
Abstract
Objective
Sports ice climbing (SIC) is developing rapidly as an independent sport with Olympic potentials. To date there has been no prior systematic evaluation of injury risks and injury patterns in a SIC-specific setting.
Methods
This paper reports injury statistics collected during the Ice Climbing Festival, which was held during the XXII Winter Olympics in Sochi, Russia. More than 2500 amateur climbers and 53 professional athletes climbed during 16 days on a dry tooling lead-difficulty, and a 17-m vertical ice wall (grade M4/M5 or Union Internationale des Associations d’Alpinisme [UIAA] V+/VI–).
Results
The injury incidence rates were 0.82/100 in lead-difficulty and 0.83/100 in speed ice climbing with an overall incidence rate of 0.83/100. The injury risk in amateur climbers was 248 injuries per 1000 hours of sports activities. There were no major accidents or fatalities during the event. SIC could be graded I according to UIAA Fatality Risk Classification. Penetrating and superficial soft tissue injuries (cuts and bruises) were the most common. The anteromedial aspects of the thigh and knee were the most typical injury locations.
Conclusions
The findings from this study provide an opportunity to compare injury patterns in SIC with what has previously been reported for traditional ice climbing. SIC has lower fatality risks, higher minor injury rates, and comparable injury severity to traditional ice climbing. The main limitation of our findings is that they were obtained on a population of amateur ice climbers with no previous experience. Further research should be performed to define injury risks in professional competitive ice climbers, and standard methodologies for reporting injuries should be considered.
Introduction
Ice climbing is an extreme sport that was historically part of traditional mountaineering and consisted in ascending natural walls such as ice-covered cliffs or frozen waterfalls (traditional ice climbing). Schöffl et al 1 distinguishes 2 subdisciplines of traditional ice climbing—alpine ice and water ice climbing. Sports ice climbing (SIC), which consists of 2 disciplines—lead and speed—could be defined as ice climbing activities and competitions, which are held according to Union International Association de Alpinism (UIAA) rules in a specific setting: artificial vertical ice wall or overhanging dry tooling section. SIC has been developing rapidly since the mid-20th century. The first International World Cup (IWC) was held in 2000 in Cortinia, Italy. The IWC generally consists of 4 to 6 separate competitions held during a 3- or 4-month competition season, with each event hosting at least 100 competitors. The ice climbing competition world has recently expanded with youth competitions in 2013, and para–ice climbing events in 2014. SIC was showcased during the XXII Winter Olympics in Sochi, Russia, and is being considered for a full Olympic medal sport event.
The number of papers about the medical aspect of ice climbing remains low. All previous studies were focused on traditional ice climbing (or associated outdoor activities). An essay by Patterson 2 gives a general description of injuries in ice climbing, and Schindera et al 3 describe injuries from glacial sports including ice climbing, but that reflects only patients who were involved in glacial-crevasse or ice-field falls. There are only 2 original studies specific to medical considerations for ice climbing: Mosimann 4 and Schöffl et al 1 , and other 2 other papers by Schöffl et al5,6 summarized and reviewed these data.
Mosimann 4 describes injury patterns in traditional ice climbing and did not include any activities in a sport-specific setting. A retrospective questionnaire study on 88 climbers by Schöffl et al 1 gives a comprehensive analysis of risks and injury patterns in traditional ice climbing but is also not specific to SIC. Review papers by Schöffl et al5,6 compare the epidemiology of injuries in mountaineering and rock and ice climbing; however, they summarize data from previous studies that were conducted in traditional ice climbing. Taken together, these studies showed small injury rates, minor injury severity, and few fatalities. 5
To our knowledge there has been no prior systematic evaluation of injury risks and injury patterns in an SIC-specific setting. Another limitation of previous studies is that data were often not reported in a standardized manner.
SOCHI 2014 ICE CLIMBING FESTIVAL OVERVIEW
The Ice Climbing Festival was held in the Olympic Park during the XXII Winter Olympics in Sochi, Russia, as a part of the cultural program in 2014. More than 2000 people came to visit the ice climbing venue (Figures 1 and 2) of the festival every day to explore the different aspects of mountaineering such as rope work, dry tooling, and climbing actual ice on a manmade structure.

Venue of the event. Speed ice climbing wall at night.

Venue of the event. Lead climbing wall.
The ice climbing construction had 2 independent structures: an overhanging dry tooling lead-difficulty and a 3-sided 17-m vertical ice wall (grade M4/M5 or UIAA V+/VI–), used for speed climbing in competition but also used for amateurs. Most of the amateurs climbed on the latter, and the dry tooling section was only used as an alternative if the ice wall was closed as a result of weather conditions. Top rope belay in both disciplines was used. Amateurs who ice climbed during the festival had little, if any, previous experience in traditional ice climbing or SIC. All amateur ice climbers were given safety instructions and signed a consent form with a description of possible hazards. If a person climbed several times a day, he or she signed a new consent form each time. Visitors with obvious signs of alcohol or other types of intoxication were not allowed to climb. Amateurs were provided with helmets, boots with crampons, and technical ice axes (The Light Machine; Grivel, Aosta, Italy; or ProMasteR; Ice Rock, Kirov, Russia), but not the speed climbing tools (also known as ice fifis), which are sharper and shorter than standard ice climbing tools. Climbing instructors gave visitors a short instruction about the general aspects of ice climbing techniques.
A total of 53 world professional competition ice climbers from 16 countries who take part in IWC competitions on a regular basis came to participate in the event, representing Switzerland, the United States, Canada, France, Sweden, Mongolia, Azerbaijan, Germany, Japan, the Netherlands, Great Britain, Portugal, Iran, Ukraine, South Korea, and Russia. These professional competitors showed and shared their skills with the general public and introduced ice climbing to Olympic spectators.
Methods
The Ice Climbing Festival had independent medical coverage of 2 medical doctors working alternate 24-hour shifts. Because the event was a part of a cultural program during the Olympics, medical help for both amateur and professional climbers was provided by UIAA-hired physicians on scene in a designated medical zone. In 2 cases, a hand and a face injury that needed suturing, the patients were referred to the Olympic Park medical center for definitive care. Information about all accidents, including name, age, sex of the patient, time of accident, description of injury, treatment provided, and sports discipline where the injury occurred, was recorded in a special journal. The number of amateur climbers per day was calculated based on the number of signed consent forms. Professional athletes were climbing on the lead-difficulty wall 3 to 8 runs/day and on the ice wall 2 to 10 runs/day.
Incidence rates in both disciplines were estimated as the total number of injuries divided by the total number of climbers. However, professional athletes were excluded from the calculation of incidence rates because the exact numbers of their runs per day on the ice climbing wall and the number of climbs on the lead-difficulty route were not recorded.
Climbing time on the vertical ice wall for amateur climbers was limited to 2 minutes. They finished their attempt if they reached the top, reached 2 minutes of climbing time, or injured themselves. The total climbing time for amateur climbers was calculated as the number of climbers (speed only) times 2 minutes. The injury risk per 1000 hours in speed climbing for amateurs was calculated as the total number of injuries divided by the total climbing time times 1000. The climbing time for amateur climbers on the lead-difficulty wall was not recorded.
Minor injuries, which required basic treatment (antiseptic, bandage oral analgesics, etc), were considered as grade 1, and injuries that needed stitching were considered as grade 2 (ICC UIAA MedCom score). The location of the injuries and fatality risks were classified according to the UIAA recommendation. 7
Results
Total number of amateur climbers was 2542 (2176 speed, 366 lead), with an average of 159 climbers per day (Table 1). Total climbing time for amateur climbers was 72.5 hours. Total number of injuries during the festival was 26 (21 in amateurs, 5 in professionals). For amateur climbers, 18 injuries were sustained on the ice climbing wall, and 3 injuries were sustained in the lead-difficulty wall (Table 2). Injury patterns are described in Table 3, and severity of injuries is presented in Table 4. There were no major accidents or fatalities during the event. The incidence rates were: 0.82/100 in lead-difficulty and 0.83/100 in speed ice climbing, with an overall incidence rate of 0.83/100. The injury risk in amateur climbers was 248 injuries per 1000 hours of sports activities. The risk for grade 1 injuries was 235 per 1000 hours, and the risk for grade 2 injuries was 14 per 1000 hours (Table 2).
Daily number of amateur climbers and injury exposure
Number of injuries, incidence rates, and injury risk per 1000 hours in different disciplines (amateurs only)
N/A, not applicable.
Injury patterns
OSICS, Orchard Sports Injury Classification System.
Severity of injuries
IIC, Injury and Illness Classification; UIAA, Union Internationale des Associations d’Alpinisme.
Discussion
The collected data show that penetrating and superficial soft tissue injuries—cuts (Figure 3) and bruises (Figure 4)—were the most common. Our data correlate with previous studies that also indicated open wounds and hematomas are the most acute injuries in ice climbing. 1 Most injuries were grade 1, which correlates with the results of previous findings. 1 Taking into consideration the previous experience in medical management of the UIAA IWC (seasons 2012/2013, 2013/2014), we believe there is a potential risk of fractures, sprains, head and eye injury, and deeper penetrating soft tissue injuries; however, this probability is relatively very low. Those rendering medical care at ice climbing events should consider medical preparedness for penetrating and blunt trauma. Care should be taken to ensure that bystanders and staff are clear of falling objects, and a fall zone that is secure should be kept clear during competition, as well as during setup and demolition of the venue.

Penetrating forearm injury.

Superficial soft tissue face injuries.
The total number of injuries in speed climbing was greater than that in lead-difficulty climbing; however, the incidence rates were comparable at 0.82 and 0.83 injuries per 100 climbers, respectively.
The data also reveal a high injury risk per time of sports activity that was 248/1,000 hours. This result is different from that of Schöffl et al 1 who argue that risk is 4/1000 h. A possible explanation for this discrepancy could be that we measured the pure ice climbing time, whereas total time in ice climbing activities previously assessed included other activities, such as walking, belaying, and rest. The injury risk per 1000 hours in professional athletes may be higher, as the competition climbing time is very short: 8 to 10 seconds in men and 13 to 16 seconds in women for a 15-m wall.
The number of injuries incurred by amateurs during the event was higher than that of the athletes (Table 1). All facial injuries were found in amateurs. This is likely caused by a lack of ice climbing skills, as this injury pattern is rare in sports ice climbing during competitions, based on our experience.
As can be seen from data presented in Table 1 and Figure 5, there was no clear pattern of injury risk depending on the number of amateurs. We can assume that the greater numbers of amateurs are associated with greater risk of injury. Further investigations are required to clearly show this statistical relationship.
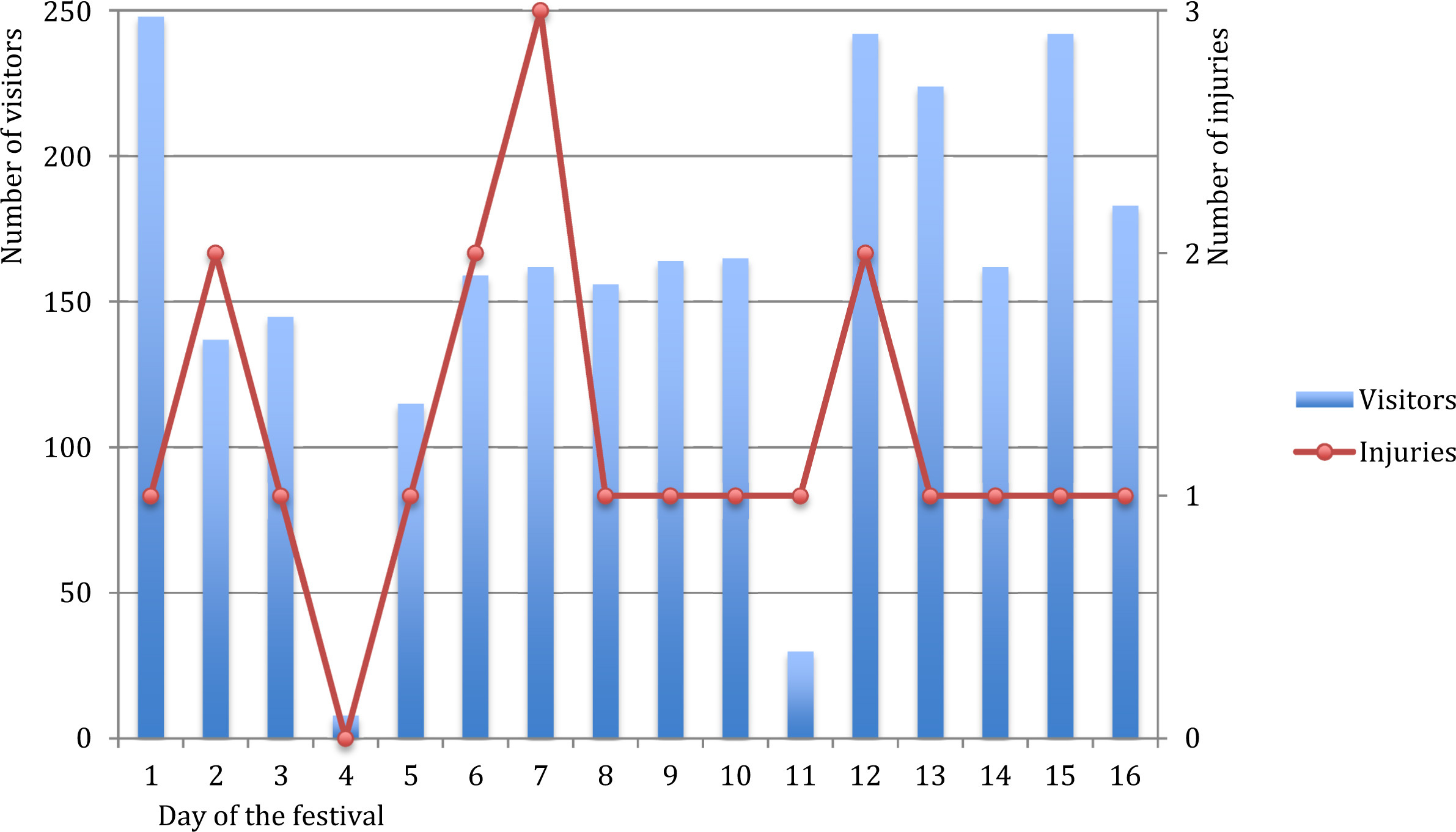
Injury exposure. Number of visitors shown as blue bars; number of injuries shown as red connected lines.
The injuries sustained were not differentiated by discipline (ie, lead-difficulty vs speed [vertical ice]). The most typical injury areas are shown in Figures 6 through 8. The anteromedial aspects of the thigh and knee were the most typical injury locations (Figure 9). Previous studies have shown that the head and upper extremity are the most injured regions during ice climbing, 1 but again, these data are relevant to traditional ice climbing and not sport specific to SIC. There are some explanations for these differences: on the one hand, physical hazards, such as avalanches, rockfalls, and icefalls, which are present in traditional ice climbing, 5 are not relevant to SIC. The specific injury pattern is more likely explained by the biomechanics of SIC, in which ice axes are aligned with the climber’s body in a loaded vector toward the body (Figures 10 and 11). There were no fatalities during the Sochi event; also we are unaware of any fatal accidents during UIAA IWCs for all years. Taken together, these results suggest that SIC could be graded I according to the UIAA Fatality Risk Classification. Personal protective clothing with the ability to resist puncture or dampen force by sharp ice axes should be considered by athletes. Key locations for protective clothing, based on our findings, are the anteromedial aspect of the thigh and knee as well as the hands. Athletes often refuse to use puncture-resistant clothing or protection as there is a perception that it affects sport performance by restricting movements and increasing the weight of the athletes.
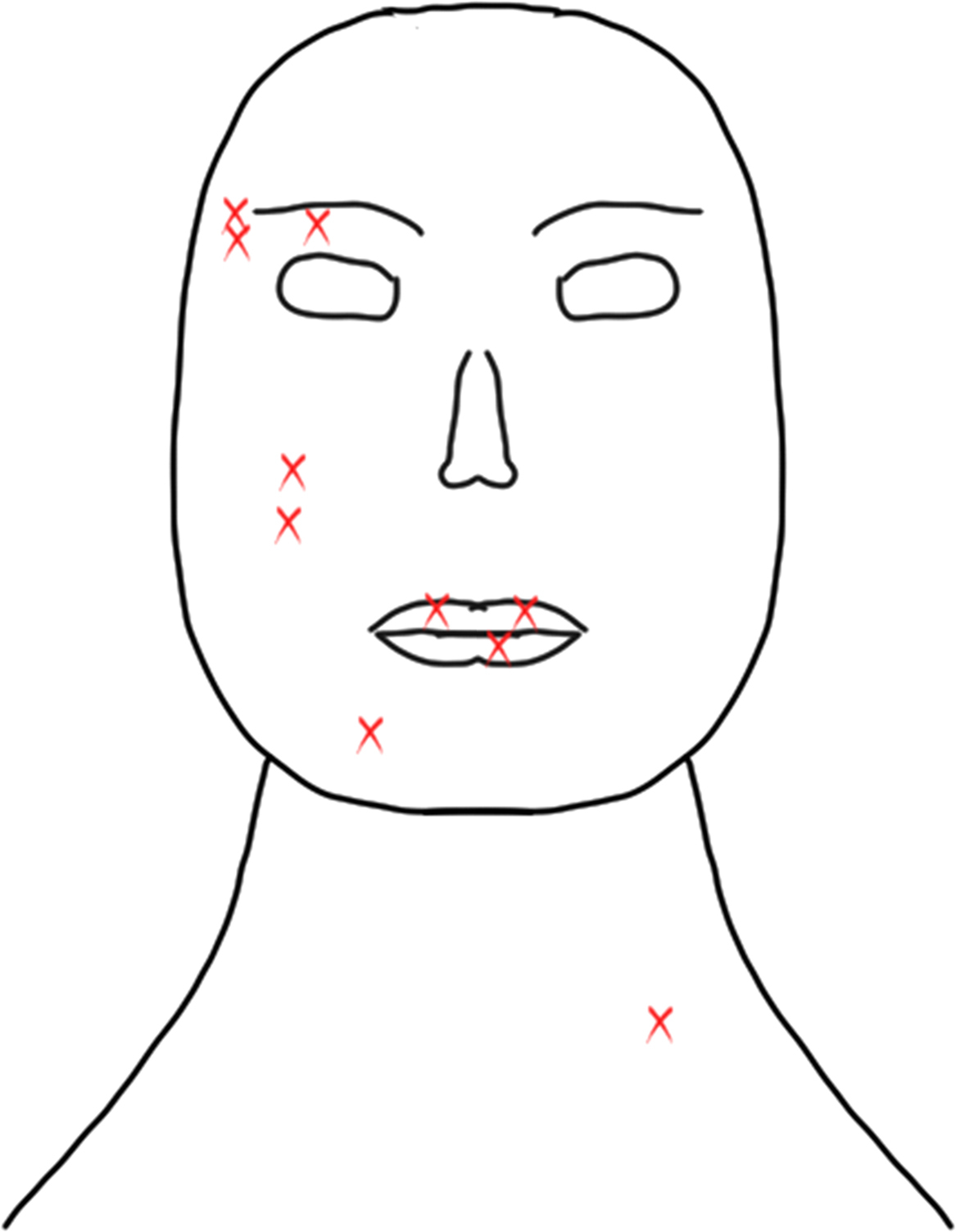
Most typical injury areas (face).

Most typical injury areas (arm).

Most typical injury areas (leg).

Typical ice climbing injury (anteromedial aspect of the thigh).

Mechanism of injury. Red arrow—leg injury, blue arrow—face injury.
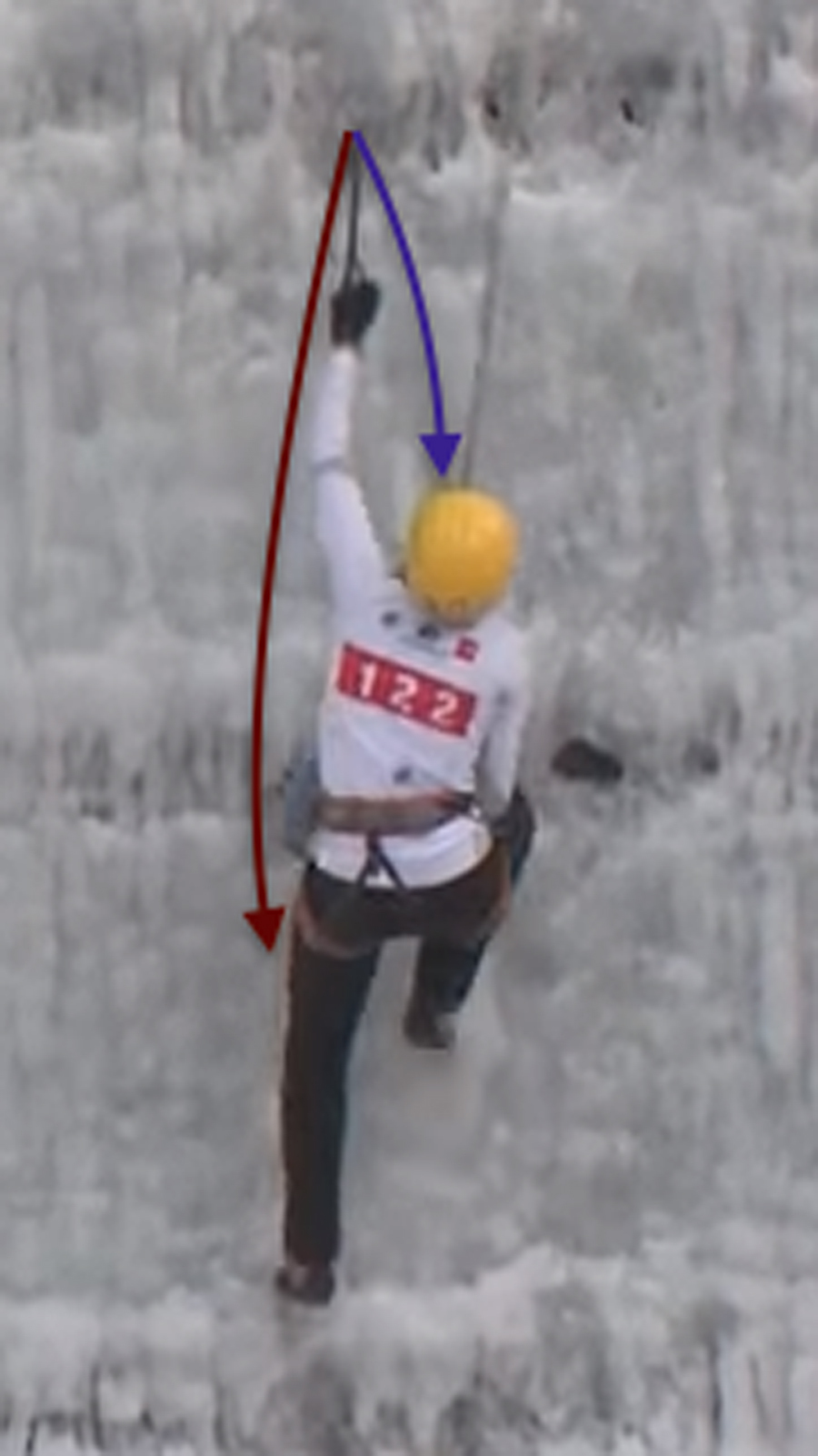
Mechanism of injury. Red arrow—leg injury, blue arrow—face injury.
Medical providers working at ice climbing events should use a standard medical kit as for other sports. SIC is generally a safe sport as it is performed in a relatively controlled environment. Our study demonstrates that the medical needs in SIC events are mostly for minor issues. However, professional medical care during ice climbing events must be provided as injuries do occur, and the possibility of major trauma exists.
With this paper we give the first analysis of injury rates in SIC, based on data collected during the Winter Olympic Games in Sochi, Russia, where more than 2500 visitors and athletes climbed during 16 days at the ice climbing venue. The findings from this study provide an opportunity to compare injury patterns in SIC with what has previously been reported for traditional ice climbing. We can conclude that SIC has lower fatality risks and higher minor injury rates than traditional ice climbing, but comparable injury severity. The main limitation of our findings is that data were obtained on a population of amateur ice climbers with no previous experience. Also, this compilation does not reflect other regular events of the UIAA IWC. It should be said that this study is a preliminary report and does not take into consideration other venues’ injuries, nor can we project injury rates or patterns outside of the sample collected. Further research should be performed to define injury risks in professional competitive ice climbers and standard methodologies for reporting injuries should be considered.
Footnotes
Acknowledgments
The authors thank Nadezhda Launits, Pavel Shabalin, and all athletes and staff who made the Sochi 2014 Ice Climbing Festival possible.