
Abstract
Burns are a common source of injuries worldwide, with a high burden of disease in low- and middle-income countries. Burns also account for 2%−8% of wilderness injuries. Although many are minor, the potential for serious morbidity and mortality exists, and standard treatments used in high-resource settings are not readily available in the backcountry. A literature review was performed to find evidence from low-resource settings that supports alternative or improvised therapies that may be adapted to care of burns in the wilderness. There is good evidence for use of oral rehydration to support volume status in burn patients. There is moderate evidence to support cold therapy as first aid and adjunct for pain control. Some evidence supports use of alternative dressings such as boiled potato peel, banana leaf, aloe vera, honey, sugar paste, and papaya when standard therapies are not available.
Introduction
Multiple large studies of wilderness trauma show burns account for 2%−8% of injuries. 1 –6 Recreational areas with geothermal features have higher rates of severe injuries. 7 The primary mechanisms of burn in the wilderness setting are scalds from hot liquids and thermal burns from direct contact with hot objects such as stoves, lanterns, and coals from campfires. Injuries from direct contact with flames are less common. Campfire burns are recognized as a worldwide problem, as evidenced by case series from San Diego,8,9 Arizona, 10 Australia, 11 Saudi Arabia, 12 and South Africa. 13 These injuries frequently involve the hands and feet, with a high potential for long-term morbidity.
Burn injuries are also a leading cause of trauma globally, with 85% of injuries occurring in low- and middle-income countries, where therapeutic options are limited by resource constraints. 14 Up to 17.5 million burns occur in children in sub-Saharan Africa annually. 15 India has an estimated 600,000–700,000 admissions to burn units per year. 16 Morbidity and mortality are higher for a given injury in low- and middle-income countries. 15 Currently, the burn size associated with a 50% case fatality in high-income countries is between 60% and 70% total body surface area (TBSA). 17 In Nepal, burns between 20%−30% TBSA carried a 50% mortality rate, and no patient survived burns of more than 40% TBSA. 18 We hypothesize that treatments used in low-resource settings can be adapted to backcountry care of burn injuries.
Most burns occur in males during the working years of life. Although scalds are the most common burns in children less than 5 years of age, burns due to exposure to fire or flame predominate in all other age groups. The majority of burns are relatively small with only 2% covering 40% TBSA or more. 19
Case report
Three days into a 14-day backpacking trip in the rural mountainous region of Nepal, an otherwise healthy 26-year-old man sustained scald burns from a pot of boiling water. He had partial thickness burns to the dorsal aspect of the left forearm and anterior thighs totaling 15% TBSA. First aid consisted of rinsing the areas with cool water from a nearby stream. He was seen at the health post of a nearby village, where large blisters were sharply debrided and the wounds were dressed with honey and boiled potato peel dressings. Pain control was adequate with cold therapy and nonsteroidal anti-inflammatory medications. He completed the trip and was seen for wound check when he returned to Kathmandu. A hydrocolloid dressing was used on the remaining open area on the left thigh. His burns healed with acceptable cosmetic outcome.
First aid
Cold therapy such as use of cool running water or cold compresses has been shown to limit the depth and size of burns 20 and is an important adjunct for pain control. In 1 study in Nigeria, patients treated with cool water lavage had a lower complication rate than those treated with other forms of first aid. 21 Optimal temperature and duration of cold therapy have not been extensively studied, 22 but use of ice water and direct application of ice has been shown to worsen burn healing.23,24 Loss of skin integrity from burns impairs the body’s ability to thermoregulate, but prehospital use of cold therapy was not associated with hypothermia in one study. 25 The authors suggested that clinically important hypothermia would only be a concern for extensive burns, 70% TBSA or greater.
The burn wound should be gently cleansed to remove debris. There is a paucity of evidence to guide management of blisters, and clinical controversy persists. Citing concerns about inflammatory mediators in blister fluid and infection risk with the presence of devitalized tissue in the wound, some authors recommend debridement of nonintact blisters, blisters over joints, and blisters larger than 6 mm. 26 Leaving the blisters intact is advocated by 1 review, which found enhanced patient comfort and lower risk of infection with conservative management than with aspiration or debridement. 27
After cleansing and possibly debridement of blisters, the wound should be evaluated to determine the location, size, and depth. Burn size is estimated using the “rule of nines” or a pediatric modification. For smaller areas, the palmar surface of the patient’s hand represents 1% TBSA. Unlike most traumatic injuries, burns are dynamic and tend to progress over time; thus, it may be difficult to accurately assess burn depth immediately after injury. 28 The initial estimate will guide fluid therapy and suggest need for evacuation. Serial assessments may be required to determine the most appropriate therapeutic plan.
Fluid therapy
Given insensible losses and leakage of intravascular fluid into the soft tissues, maintaining adequate circulating volume is crucial. Patients with deep burns covering larger body surface areas will require fluid resuscitation to support vital organ perfusion and ensure adequate urine output. When intravenous access is available, the Parkland formula is the most common method used to calculate fluid requirements. 29 –31 It calls for 4 mL/kg/%TBSA of Ringer’s lactate solution over the first 24 hours; half of the fluid is given within the first 8 hours after injury and the other half is given over the next 16 hours.
Concern that excess fluid administration contributes to burn edema and lung injury have led to multiple modifications of resuscitation protocols. 32 The Modified Brooke formula calls for 2 mg/kg/%TBSA in adults and 3 mg/kg/%TBSA in children in the first 24 hours. The United States Armed Forces Institute of Surgical Research has recently proposed a simplified formula, the “rule of 10” in which patients are administered 10 mL Ringer’s lactate solution for every %TBSA per hour, with hourly adjustments based on clinical response and urine output. 33 The rule of 10 has acceptable predictive value for adult patients but has not been validated for pediatric patients. 34 The target urine output is 0.5 mg/kg/h for adults and 1 mg/kg/h for pediatric patients.
In low-resource settings, oral rehydration therapy is routinely used for burns of less than 20% TBSA and has been successful in treating burns up to 40% TBSA. 35 –37 Frequent small sips of fluid are better tolerated than larger boluses. Oral rehydration therapy salts can be purchased or improvised according to several recipes (Table 1), or locally available substitutes such as salted rice water or lassi may be used. 38 If patients are unable to tolerate large volumes of fluid orally, rectal infusion therapy (proctoclysis) can be implemented with oral rehydration therapy solution. A urethral catheter is inserted into the rectum, and fluids are instilled according to the patient’s clinical condition and tolerance of the infusion. 39
Formulas to prepare oral rehydration solution
KCl, potassium chloride.
Pain management
Adequate pain control is thought to reduce long-term psychological sequelae after burns. 40 For decades, cold therapy has been advocated to control burn pain,41,42 but recent data to support its use is limited. 43 Narcotic analgesics, often in high doses, are the mainstay of pain control in the hospital setting. 44 Acetaminophen and nonsteroidal anti-inflammatories reduce the total amount of opioids required, and anticonvulsants and antidepressants are used to treat the neuropathic component of burn pain. 45 Clonidine has been utilized for pediatric burn pain; it is thought to reduce pain in burns by stimulating the descending inhibitory pain pathways in the spinal cord as well as by acting as a mild sedative. 46 Ketamine has been used extensively for pain control in burn units in the developed world and in austere and low-resource settings. 47 –51 Adjuncts such as reassurance, hypnosis, music therapy, and distraction may also be of benefit. 52
Topical agents and burn dressings
Burn wounds are sterile for the first 24–48 hours, after which the wound becomes colonized with skin flora. By days 5–7 postinjury, gram-negative organisms predominate. 53 The purpose of burn dressings is to minimize bacterial counts to reduce the chance of overt infection and to provide a moist environment for optimal healing. If field management of a burn will be attempted, topical agents and a dressing should be applied to the wound. The standard of care in high-resource environments is evolving; advanced dressings such as hydrocolloids, silver impregnated gauze, and biosynthetic skin substitutes have largely replaced traditional topical antimicrobials. 54 –57 However, such dressings may not be available in the wilderness setting.
Silver sulfadiazine (SSD) was historically the topical agent of choice and is still used in many low-resource settings.58,59 Most alternative dressings that have undergone clinical trials were compared with SSD. However, Genuino et al found that burns treated with petrolatum-impregnated gauze without an antibacterial agent healed slightly faster than SSD-treated wounds. 60
A 2007 meta-analysis suggested that topical aloe vera was at least as effective as standard therapies, but the evidence was rated as poor quality. 61 If aloe vera is being harvested in the field, users should be careful to choose the correct plant, as plants that are similar in appearance can be caustic (Figure 1).

Aloe vera plant.
Honey is an ancient traditional remedy for wounds and is supported by modern scientific evidence. The antimicrobial properties of honey have been attributed to osmotic gradient, acidity, and inhibines. 62 Honey has been shown to inhibit Pseudomonas, an important cause of burn infections. 63 Honey has been shown to be at least as effective as SSD in several studies.64,65 A recent meta-analysis 66 and a Cochrane review 67 support use of honey for partial thickness burns. Sugar paste is reported to have similar effects due to the hyperosmolarity but is not well studied in burns (Table 2). 68
Preparation of sugar paste
Banana leaf dressings (BLD) have the advantage of being inexpensive and widely available in the tropics and are nonadherent due to their waxy surface. Use of BLD dates back decades. 69 Dressing changes with BLD are reported to be less painful than traditional dressings, and wounds treated with BLD healed faster. 70 Banana leaves must be sterilized before use, as they can be contaminated with pathogens such as Clostridium, Bacillus, and mold. Autoclaving is believed to be the optimal technique, but boiling and chemical sterilization have also been shown to decrease bacterial load (Figure 2). 71

Close-up of banana leaf, showing waxy texture.
Boiled potato peel dressings (BPPD), alone or in combination with SSD, were first described more than 30 years ago. 72 They are reported to reduce wound desiccation and hasten epithelial regeneration. 73 BPPD are laborious to prepare 74 and 1 study found them inferior to honey, 75 but they may be more readily available in the backcountry setting in temperate zones than other alternative dressings. To prepare a BPPD, the potato skin is cleaned, then the potato is boiled whole. The pulp is aseptically removed, and the inner side of the potato skin is placed on the open area (Figure 3). 72
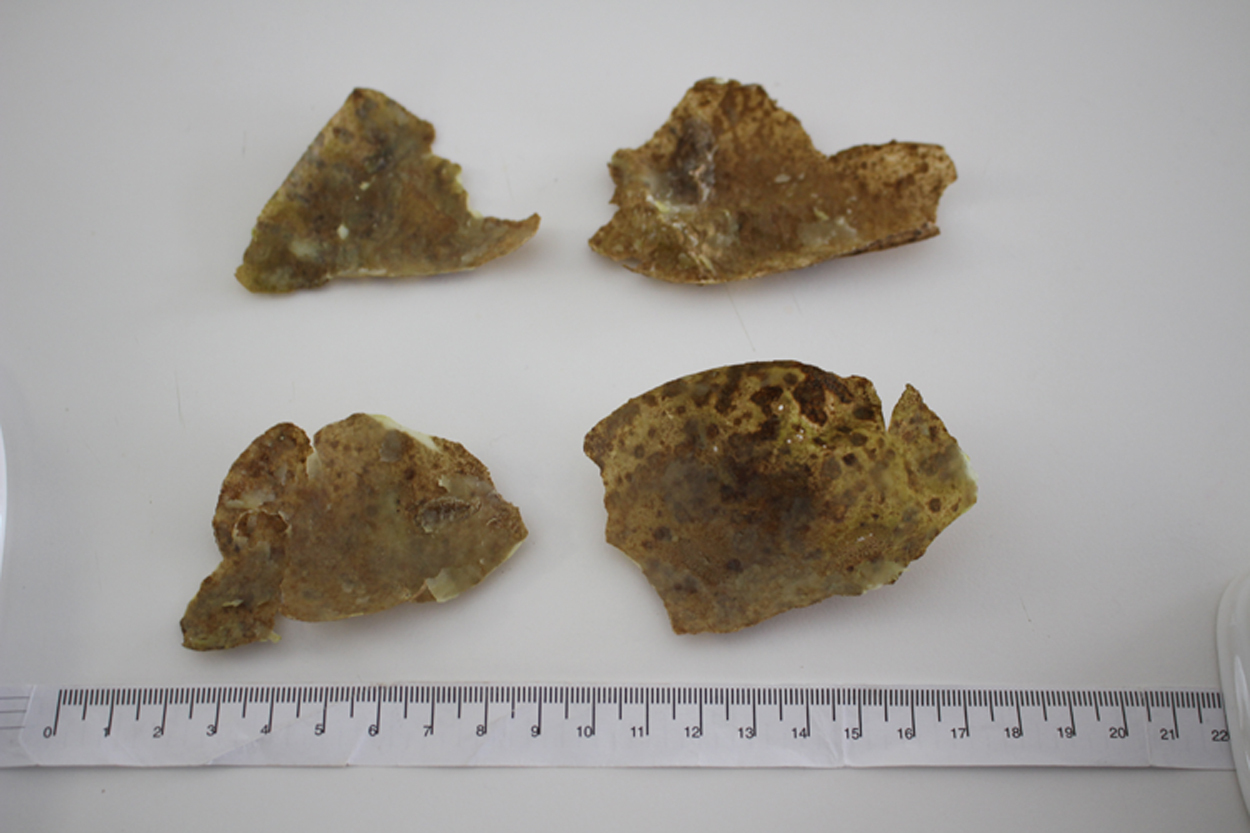
Boiled potato peel dressing, prepared as described in text.
Use of enzymatic debridement in lieu of early escharotomy and skin grafting has been advocated by some authors, 76 and a commercial product derived from pineapple is approved for use in Europe. Paste made from papaya, readily available and inexpensive in the tropics, has also been utilized for burn dressings. 77 It is thought to act as an enzymatic debriding agent and contains substances that inhibit bacterial growth (Figure 4). 78 Kiwifruit was shown to have similar properties in an animal experiment, 79 but there is no evidence from human trials.

Papaya fruit.
Other topical agents with animal data to suggest their effectiveness include turmeric, 80 yarrow, 81 coconut oil, 82 and St. John’s Wort. 83 Many other traditional agents are being investigated for efficacy. 84 –86
Placing a dressing over the wound helps keep the wound moist for optimal healing. Clean, food-quality, plastic cling wrap can be considered free of significant pathogens. 87 Amniotic membrane is often used as a wound dressing in low- and middle-income countries 88 but is not likely to be available in the backcountry. Membranes from the inside of egg shells may be useful for small areas. 89 A layer of sterile gauze or clean clothing can be wrapped over the burn to shield the area and prevent heat loss.
Evacuation
Most superficial and small burns can be managed in the wilderness setting, with clinic or emergency department follow-up within the following few days. Patients with other trauma, large or deep burns, burns involving critical areas, or those with significant comorbidities should be evacuated for evaluation in a hospital setting. Wilderness Medical Society guidelines for evacuation of burns recommend urgent evacuation for patients with inhalational injury; burns to the thorax that impair ventilation; circumferential burns to extremities; significant burns to the hands, feet, face or mucous membranes; full thickness burns greater than 5% TBSA; partial thickness burns greater than 10%−20% TBSA; or burns that become secondarily infected. 90 Most low-resource settings do not have burn centers, unless located in a major urban setting or teaching institution.
Conclusion
Burns are potentially devastating injuries that may occur in the wilderness setting. Evidence for many first aid interventions and scientific confirmation of traditional treatments is all too often lacking. Improvised dressings such as aloe vera, honey, and banana leaf are at least as effective as SSD and are reasonable options when advanced dressings are not available. Knowledge of alternative fluid resuscitation methods and wound care can give the wilderness medical provider additional options for treating these potentially devastating injuries in low resource and remote settings.
Author Contributions: Study concept and design (CB); acquisition of the data (CB); drafting of the manuscript (CB); critical revision of the manuscript (TE); and approval of the final manuscript (CB, TE).
Financial/Material Support: None.
Disclosures: None.
Footnotes
Submitted for publication May 2016.
Accepted for publication September 2016.