
Abstract
Multiple casualty incidents (MCIs) are uncommon in remote wilderness settings. This is a case report of a lightning strike on a Boy Scout troop hiking through Sequoia and Kings Canyon National Parks (SEKI), in which the lightning storm hindered rescue efforts. The purpose of this study was to review the response to a lightning-caused MCI in a wilderness setting, address lightning injury as it relates to field management, and discuss evacuation options in inclement weather incidents occurring in remote locations. An analysis of SEKI search and rescue data and a review of current literature were performed. A lightning strike at 10,600 feet elevation in the Sierra Nevada Mountains affected a party of 5 adults and 7 Boy Scouts (age range 12 to 17 years old). Resources mobilized for the rescue included 5 helicopters, 2 ambulances, 2 hospitals, and 15 field and 14 logistical support personnel. The incident was managed from strike to scene clearance in 4 hours and 20 minutes. There were 2 fatalities, 1 on scene and 1 in the hospital. Storm conditions complicated on-scene communication and evacuation efforts. Exposure to ongoing lightning and a remote wilderness location affected both victims and rescuers in a lightning MCI. Helicopters, the main vehicles of wilderness rescue in SEKI, can be limited by weather, daylight, and terrain. Redundancies in communication systems are vital for episodes of radio failure. Reverse triage should be implemented in lightning injury MCIs. Education of both wilderness travelers and rescuers regarding these issues should be pursued.
Keywords
Introduction
Recreation in our national parks is an increasingly popular way for people to spend their free time and experience the natural beauty of our nation. 1 In the heart of California, Sequoia and Kings Canyon National Parks and Inyo National Forest are home to the tallest peak in the 48 contiguous United States, Mount Whitney, at 14,505 feet (4421 m) above sea level. The peak season for a summit attempt is during the months of June through October, when hikers aim to avoid winter conditions requiring the use of ice axes and crampons. Summer thunderstorms are common during these peak months of recreation, leading to an increased risk for lightning injury. Despite a downward trend over the last 50 years, lightning injuries have remained the second most common cause of storm-related death in the United States (behind flash floods).2,3 Lightning morbidity and mortality in the United States affects nearly 400 persons annually, with approximately 40 deaths per year. 3
For those wishing to summit Mount Whitney, a lottery system for permits is in place to grant access to all routes. The most direct route to the summit is a 10.7 mile one-way hike from Whitney Portal, on the eastern side of the Sierra Nevada. Western access, which is often less crowded, is via the High Sierra Trailhead leaving from Giant Forest in Sequoia National Park (Figure 1). Western access takes a minimum of 10 days (round trip) to complete, comprising 70 miles from trailhead to summit one way.
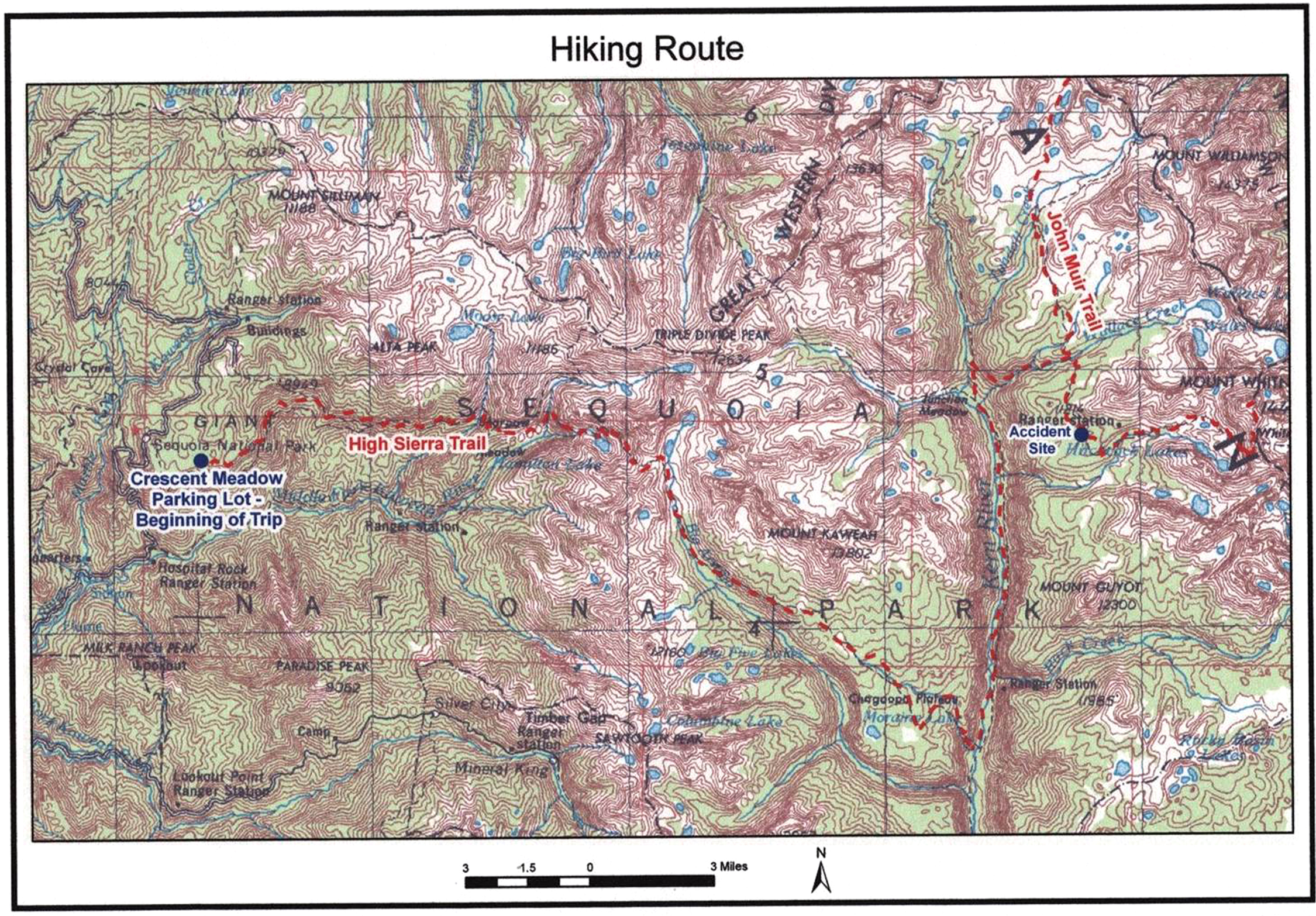
Hiking route.
We present a case of an MCI due to lightning striking a Boy Scout troop in Sequoia National Park, approximately 50 miles from the trailhead at Giant Forest to the west and more than 20 miles from Whitney Portal to the east.
This case was challenging for the prehospital providers, balancing personal safety in hazardous weather conditions against their duty to deliver rapid life-saving patient care. The objectives of this report are to review the response to a lightning-caused MCI in a wilderness setting, address field management of lightning injury, and discuss evacuation from remote locations in inclement weather.
Methods
The University of California San Francisco, Fresno (UCSF Fresno), Department of Emergency Medicine provides medical oversight for SEKI through the Parkmedic/Emergency Medical Services (EMS) program. The Parkmedic/EMS program, in operation since 1982, has provided prehospital training and protocols, and has played a lead role in the development of a unique hybrid parkmedic scope of practice utilized by EMS providers operating in our national parks. Although training is similar to that for emergency medical technician–intermediate, certified park rangers have an expanded pharmacological and procedural scope of practice allowing establishment of a definitive airway, administration of 25 to 30 different medications, and protocol-based decision-making in cases of radio failure.
A Freedom of Information Act release was obtained from the National Park Service (NPS) in 2010 to present this case to a medical audience. The details of the prehospital care were ascertained from the documentation provided, as well as firsthand accounts from the field providers involved. In addition, 3 of the authors (S.S., D.C., G.S.) were emergency physicians on duty, at the receiving facility for critical victims at the time of the incident, and have personal recollections of the event.
Case Presentation
A party of 5 adult chaperones and 7 teenage Boy Scouts were on a backpacking trip to the summit of Mount Whitney in late July 2005. In the 24 hours immediately preceding the lightning strike, they encountered deteriorating weather conditions with the accumulation of storm clouds and frequent bouts of rain. At 53 miles into their trip, and a full day’s hike from the nearest road access on the eastern side of the Sierra Nevada mountain range (Whitney Portal), the group stopped at an anticipated camping site in Sandy Meadow at approximately 1300 hours. Sandy Meadow is at 10,600 feet (3231 m) above sea level and is seen from the air as a kidney bean–shaped green clearing cradled by pines and a granite backdrop that includes the Whitney zone (Figure 2). At approximately 1430 to 1500 hours, the troop noticed an incoming storm and hastily broke into groups and erected tarpaulin (tarp) 1, tarp 2, and a tube tent at the edge of the meadow. The actual field drawing from the rescue shows the arrangement of these shelters and their occupants in relation to one another (Figure 3). Tarp 1 was strung between 2 mature foxtail pines, guyed out with parachute chord, and covered 4 chaperones and 2 scouts. Tarp 2, which covered 2 scouts, was 50 feet uphill of tarp 1 and was supported on stacked logs in a V-shape formation previously constructed by other campers. Fifty feet further uphill was a tube tent with a father and son. One scout was standing outside at the time of the incident. At 1610 hours, lightning struck one of the trees supporting tarp 1 and injured multiple victims (Table 1).

The Sandy Meadow incident site, at an elevation of 10,600 feet (3230 meters), in the Sierra Nevada mountain range.
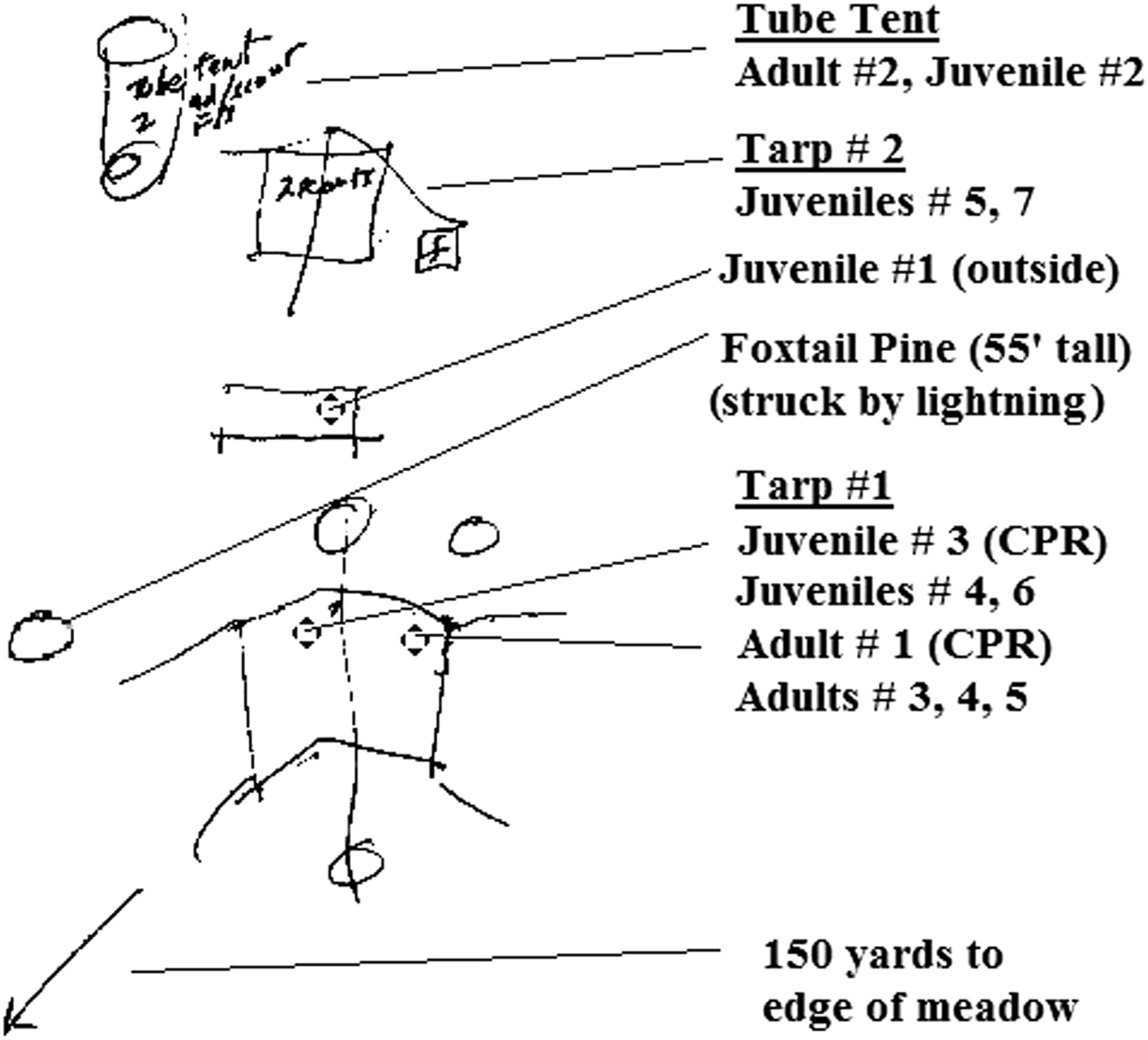
Field sketch of the structures and occupants in relation to each other from the rescue. CPR, cardiopulmonary resuscitation.
Juveniles and adults involved in the incident a
Tarp, tarpaulin; CPR, cardiopulmonary resuscitation; LZ, landing zone.
All victims were male.
Shortly after the lightning strike at 1628 hours, 2 teenage scouts arrived on foot at the Crabtree Ranger Station. Approximately 1 mile from Sandy Meadow, the backcountry ranger station was staffed by a law enforcement (LE) ranger who was certified as an emergency medical technician–basic. The initial report from these 2 scouts was that the 12-member troop had been struck by lightning and 4 people were unconscious. The LE ranger radioed dispatch requesting a helicopter and medical backup. With the 2 scouts, limited medical supplies, and oxygen, the ranger set out on foot as the first EMS responder to the scene.
The initial scene size-up at approximately 1710 hours by the LE ranger revealed a disorganized and chaotic environment. Estimating the precise number of affected persons was difficult, as additional hikers had arrived on scene, responding to the whistles and yelling from the Boy Scout troop. Two people were receiving bystander cardiopulmonary resuscitation (CPR), while others were crowded around combative or altered victims of the strike. There was a temporary reprieve from the rain and lightning, but thunderheads were still visible on the horizon while daylight faded rapidly in the overcast conditions. Radio communications were significantly affected owing to the electrically active storm. According to the field report from the EMS provider on scene: “I recall several attempts to contact incident command during this period that went unanswered, and conversely, I remember hearing broken transmissions from incident command to the incident site that were unintelligible.”
At 1743 hours, the first parkmedic, an advanced life support–level provider, arrived by helicopter H 552 and received report of patients from the LE ranger who was the first responder on scene. There were a reported 12 victims: 5 adults and 7 juveniles (Table 1). The 2 most critical patients were a 29-year-old assistant scoutmaster (adult 1) and a 13-year-old scout (juvenile 3), both receiving bystander CPR. Because of imminent storm and lightning risk, helicopter H 552 left shortly thereafter, without time to load either critical patient onboard before departure. The parkmedic took over the scene and instructed bystanders to continue CPR on adult 1 and juvenile 3, who remained unresponsive and apneic. During the continued CPR efforts, victims were assessed using simple triage and rapid transport (START triage).
In addition to the patients requiring ongoing CPR, several other victims had sustained serious injuries. Adult 4, another chaperone, was a 43-year-old man with a Glasgow Coma Score of 3 immediately after the strike who had initially received bystander CPR. On later assessment, he was intermittently combative and restrained, with eventual improvement in the field to a Glasgow Coma Score of 12 (eye response 2, motor response 6, verbal response 4). At that time, he complained of severe lumbar pain and an inability to walk. Adult 5, the 57-year-old scoutmaster, had a prolonged loss of consciousness estimated at 10 to 15 minutes and reported a period of initial whole body paralysis that had since resolved.
The rain had returned as a downpour, with cloud to ground lightning strikes intensifying. With the plan of air evacuation from the edge of Sandy Meadow, all of the ambulatory patients and unassigned bystanders were moved away from the accident site to a staging area on the edge of the meadow (Figure 4). Several scouts set up tarps to mark the helicopter landing zone in this location.
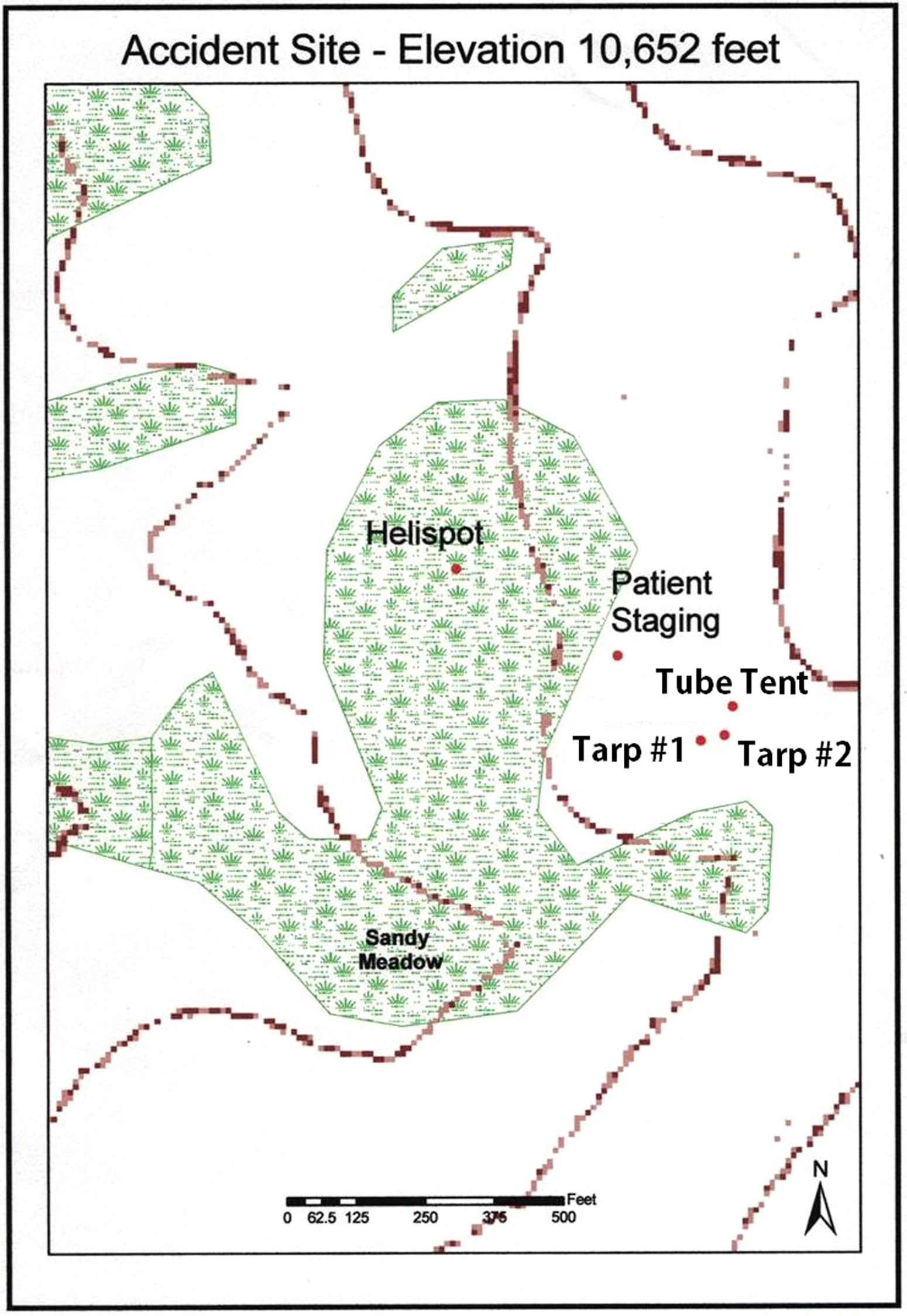
Staging areas established at the accident site.
At 1822 hours, a second helicopter, H 47 C, rerouted from working a nearby wildland fire, dropped off another parkmedic but also left the scene owing to the persistent storm risk. After a total of 90 minutes of CPR, adult 1 had no change in status, had dependent lividity, and was declared dead. Juvenile 3, also after 90 minutes of CPR, had a carotid pulse of 20 to 30 beats/min, but remained apneic. A Combitube airway was secured by the parkmedic, bystanders were instructed to perform bag-valve mask ventilation, and several intravenous line sites were established and subsequently lost owing to the inability to secure them with tape in the extremely wet conditions. The parkmedic administered 1 ampule (1 mg) epinephrine through infraglossal injection, and oxygen supplementation through bag-valve mask–assisted ventilation. The repeat pulse after epinephrine administration was 100 beats/min, blood pressure measurements were unsuccessful, and the patient was covered with a sleeping bag for warmth as nightfall approached.
At 1830 hours, thanks to a fortuitous break in the weather, helicopter evacuation became feasible. To the relief and surprise of the ground crew, who had begun to anticipate a night without radio communication or evacuation, 4 helicopters arrived in rapid succession. The helicopters involved were from different agencies: H 552, a Sequoia-Kings Canyon exclusive use helicopter (Eurocopter AS350 B2, set up for litter); H 551, a Yosemite exclusive use helicopter (Bell Super 205, litter capable); H 47 C, a rental helicopter (Bell 206 L4 Long Ranger, not set up for litter); and H 1109, a rental helicopter from Inyo National Forest (Aérospatiale SA 315B Lama, not litter capable). These 4 helicopters evacuated the scene and joined 2 ground ambulances from Tulare County, 1 ground ambulance from SEKI, Fresno’s regional H1 Skylife helicopter (Bell 407), and several government vehicles at the Ash Mountain helicopter base in SEKI to transport all patients to definitive care.
The scene was cleared of all patients, rescuers, and the deceased by 2035 hours. The bystanders who were on the scene were not evacuated and went back to their respective activities. The field triage and transport of victims from the incident is documented in Table 2. Adult 1 was declared dead on the scene after prolonged resuscitative efforts lasting approximately 90 minutes. Juvenile 3 went into cardiac arrest 2 days later in the intensive care unit at the regional trauma center secondary to complications of renal failure and multisystem organ failure. The remainder of the victims survived, with reported full recovery. Long-term follow-up and full coroner’s reports were not included with the incident-related documents released in the Freedom of Information Act reports; however, recent correspondence with the scoutmaster confirmed that all of those involved were still recovering emotionally. None of the original party has maintained backpacking or hiking hobbies since the event.
Field triage and transport of victims from incident
AM, Ash Mountain; SEKI, Sequoia and Kings Canyon National Parks; GV, government vehicle; CPR, cardiopulmonary resuscitation.
All victims were male.
In summary, a lightning strike at 10,600 feet (3231 m) in the Sierra Nevada Mountains affected a party of 5 adults and 7 Boy Scouts ranging in age from 12 to 17 years. Resources mobilized for the rescue included 5 helicopters, 2 ground ambulances, 2 receiving hospitals, 15 field personnel, and 14 logistical support personnel. The incident was managed from strike to scene clearance in 4 hours and 20 minutes. There were 2 fatalities, 1 on scene and 1 in the hospital. This case brings up pertinent areas of discussion for those involved with search and rescue operations, prehospital care, and wilderness recreation.
Discussion
The objectives of this case report were to review the response to a lightning-caused MCI in a wilderness setting, address lightning injury as it relates to field management, and discuss evacuation options in inclement weather incidents occurring in remote locations.
The Wilderness Medical Society, 3 the American Red Cross, 4 and the National Oceanic and Atmospheric Administration (NOAA) in association with the Federal Emergency Management Agency (FEMA) 5 all publish practice guidelines for the prevention and treatment of lightning injuries. Unfortunately, the guidelines are intended to be followed in advance of a storm or when caught unexpectedly in a storm and do not offer any guidance to reduce the risk of lightning strike injury to rescuers who have made the decision to respond to a call. Leaving a place of established safety (such as a ranger station) to rescue and resuscitate victims in an unsafe environment is not endorsed by EMS agencies.
This Boy Scout troop did not have substantial shelter available, and subsequently took several actions to find shelter, which likely resulted in fewer members being directly injured by the strike. They avoided the open meadow by finding a small outcropping of smaller trees 150 yards away from the meadow’s edge. Also fortuitous for them, either by design or coincidence, the scouts divided 1 large group into 3 smaller groups (tarps 1 and 2 and tube tent) to seek shelter from the rain. Although that actually increases the chance that someone might get struck by lightning, it simultaneously decreases the number of likely victims and increases the chance that someone could help if a person were struck. 5 This case demonstrates the pivotal role that uninjured victims have in rescue, as the occupants of tarp 2 and the tube tent provided immediate bystander CPR and activated the EMS system by sending 2 of their party on foot to the nearest ranger station.
It should be noted that there were additional actions that might have been taken to further minimize lightning injury risk. Tarp 1 was secured by parachute cord to anchors just feet away from a healthy, 55-foot-tall foxtail pine, whose relative height near a meadow made it a natural conduit for the strike (Figure 5). Additionally, the presence of burns on backs and buttocks also suggests several troop members were sitting or lying directly on the ground rather than using a lightning crouch, which would have been recommended for groups in a high-risk area where more effective risk reduction cannot be achieved. 6

Lightning damage is evident on a 55-foot-tall foxtail pine just adjacent to the tarp and tent shelters.
In the setting of an MCI, triage priorities are designed so that the most good can be done for the greatest number of patients. In essence, the treatment and resuscitation priorities are shifted to those who are likely to survive, and not necessarily those who are the most sick, owing to limited resources during an MCI. For example, during an MCI, a cardiac arrest would be labeled a “black” and no attempt to resuscitate the patient would be made. However, lightning is one of the exceptions to these triage rules and utilizes reverse triage principals.
The NPS EMS field manual 7 procedure for an MCI indicates use of START triage and triage tags. Using the current MCI protocol, both patients found in cardiac arrest in this case would be START triaged as “deceased/black,” prioritizing care based on acuity and the need to provide the most benefit for the greatest number of patients. 7 However it is typical for lightning strike victims who do not experience cardiac or respiratory arrest to survive. 8 Focusing resuscitative efforts on patients found in arrest demonstrated the appropriate use of reverse triage strategy in a lightning MCI.3,8 The advanced life support providers who flew to the scene brought triage tags with them that were not used, likely because transport priorities were clear by the time helicopters arrived for evacuation. Although not classically associated with a wilderness setting, the use of triage tags keeps triage and treatment information with the patient. This information plays an important role in wilderness evacuation, especially when communication failure occurs. Wilderness rangers in SEKI are not provided with triage tags, and triage tags are not stocked in backcountry ranger stations. Although a wilderness MCI is a rare event, the extension of triage tag use to the backcountry should be considered.
There are limited evacuation options in the wilderness, including litter carry, stock evacuation, and aeromedical transport. These options are often further restricted by the specific situation. Evacuation or transport of any kind is generally not appropriate for patients in cardiopulmonary arrest. Chest compressions during patient transport have been shown to be ineffective, and patients requiring CPR should be treated and triaged on scene. 9 For a prolonged litter transport, the NPS recommends an average of 16 personnel owing to inevitable provider fatigue and a field estimate pace of 0.25 miles per hour (mph) in mountainous terrain. Knapik et al 10 showed that hand carrying a litter, while on a treadmill set at 3.0 mph, could not be continued longer than 2.7 minutes, on average, without rest. With a 5-minute break after each carry, these easy conditions correlate with a pace of 1 mph, assuming no issues with terrain navigation. Although faster, stock evacuation is not indicated for the altered patient who cannot stay secured to the animal. Because of these drawbacks, aeromedical evacuation, as in this case, is the most utilized and often the most appropriate wilderness evacuation option in SEKI.
Aeromedical rescue is not without limitations, especially considering that the 2 highest priority patients in this case were receiving ongoing CPR, and prioritizing them for transport may not be the best decision in a remote setting. Helicopter transport of patients with ongoing CPR is not common practice in our system, owing to logistical and safety issues of crews attempting chest compressions in a spatially constrictive area without a safety harness. Few controlled studies of sufficient quality and strength examining survival with prehospital advanced life support treatment exist. 11 Available evidence suggests aeromedical evacuation of victims of nontramatic 12 and traumatic13,14 cardiac arrest from remote locations have a negligible impact on patient survival.
Although the chance of successful resuscitation may be greater for patients who have cardiac arrest from lightning strike than for those with other causes of cardiac arrest,15,16 there is no good evidence suggesting that lightning strike victims benefit from longer than usual resuscitation times. 17 Analyzing this case indicates that juvenile 3 would still have been the top priority transport, as he had a carotid pulse of 100 beats/min. This priority would have changed had his pulse remained at 30 beats/min, thus requiring CPR under the pediatric advanced life support algorithm. With respect to adult 1, how long is long enough to continue resuscitative efforts in the case of lightning strike? In the opinion of the authors, if both patients had an ongoing need for CPR when aeromedical rescue options became viable, it would have been judicious to prioritize transport of the patient categorized as “immediate/red” using traditional START triage, namely, adult 4 who presented with neurological complaints and altered mental status (Table 2). Given the relatively higher rates of successful resuscitation of lightning strike victims and the low rates of acute complications among those who initially survive the strike, there remains some controversy regarding the appropriate triage priority. Transport times, manpower, and equipment resources also play into these decisions, and in this circumstance, the authors believe the appropriate triage decisions were made. 18
In this case, reallocation of evacuation resources to lower priority patients may have expedited evacuation efforts, and perhaps should have been considered given the persistent danger posed by remaining on scene. Two helicopters, H 552 (litter capable) and H 47 C (not litter capable), landed on scene with providers and equipment and left before any patient loading because of imminent storm risk. The highest priority patients could not be mobilized to the landing zone during this narrow window. For example, while adult 4, who was minimally responsive and nonambulatory, was being carried to the landing zone for H 552 evacuation, the helicopter crew was already in maneuvers to lift off for reasons of operational safety. With better communications, these air resources could have been used to provide an expedient evacuation of ambulatory patients. It is also unknown whether H 47 C, a small aircraft without a medically trained crew, was considered as potential transport for “minor/green” patients at this initial departure. It was used for that purpose later in the rescue effort. Reprioritization would have meant a majority of the minor victims had access to shelter safe from further lightning injury, but potentially would have delayed definitive care for the most critical patients. Knowing when to break policy is a judgment call. In this case, it is interesting to note that final evacuation priorities mirrored the current MCI procedure (Table 2), with the exception of prioritizing transport of juvenile 3, a victim the policy categorizes as “black/deceased.”
The pilots involved in this incident had to balance the dangers to the persons remaining on the ground against regulations regarding safe helicopter use in mountainous terrain. Since August 2004, the Federal Aviation Administration (FAA) has promoted more training regarding safety, and advocates that aviation safety decisions remain separate from medical decisions. 19 Occurring late in the afternoon, this incident quickly approached the limit of visual flight rules, which restrict helicopter flight to 30 minutes before official sunrise and 30 minutes after official sunset. 20 Mountainous terrain causes additional restriction of visual flight periods, as light is diminished by the relationship of the sun to the peaks. The FAA recommends the use of terrain awareness warning systems for EMS helicopters but they are not mandated. Air operations in the Sierra Nevada mountains frequently occur above 10,000 feet (3,000 m), and in some instances may require supplemental oxygen onboard. 20 Wind restrictions are also in place for light helicopters, limiting flight below 500 feet (takeoff and landing) in steady wind of 30 knots or gusts of 15 knots. 20 For persons on the ground who need to estimate whether these conditions exist, knots can be roughly converted to miles per hour, meaning that a typical fast-moving summer storm could produce 15 mph winds that would interfere with aeromedical rescue.
Safe helicopter use in rescue situations includes mission risk assessment and appropriate response crews for the situation. The NPS utilizes a commercial helicopter EMS request mission risk assessment card (Figure 6) to determine the overall risk of the mission. 21 The director of flight operations for the EMS helicopter agency is required to determine approval of any high-risk mission. 22 However, transporting patients in helicopters not specifically designated as aeromedical is common in emergencies such as in this MCI search and rescue setting. Aeromedical transports may not be the most appropriate scene-capable aircraft, and medical crews may not be adequately trained in wilderness scenarios. Evacuating to a helicopter base where patients are transferred to EMS units, as was done here, is a common strategy.
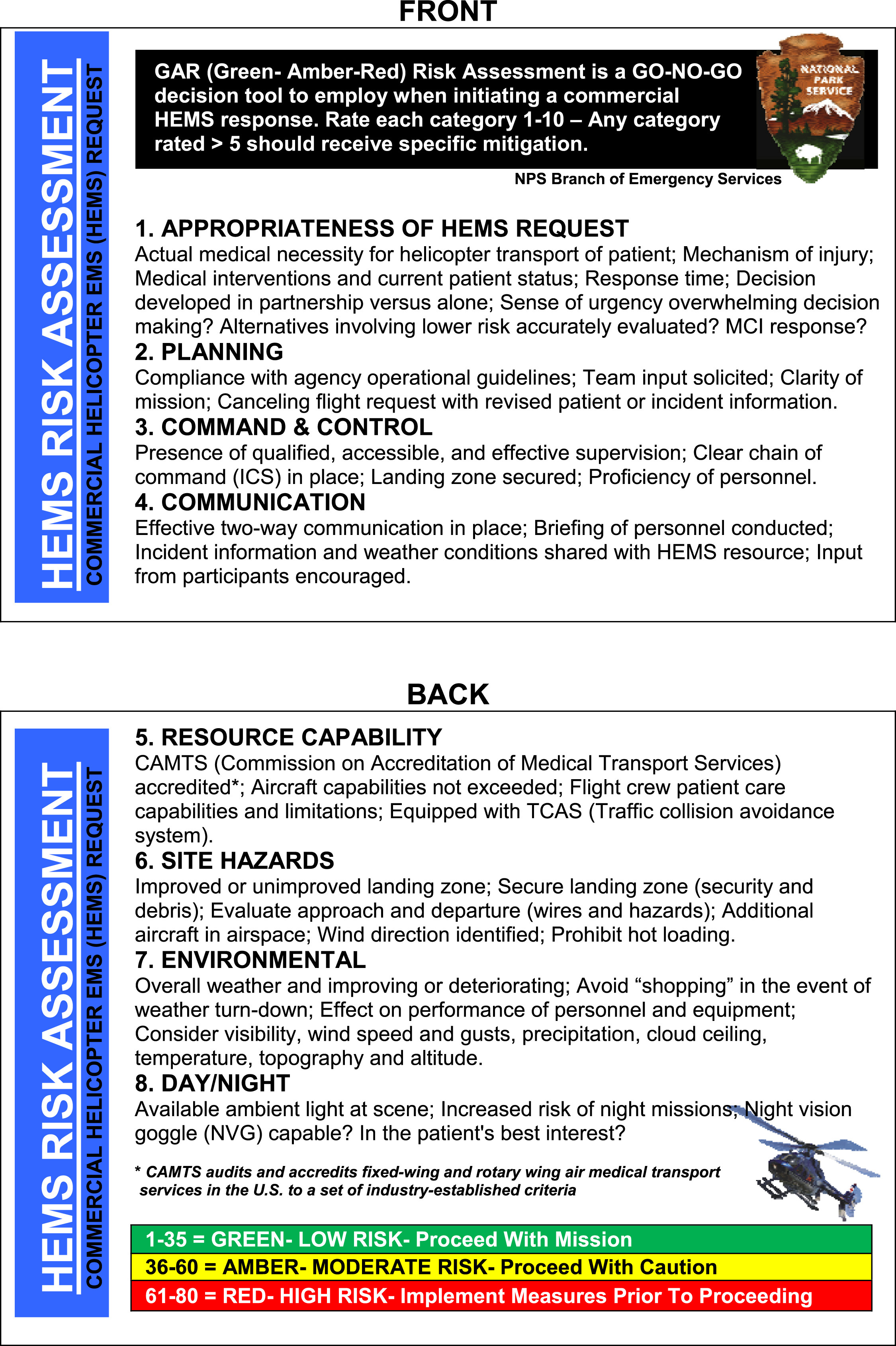
Helicopter emergency medical services (HEMS) risk assessment card.
An analysis of the ways in which communications were and were not compromised affects planning for future events. The initial analog radio report from Crabtree Ranger Station to dispatch triggered the deployment of air resources and medical and incident command personnel without any complications. The intense thunderstorm cell was so localized that the weather at Crabtree, only 1 mile from Sandy Meadow, was unremarkable at the time of the incident. Analog radio systems (high or low frequency) can use tones, wideband (25 MHz) or narrowband (12.5 MHz) signals, susceptible to interference from static buildup in the air and clouds. 23 Once at Sandy Meadow, static and loud wind interference rendered the low-frequency radios nearly unusable on the ground. In the air, all agency-owned, contract, and rental aircraft have a very high frequency (VHF-AM) radio for communication with FAA facilities. 23 These radios are less vulnerable to electrical storm interference; therefore, the air crews were able to maintain contact with dispatch and incident command throughout the operational period. Even more resistant to electrical interference, ultrahigh frequency (UHF) systems such as satellite were not available in the backcountry at the time of the incident. Today, all SEKI wilderness rangers are issued radios, satellite phones and GeoPro satellite tracking devices. Use of satellite technology is now common in many parks for communication and employee tracking in remote areas. Since this incident, the system has transitioned from analog to digital, radios have been upgraded, and the repeater system has been adjusted frequently to improve its performance. However, even the most sophisticated communication systems are limited by battery life, range, and transmission and receiving voids in remote mountainous environments. The need for redundancy in communication strategies, as was ultimately effective in this case, cannot be overemphasized regardless of technological advances.
On review of this case, several issues stand out as take-home points for future training, education, and research. First, the parkmedics at the scene had prepared to stay overnight in the meadow with the injured and deceased victims until first light. However, incident command had better information regarding weather, enabling a coordinated helicopter rescue. That underscores the largest problem often faced by those managing MCIs, namely, communication is frequently the most crucial and tenuous resource. This incident illustrates the need for redundancy in all communication systems, from triage tag use to having multiple technologies to communicate remotely. Second, there are regulations on and limits to aeromedical rescue. Wilderness providers at all levels, from wilderness first responder to base hospital physician, should know these limitations to maximize safety in future operations. Third, given the poor outcomes seen with long transport times, regardless of injury mechanism, triage priorities in remote settings should be further researched and debated. Furthermore, development of disaster management practice guidelines for use in remote environments may better address these challenging scenarios, from lightning strikes to fires to alpine plane crashes, where evacuation may not be measured in hours, but days.
Conclusion
Exposure to environmental dangers, such as lightning in this case, and an increased length of time, both on scene and in transport, can dramatically affect the outcome of a wilderness rescue and affects both patients and rescuers. In the NPS, the parkmedic level of training and scope of practice is designed to address this unique environment. The responding team must take into account the risks a wilderness rescue places on their personal safety, as well as changing weather, daylight, and terrain. Helicopters are often the main vehicles of rescue, and as seen in this case, communication becomes a key factor in the success of such a rescue. Redundancy should be built into communication systems, and written protocols established and understood by all rescuers, ground and air crew alike. With regard to a lightning-induced MCI, reverse triage should be implemented, and education for both wilderness travelers and rescuers regarding this issue should continue to be pursued, as it has been shown to save lives.