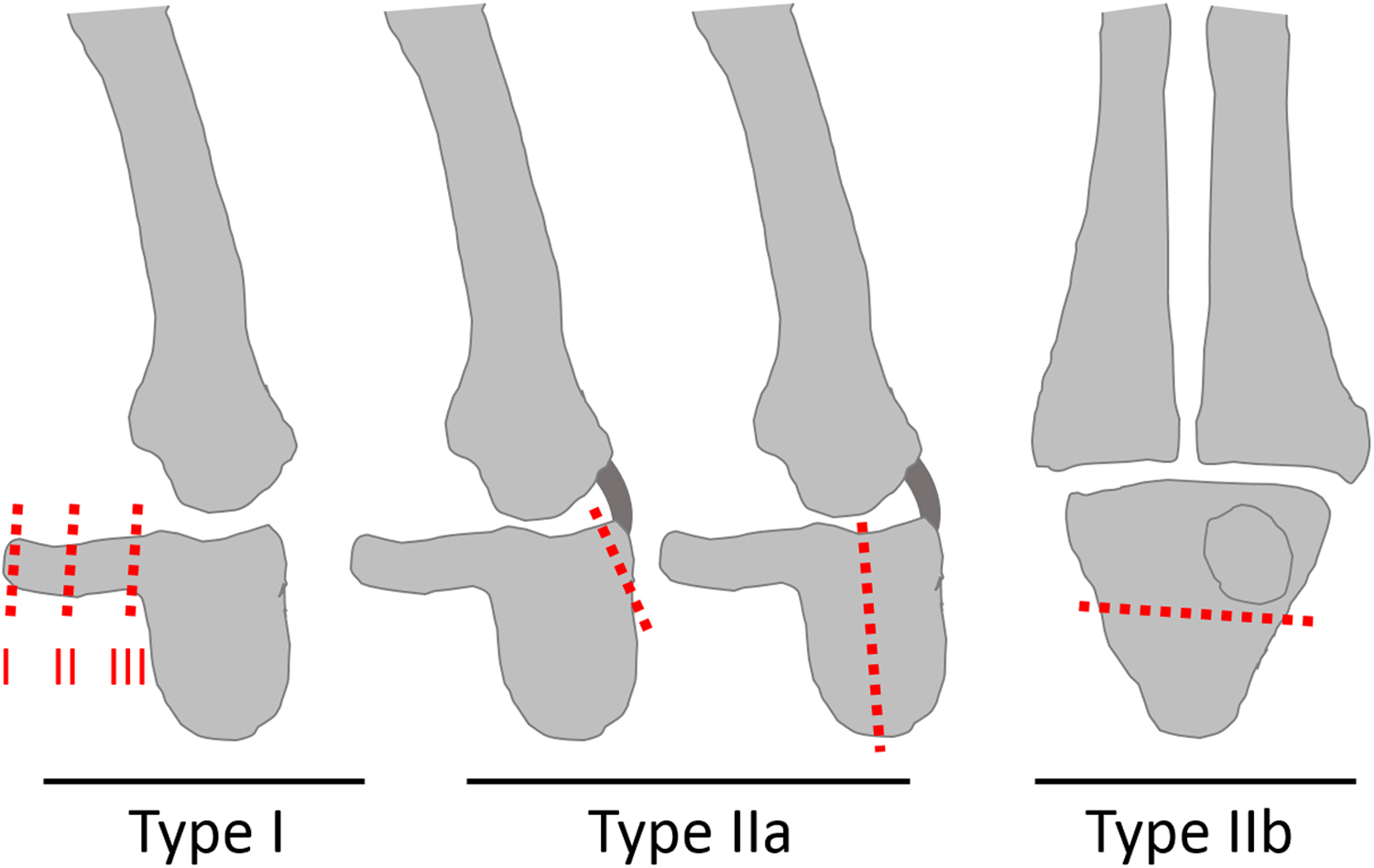
Milch’s classification of hamate fractures Type I: hamate hook fractures. Type IIa: coronal hamate body fractures. Type IIb: transversal hamate body fractures. Hamate hook fractures can be subclassified according to Xiong et al: Type I(I) fractures are avulsion fractures at the tip of the hook. Type I(II) represent fractures in the middle part of the hook. Type I(III) are fractures at the base of the hook. Modified from Hirano et al and Xiong et al. 2 ,3,5,6
Several publications recommend surgical treatment of hamate fractures with resection of the hamate hook. 3 ,6,7 As the hamate hook is the main deflection pulley for flexor tendons of the digitorum IV/V flexor muscles, we focused on a conservative approach in order to avoid any loss of strength in rock climbing athletes.
Materials and Methods
For this case series, we investigated 12, mostly high-level, rock climbers with diffuse ulnar-sided pain in the wrist between 2009 and 2015 (Tables 1 and 2). All patients were seen and treated in the outpatient clinics of the referral centers for climbing-related injuries in Germany and Switzerland. The inclusion criterion was severe climbing-related pain over the hamate hook without trauma. The study was approved by the institutional review board, and all patients provided informed consent.
Hamate fractures in rock climbing athletes
CT, computed tomography.
UIAA metric scale.
Patient injury distribution 2009–2015
Values are mean ± standard deviation (range).
All athletes reported mild to moderate pain during relaxation and moderate to severe pain (numerical analogue pain scale) during climbing, forcing them to stop sport-specific activities. Exacerbation of pain was reported while performing the “undercling” position of the hand, a special climbing move in which the hand is in a supine and ulnar abducted position, leading to a high level of stress on the hamate hook (Figure 2). 1

“Side-undercling” position of the hand during indoor rock climbing. This position of the forearm and the hand is used during special climbing moves in which the hand is in a supine and ulnar abducted position, leading to a high stress level on the hamate hook.
In addition to palpation of the hamate hook, we used the hook of hamate pull test, a specific provocation test that causes a high level of stress on the hamate hook. An increase of pain under flexion of digitorum IV and V (musculus flexor digitorum profundus and musculus flexor digitorum superficialis) against resistance in a flexed and ulnar abducted wrist is pathognomic for hamate injuries. No pain is triggered in an extended and radial abducted position of the wrist with simultaneous flexion of the fingers against resistance. 8 Furthermore, movement of tendons (especially digitus IV and digitus V) was tested to avoid underdiagnoses of an impinged tendon within the fracture site (Figure 3). 9
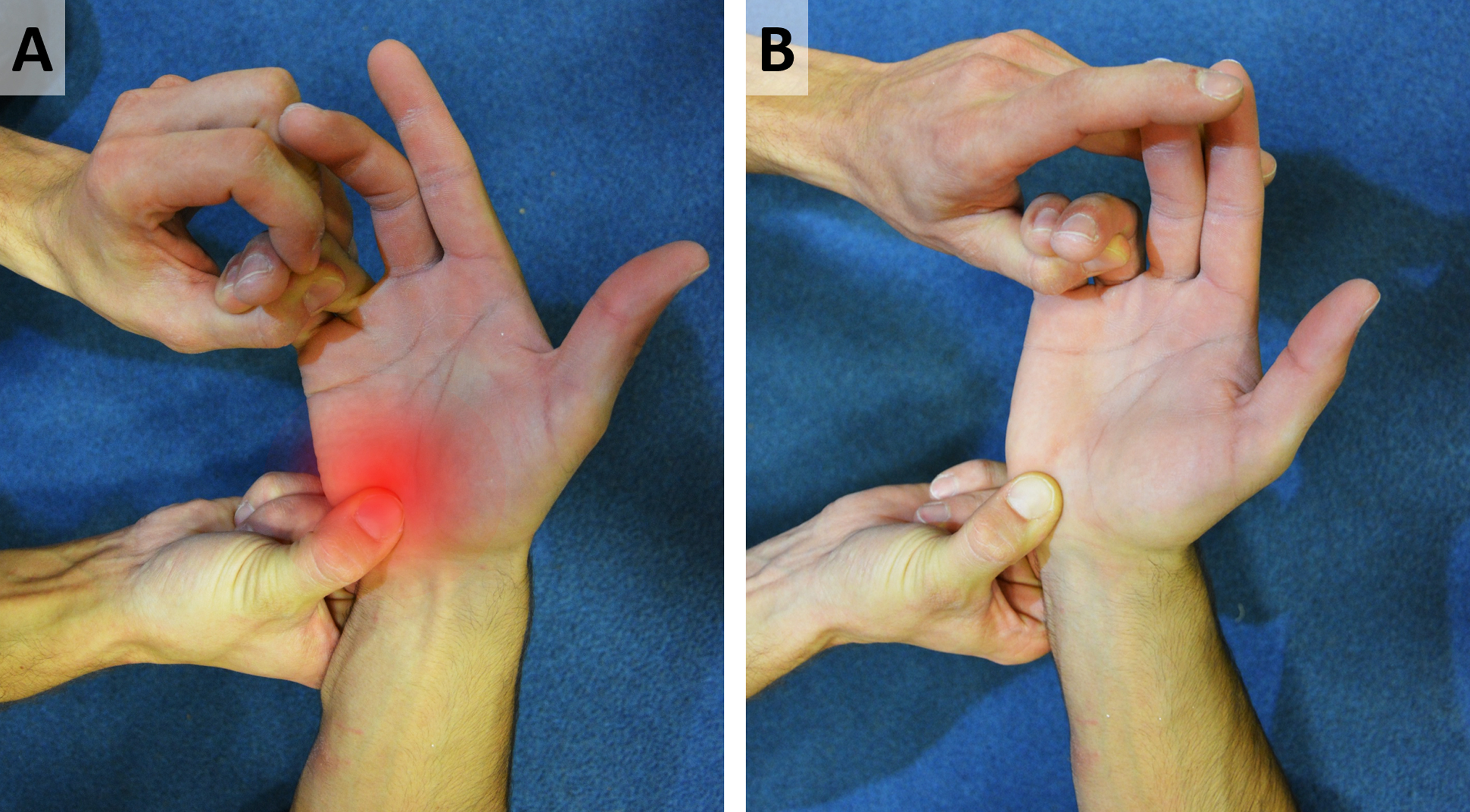
Investigation of the hamate hook in a rock climbing athlete. A, Provocation test leading to a high level of stress on the hamate hook. Pathognomonic for hamate injuries is increase of pain under flexion of digitorum IV and V against resistance in flexed and ulnar abducted wrist. B, No pain is triggered in extended and radial abducted position of the wrist with simultaneous flexion of the fingers against resistance.
Computed tomography (CT) or magnetic resonance imaging (MRI) (sagittal, axial, and coronary layers) were performed subsequently in 10 cases in which plain radiograph was nondiagnostic. If no clear fracture was detected but clinical examination revealed pain and liquid accumulation (detected by MRI) in the hamate hook, we interpreted this as an “insertions-ligamentopathy” of the flexor retinaculum.
All patients were advised to avoid training, and the fracture was treated with a cast for at least 6 weeks (7.3 ± 0.9, 6–8 weeks). Primary medical failure was defined as ongoing pain after 6 to 8 weeks of immobilization. Recommencement of training was performed with a stepwise gain of intensity in both the conservatively and the surgically treated athletes; training intensity, frequency, conception, and methodology were adapted to suit the individual athlete.
Statistical analyses
Microsoft Excel was used for collection of data; statistical analyses were performed using SigmaStat software (Systat Software Inc, San Jose, CA). Unless stated otherwise, data were expressed as mean ± standard deviation (range).
Results
Our patient population was all male, with an average age of 32 ± 7 (15–43) years. The average rock climbing history/experience was greater than 10 years, with an average climbing level of 9.9 (interquartile range = 1.3, 6.7–10.7; International Climbing and Mountaineering Federation [Union Internationale des Associations d’Alpinisme, or UIAA] metric scale) (Table 2). 10 All patients denied direct trauma to the palm or the wrist that could have resulted in a fracture and reported pain during or directly after high-performance climbing or bouldering. Ten athletes experienced a type I fracture of the hamate hook; none experienced a type II fracture. All fractures were detected in the hamate hook (Figures 4–7). Distribution of fracture locations within the hook (type 1(I–III), Figure 1) was balanced. Two patients were diagnosed with an insertions-ligamentopathy of the hamate hook, as fractures were not clearly detectable. Clinical examination of the patients with acute symptoms found local tenderness and ulnar-sided swelling of the wrist. Athletes with a longer history of symptoms only presented inconspicuous pressure pain over the hamate hook. All patients experienced restricted motion of the wrist due to painful pronation, supination, and ulnar/radial deviation.
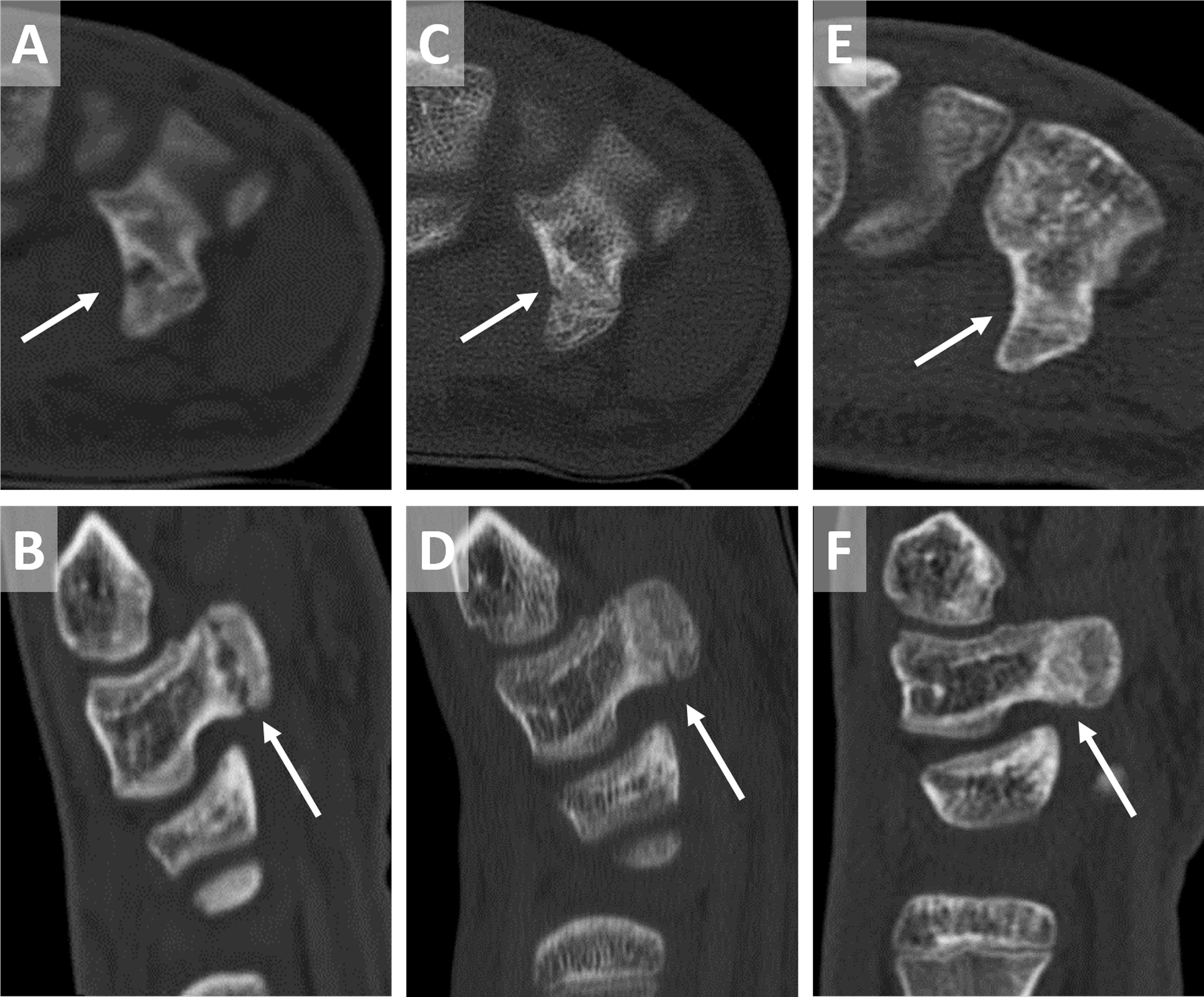
A 16-year-old rock climbing athlete with type I(II) fracture of the hamate hook. A, B, Refractured nonunion of a hamate fracture. C, D, Radiological healing after 6 weeks immobilization. E, F. Bony union after 12 weeks.
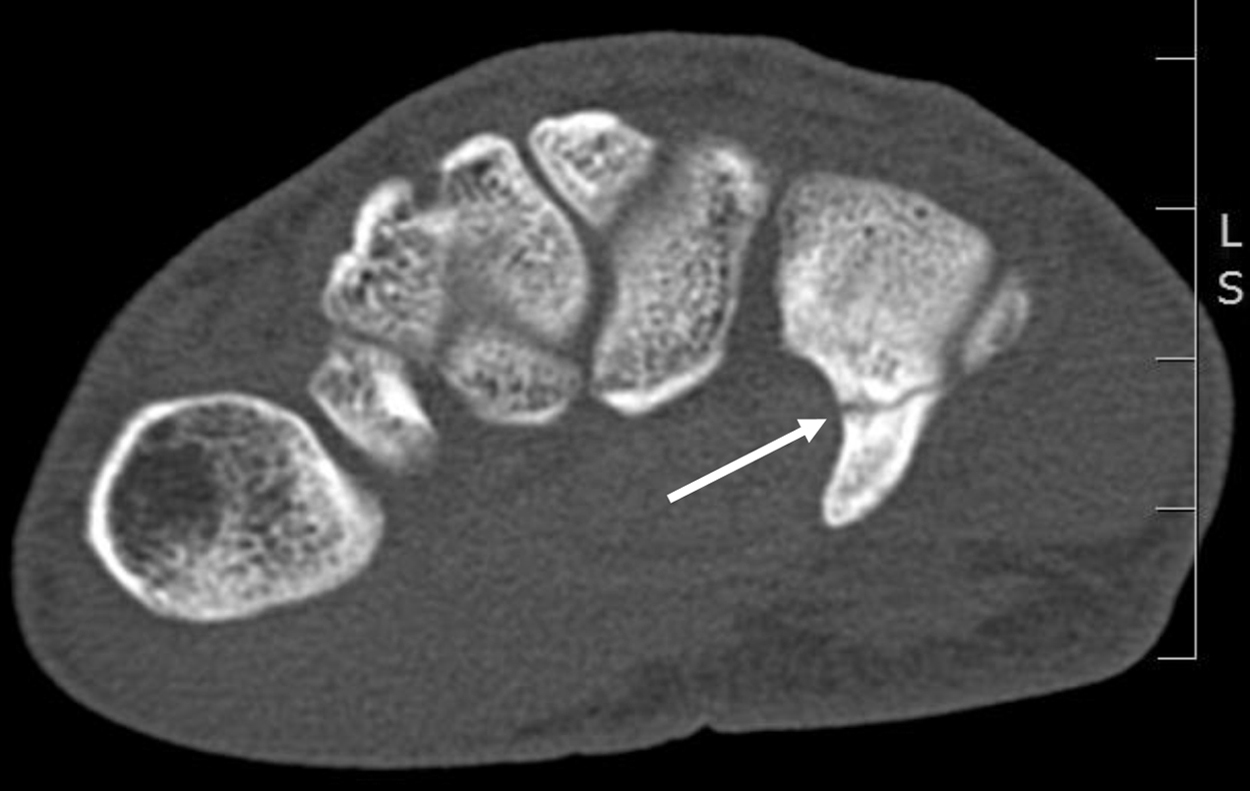
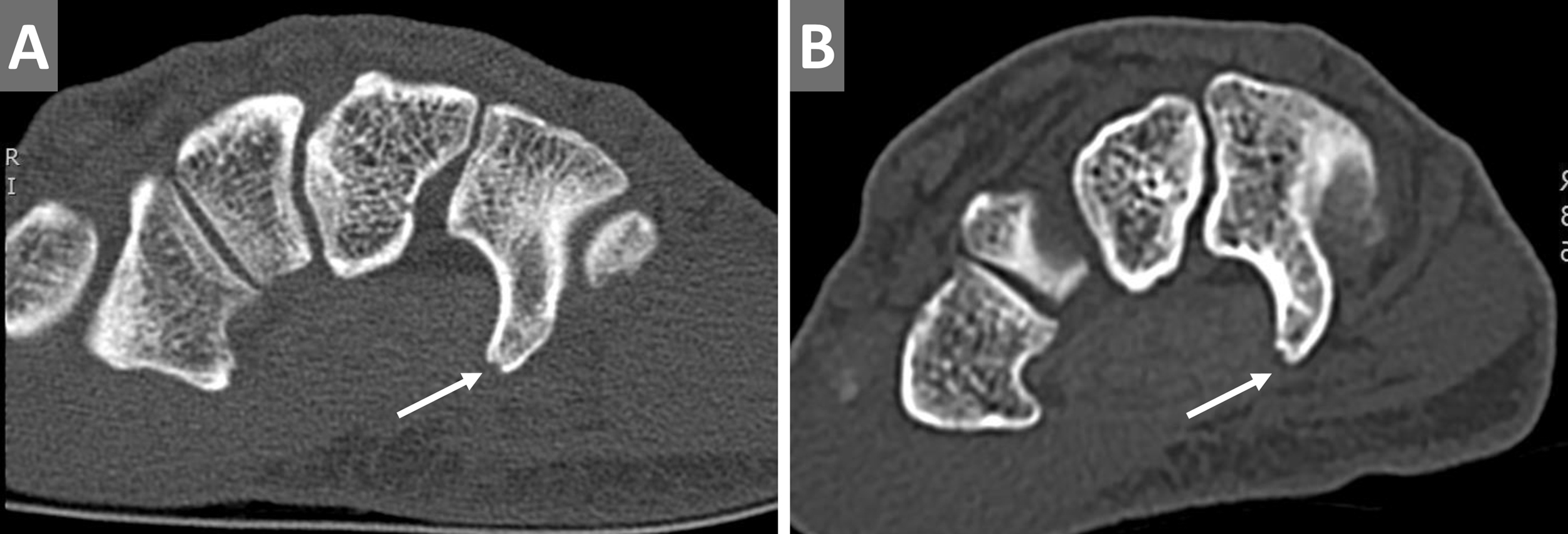
Typical type I(III) fracture of the hamate hook in a rock climbing athlete: fracture site at the base of the hook (arrow).
Type I(I) fractures of the hamate with avulsion fractures at the tip of the hook (arrows).
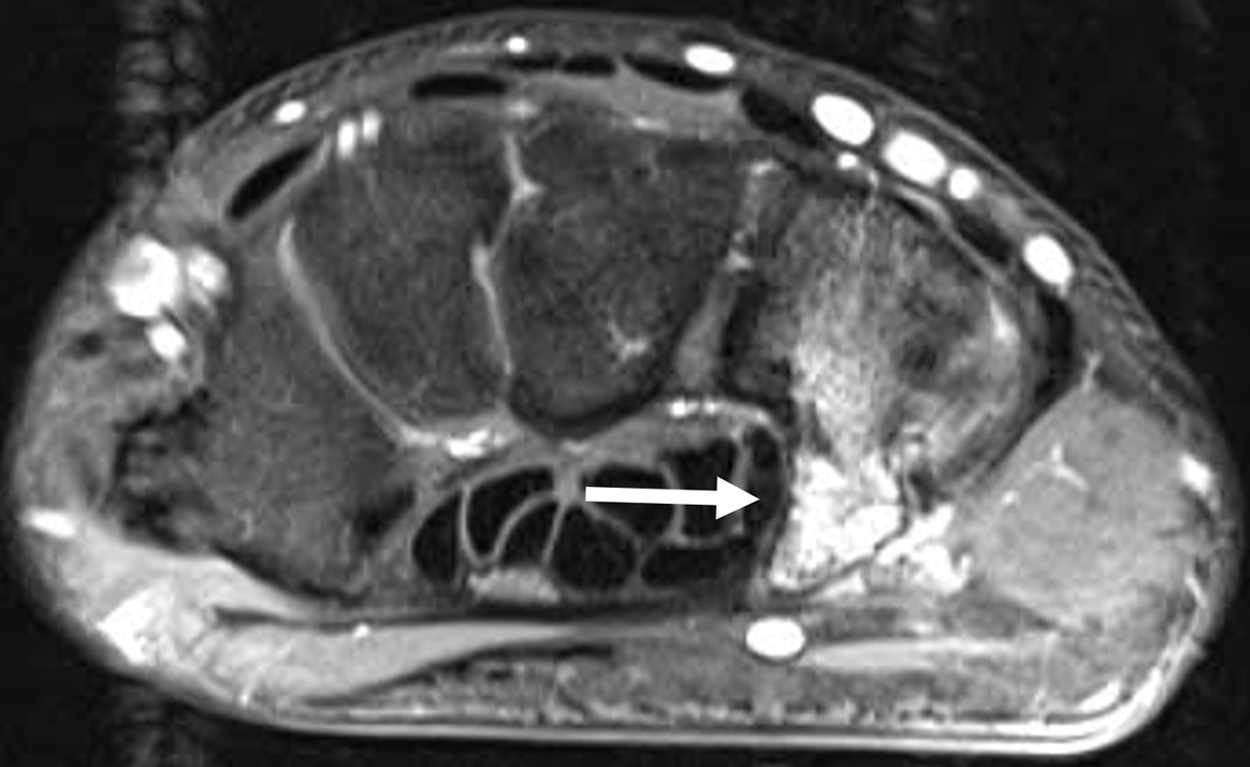
Magnetic resonance image of a type I(II) hamate hook fracture with bone bruise in a 31-year-old rock climbing athlete.
The average duration of symptoms was 12.3 ± 14.9 (0–56) weeks before the athlete was seen by a medical specialist for the first time. First follow-up investigations for all patients were performed no later than 8 weeks after initial contact. Conservative treatment resulted in reduced pain and restored strength in 9 of the 12 patients. Follow-up radiograph or CT showed consolidated situations within the hamate bones, and the process of healing was satisfactory. One athlete was additionally treated with a circular wrist tape after he restarted training. Recovery under conservative therapy was 8.2 ± 1.5 (6–12) weeks in duration, and the final outcome (full recovery of preinjury climbing level) was satisfying in all athletes. Furthermore, 1 athlete was treated with steroid injection into the carpal tunnel; he was free of symptoms within 12 weeks.
A surgical procedure was required for 3 patients. One of these patients initially experienced a type I fracture of the hamate combined with a ganglion of the second annular pulley, which was immediately treated surgically. In the other 2 patients, we performed a resection of the hamate hook, as nonunion was seen in follow-up investigations after immobilization (type I fractures). A fourth patient whose initial therapy had failed received a double shot steroid injection close to the hamate hook and became free of symptoms. Nonsteroidal anti-inflammatory drug (NSAID) therapy—which preceded the correct diagnosis, in some cases over a period of weeks—showed no benefit.
All patients who underwent surgery were free of symptoms after 14.0 ± 2.8 (12–18) weeks. The overall duration of symptoms was 10.7 ± 5.1 (6–24) weeks in our patient collective (Table 2). During late follow-up investigations approximately 6 months after last contact, all athletes confirmed that they were free of symptoms (no pain; numerical analogue pain scale) and all had regained full strength and their preinjury climbing level (UIAA metric scale). 10
One young patient, a member of the German National Team who reported a repetitive injury and pain in the hamate, had not initially contacted a specialist. After the pain had subsided after 6 weeks, he continued climbing. During preparation for the European championships, he finally reported pain in the wrist and was medically evaluated. The MRI and CT scans showed a refractured nonunion of a hamate fracture (Figure 4). Due to his young age, we decided to attempt conservative therapy, consisting of 6 weeks of casting and 2 weeks of orthotics. A control CT scan after 6 weeks of immobilization found a partial healing of the bone; another 6 weeks later, a second scan finally showed a union of the fracture, and the athlete was allowed to restart and slowly increase sport-specific stress after 12 weeks (Figure 4). No further symptoms resulted.
Discussion
Fractures of the hamate are well known to occur during different sports, such as golf, baseball, or mountain biking. 2 ,3,7,11–13 However, all of these sports provide a direct external impact on the hamate, which is transmitted by a bat or by handle bars. High-impact impulses acting directly on the hamate hook can lead to a fracture of this bone.3,6 During climbing, there usually are no high pressure situations directly affecting the hamate hook externally, as this sport is characterized by moving upward or sideways against the influence of gravity. Body weight is supported by tensile loading largely within the arms, hands, and fingers. Stress is applied to the hook of the hamate by tightened flexor tendons, which press against the ulnar margin of the carpal tunnel. 14 This situation mainly arises when the hand is repeatedly loaded with the wrist in ulnar deviation (“side-undercling position” of the hand, Figure 2). 1 Fractures of the hamate hook that are most likely caused by internal contact pressure of tendons and not by external trauma are rare. In our opinion, this occurs nearly exclusively during climbing or bouldering. 1
We first described fractures of the hamate in rock climbing athletes in 2009. 1 It is known that this symptom often accompanies bone marrow edema. Therefore, we previously conducted a study in which we first described bone marrow edema in the hand/wrist in rock-climbing athletes. 15
The increase in the frequency of hamate fractures is probably due to the rising number of athletes who are able to climb at higher levels of difficulty. Climbing experience and climbing level were higher in our patient group compared with rock-climbing athletes who experience other types of hand or finger injuries.15,16 Ten or 20 years ago, only a few professional athletes were able to successfully climb routes at the upper end of the UIAA metric scale. 10 Because of an increased number of climbers combined with modern training concepts and better climbing gyms, more athletes reach the upper end of the climbing scales.15,16 Even though hamate fractures will only affect a small subset of climbers, the injury and pathomechanism we describe might become more important with the rising number of high-level athletes.
Whether excessive tensile load can cause stress fractures has not yet been properly investigated. However, it is comprehensible that repetition of the same strenuous movement (common during training for a hard climbing route or boulder problem) could lead to stress fractures within the bones that are affected most by the tightened flexor tendons. 1 Nevertheless, a list of potential differential diagnoses should be considered, as fractures can also be based on other pathologies (Table 3). The possibility of direct trauma of the hands always needs to be assessed, even if the patient does not remember having incurred a trauma. Impact traumas can occur especially in bouldering, where athletes are only protected by mats on the ground. In adult rock-climbing patients with wrist pain, a variety of other differential diagnosis should also be considered, such as arthritis or collapsed cysts resulting from degenerative alterations as described previously.15,17
Differential diagnosis of hamate fractures
In our series, no patient presented a type II fracture or any other injury of the carpal bones; therefore, we believe that the fractures resulted from the high contact pressure of the tendons rather than from direct impact or repetitive strain to the hook via the palm.3,6
Fractures of hamate bones are challenging to diagnose in radiograph. Therefore, a CT scan or MRI should be considered in rock-climbing athletes who have pressure pain over the hamate without diagnostic radiographic findings. 2 ,6,9,11,18–20 If no fracture can be seen in CT, but clinical examination clearly shows pathology of the hamate hook, it can be interpreted as “insertions-ligamentopathy” of the hamate’s hook-tip.
A delayed healing progress can occur if patients restart rock climbing or training too early and with a high load. Therefore, we recommend a break in training of at least 3 months in cases of documented hamate fractures. Consolidation of the fracture site should be ensured and documented by CT, as small finger tendons can be frayed by the fracture site, which could ultimately lead to a rupture of the tendon.3,6 Furthermore, the ulnar nerve can be irritated by loose fragments. 3 ,6,9,12,18
Of the 3 options for treating hamate hook fractures (excision of the fragments, open reduction and internal fixation, and cast immobilization), most reports indicate a preference for excision of the fragments. 3 ,6,7,19,21,22 However, biomechanical studies have found that resection of the hamate hook leads to a 15% decrease of the flexor tendon forces, especially with the wrist in 30 degree extension and 30 degree ulnar deviation.3,14 This weakening would subsequently lead to a restriction of the climber’s ability. Therefore, we recommend conservative therapy or open reduction and internal fixation to avoid fragment resection in type I fractures, especially in type I(II) or type I(III) cases in which relatively large fragments have been detected via CT. Xiong et al reported a high risk of nonunions, especially in type I(II) fractures with fracture sites in the center of the hook. 3 However, even patients with conservatively treated type I(II) fractures mostly experienced good healing. Nevertheless, physicians should be cognizant of the risk of nonunions; in such cases, a resection of the fragments and the residual base of the hook combined with a coverage of the fracture section with soft tissue is required. 3 ,20,23,24
NSAID therapy did not appear beneficial in our case series, although larger studies are required to conclude that they are of no benefit. Furthermore, NSAIDs are known to reduce osteoblastic activity and may be counterproductive. 25 However, this study was not designed and powered to assess NSAID effects in hamate, and therefore conclusions have to be assessed critically.
A treatment with circular wrist tape, which is supposed to protect the wrist by ensuring additional stability, can show varying results. This tape support leads to an increase of pressure within the wrist, which can trigger previous symptoms. Therefore, we recommend testing circular wrist taping, which can be continued if determined to be helpful.
High training frequency with high exercise load (especially repetition of the same difficult move) is probably the reason for the described condition. Younger climbers who have developed a fracture of the hamate may exceed their tolerance limit and practice with a peak load that is too high and relaxation breaks that are too short. Constant repetition of strenuous moves, especially with the hand in a position of maximal ulnar deviation, is the main risk factor for this type of injury. Therefore, medical supervision is mandatory, and physicians treating rock climbing athletes should be aware of this pathomechanism and the injury itself.
Study Limitations
The present study is a case series that is not large enough to investigate any statistically significant differences between treatment type or outcome. Therefore, all findings should be interpreted with caution. Whether tightened flexor tendons can create a pressure that is high enough to cause fractures of the hook has not yet been finally proved; further studies including more cases of hook fractures in rock climbing athletes are needed to provide a better understanding of development and special features of this affection. Therefore, it is essential to interpret the results in context.
Conclusion
Hamate fractures should be considered in rock-climbing athletes who experience pain in the wrist after performing strenuous moves, especially repetitively. Anatomical circumstances and shape of the carpal bone are reasons for the frequent occurrence of fractures within the bone; tightened flexor tendons may create high contact pressure on the hamate hook during strain of the flexor muscles of the fingers, leading to stress fractures. Clinical investigation, radiographs, and CT determine the proper diagnosis; the therapeutic approach in rock-climbing athletes should be immobilization. If a nonunion occurs, surgical resection of the fragments combined with a resection of the residual base is necessary. If healing is seen under conservative therapy, the training routine has to be adjusted to avoid refractures or other injuries. In cases of stress-induced return of symptoms, an additional protective circular wrist tape can be useful if the patient feels comfortable with it.
Acknowledgments: The authors thank Rosamunde Pare for English language support.
Author Contributions: Study concept and design (CL, AS, TH, VS, TB); acquisition of the data (CL, AS, TH, VS); analysis of the data (CL, AS, TH, VS, TB); drafting of the manuscript (CL, AS, TH, VS); critical revision of the manuscript (AS, TH, TB); and approval of final manuscript (CL, AS, TH, TB, VS).
Disclosures: None.
Footnotes
Submitted for publication April 2016.
Accepted for publication September 2016.