
Abstract
Extracting a tooth is the final treatment for multiple dental problems. Persons who are not dentists, however, have little experience with tooth extractions. When a remote setting makes it impossible to send a patient for optimal dental treatment, the clinician may need to extract teeth, sometimes using improvised equipment. The following cases of two patients with three carious, painful molars describe such a situation. The non-dental clinicians had to improvise not only appropriate dental tools, but also personal protective equipment, a functional suction machine, medications for a dental block, a dental chair, and dental consent forms and follow-up instructions in the patients’ language. In these cases, they also communicated with their patients through a translator. To prepare to do tooth extractions in remote settings, clinicians should learn and practice dental blocks and review extraction techniques before they deploy. If they must do an extraction, clinicians should use the closest approximation available to the appropriate dental tools. When done correctly, a dental extraction can take some time and should not be rushed.
Introduction
Two crewmembers from a research fleet support vessel had severe dental pain due to carious molars. At that point, the ships were in Baffin Bay (62 degrees longitude; 74 degrees latitude), about 150 nautical miles off the remote Greenland coast. With almost no dental equipment aboard and the closest (and only) regional dentist having traveled to northern Greenland to provide before-winter dental care, it fell to a fleet emergency physician and medic to deliver definitive dental care using improvised equipment.
A medical history was obtained by e-mail from both patients before they were transferred to the base ship for dental care. Neither had any significant medical problems or was taking any medications unrelated to their dental pain. When they arrived on the base ship, a brief medical examination confirmed, as much as possible under the conditions, that they were both in good health.
Case Presentations
Case 1
A 37-year-old Russian sailor presented with sharp shooting pain that had started 3 days previously when he broke a tooth while eating. Rating the constant pain as 8/10, he had been self-medicating with Ketanov (ketorolac). For more than a month he had had milder tooth pain, which had improved on self-administered Amoksiklav (amoxicillin/clavulanic acid). The pain was now limiting his eating and sleeping. His last dental check had been five months earlier. A photo sent from his ship showed a broken first right lower molar (30 according to the Universal Numbering System [UNS]; 46 according to the Fédération Dentaire Internationale [FDI], World Dental Federation notation) with a temporary filling and overgrown gingiva.
After contacting the regional dentist by e-mail and phone, she helped define the problem and recommended extraction. She wrote, “It seems that the patient has a broken composite filling in his molar and a temporary filling (the white material). The gingiva is covering some of the tooth, so it seems that the tooth has been broken for some time. It needs extensive dental work to repair. With this much pain, he needs a root canal with extirpation of the dental nerve, and then a crown. [Only 1 dentist in Greenland could do that, and he was too far away to help.] Because of the circumstances, the best treatment is for you to remove the tooth and relieve the man’s pain.”
Case 2
A 40-year-old Russian from the same ship arrived with the first patient. He had significant pain in his remaining 2 left upper molars, 15 and 16 UNS (27 and 28 FDI). A piece was missing from the lingual side of the second molar and large contiguous caries affected both teeth, exposing the pulp. He had extensive prior dental work on the second molar. The dental consultant also advised extracting these teeth.
Procedure for Both Patients
After transferring the patients to the main research vessel, a bilingual, native-Russian crewmember, with help from his pocket translator, facilitated communication. After explaining the proposed procedure, including the lack of standard dental tools, both patients read and signed a consent form in Russian to further assure their understanding. No radiographs were possible, because the on-board machine could obtain only extremity films.
Advance Preparations
Personal protective equipment included gowns fashioned from plastic garbage bags, borrowed painter’s masks, and personal eyeglasses. We had barely enough gloves to do the procedures, and because we could not position the overhead surgical light adequately to illuminate a patient’s mouth once he was in the chair, we used our personal headlamps. The patients used chlorhexadine mouthwash as a preprocedure rinse to reduce the chance of developing alveolar oseitis.
To perform dental blocks using the only available local anesthetic solution, we first had to make a 1% lidocaine-epinephrine 1:200,000 solution using the following method: 1 1) add 0.1 mL (0.1 mg) epinephrine 1:1000 to 19.9 mL (19.9 mg) of 1% lidocaine; 2) the total solution is now 20 mL, and the original epinephrine has been diluted 200 times (1:200,000 solution); and 3) label and refrigerate the solution until needed.
Next, we had to devise an adequate suction device and obtain suitable “dental” tools. Lacking liners for the suction unit (Laerdal Suction Unit 78002001, Stavanger, Norway), our medic improvised a container by using standard oxygen bubble tubing to connect the suction unit’s vacuum outlet to a spare oxygen concentrator reservoir (HUM AEROpart Humidifier, HAB01-916, Lünen, Germany). Additional bubble tubing was used to connect the other outlet on the suction unit to the suction tubing and Yankauer suction device, although a plastic intravenous catheter may have also functioned well. Electrical tape was used to seal any vacuum leaks. We used saline-filled syringes for irrigation.
Extractions
On examination, all 3 teeth were stable, but their pulp was exposed. A Gow-Gates mandibular block 2 was performed on patient 1 with the lidocaine-epinephrine mixture. Patient 2 received supraperiosteal injections. Both patients had supplemental supraperiosteal injections as their procedure progressed.
After incising the periodontal ligaments with a tiny flathead screwdriver, the teeth were leveraged against adjacent teeth using a tiny right-angled screwdriver. The 2 adjacent carious molars were leveraged against each other. Eventually, the affected teeth became mobile. Once a tooth was sufficiently mobile to grasp it adequately, rotation and leverage allowed it to be extracted. Each tooth was grasped with a small smooth-jawed pliers below the gum margin and rocked lingually (inward) and buccally (outward) in a figure-of-8 manner, pausing at the “top” and “bottom” of the 8 for about 5 seconds. Two of the 3 teeth were extracted intact. On the third tooth, a restoration came off first, and then the balance of the tooth was extracted in 1 piece.
After the extractions, we placed a cotton dental roll over the sockets, and the patients were instructed to bite down on it. There was no significant bleeding. The patients began taking oral penicillin and acetaminophen before departing for their ship. They would take ibuprofen, as needed, beginning 72 hours after extraction. They received and read a copy of standard postextraction instructions in Russian. Follow-up was by e-mail and radio contact through their ship’s on-board English-speaking medic. Had it been necessary, the clinicians would have rechecked them in person.
Discussion
Frequency Of Dental Problems On Remote Expeditions
Dental problems occur frequently in remote settings. Researchers have found that between 12% and 38% of offshore workers have tooth decay and 35% to 60% have gum disease or infection. Another 19% have failed restorations or problems after dental treatment.3,4 Several studies show that dental problems comprise 5% to 14.6% of all medical evacuations. 3 –6
The logical solution would seem to be to require dentists (or physicians, which is often the norm) to examine personnel before deployment. Yet, when 2 remote populations with and without such examinations (members of the British Antarctic Survey and offshore oil and gas workers, respectively) were compared, the difference in occurrence of their dental problems while deployed was insignificant. 7 The US Air Force reported that, despite prescreening, dental problems constituted 22% of emergency department visits on a 2003 deployment. 8 Limited data suggest that during a single 4-month period, they subsequently decreased their rate of dental emergencies (2.7% annualized) with improved prescreening. 9
Reasons For Extraction
Pain is the most common presenting dental complaint. Most dental pain is due to inflammation in a closed space: within the pulp of the tooth, within the bone, or beneath the periosteum. Relieving the pressure, generally by extracting the tooth, typically eases pain stemming from pressure within the pulp or bone. Incision and drainage relieves pressure from subperiosteal abscesses.
Given the difficulties with extractions in remote locations, teeth should be extracted only when absolutely necessary. Consideration should be given to the use of analgesics and antibiotics and the application of medicated temporary dental fillings as an alternative to extractions. These medicated fillings often contain eugenol, which acts as a sedative to treat diseased nerve-pulp tissue. Although temporary, they can often last quite a while or until conventional dental services are available. In the presence of a frank abscess with palpable lesion, incision and drainage along with antibiotic therapy may be the preferred option.
However, extractions in austere circumstances may be necessary, if not the only available option. In general, reasons to extract a tooth 10 are 1) the patient has constant pain from the tooth; 2) the tooth is already broken with an exposed nerve root; or 3) the tooth is loose and painful when moved. In the cases presented, not only did each patient present with both of the first 2 indications, but they also had used both antibiotics and analgesics without significant relief and, for both logistical and visa-related reasons, had no reasonable expectation of getting formal dental care in the near future.
Improvised Equipment And Medications
Once the clinicians decided to extract the teeth, many items needed to be prepared. A dental consent form was downloaded from the Web, and a postextraction patient instruction sheet taken from a textbook. 11 We converted both into Russian using an online translator, 12 and our Russian interpreter made a few minor changes. Searching for a suitable dental chair that would support the patient’s head, we borrowed the captain’s office chair, covered it in plastic garbage bags, and wedged it into the tiny space between the immobile clinic stretcher and some cabinets. We considered using sedation rather than or as a supplement to dental blocks, but decided that it would be too dangerous: after the procedure, our patients had to return to their ship on a small boat over choppy Arctic waters and then climb aboard using an unstable Jacob’s ladder.
We scrounged improvised dental tools from the electrical, engineering, and instrument departments. These included tiny screwdrivers to explore and cut periodontal ligaments, small right-angled screwdrivers to lever the teeth, small wire pliers to grab the teeth, and nonserrated flat pliers to firmly grip the molars (Figure 1; Figure 2 illustrates the comparable equipment that dentists normally use). An important question for those planning remote medical operations is, why were these clinicians put in a situation where they had to improvise the necessary medications, supplies, and equipment? The answer seems to be that there was poor planning and inadequate logistical support. 13
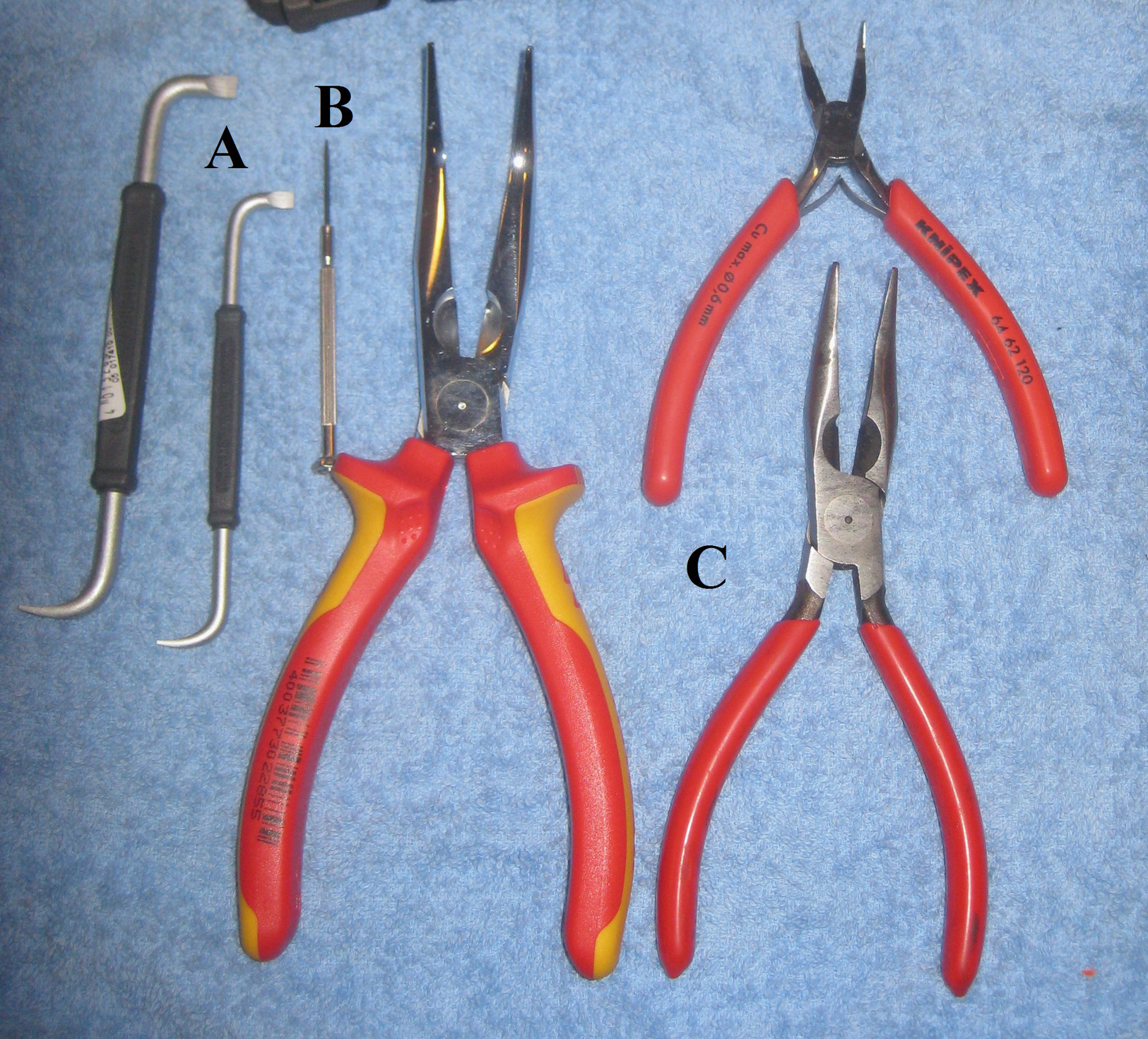
Improvised tools used for dental extractions in this case: (A) right-angled screwdrivers; (B) Mini screwdriver; and (C) Various pliers.

Comparable tools used by dentists and oral surgeons: (A) elevators; (B) root elevators; and (C) universal extractors, lower (left) and upper (right).
Tooth Extraction Technique And Procedural Steps
In old-time movies, tooth extractions appear to be a simple procedure. In reality, extraction is difficult to accomplish without breaking the tooth, even with modern surgical tools.11,14
The keys to successful extractions are patience and finesse. Rather than simply pulling a tooth out, the basic principle is to break the periodontal ligaments that hold the tooth to the bone and then rock and lever the tooth out. Slow gradual luxation of a tooth with either an elevator (screwdriver) or forceps (pliers) is crucial. The bone will expand and the inflammatory process in the periodontal ligament that follows luxation further loosens the tooth. Attempting to yank the tooth will only break it off.
Root fractures are particularly common in nonmobile molar teeth, such as in the cases in this report. However, most retained roots are not a problem, and experienced dental practitioners know that they will eventually come out on their own, will remain in place without causing a problem, or, especially if surrounded by infected tissue, will be the focus of an abscess that can be drained through the gum and the root removed.
There are various dental extraction techniques. Although dental forceps and elevators are the hand tools dentists use for extractions, clinicians in unusual circumstances may need to improvise these tools. The following steps illustrate a process that can be used in remote settings. Positioning the patient. Position the patient correctly. Seat the patient in a chair with a high back that will support the patient’s head. Patients who need a lower tooth extracted should be sitting lower than the clinician, because to extract the tooth requires pushing down and then pulling up on the tooth. Patients who need an upper tooth removed should sit higher than the clinician, because that extraction technique is to push up and then pull down on the tooth. Anesthesia. After the patient rinses his mouth with chlorhexadine, if available, do a dental block. Supraperiosteal injections, commonly used for maxillary teeth, are the easiest to learn and administer. Inferior alveolar blocks are the easiest to learn for mandibular teeth. Alternatives are the Gow-Gates, palatine, and for upper incisors, infraorbital blocks. (Mental blocks are ineffective for mandibular incisors.) Your position. Position yourself correctly. Right-handed clinicians should stand behind and to the right of the patient when extracting lower right molar or premolar teeth. When working on all other teeth, clinicians should face the patient and stand to the patient’s right. Separate tooth from alveolar bone. To remove the tooth, first separate the tooth from the bone. The attachments (periodontal ligaments) are strong, but thin. Push a sharp dental instrument, or a tiny screwdriver or blunted needle as a substitute for the dentist’s periosteal elevator, between these attachments and the tooth. Then separate the tooth from the bone by moving the tool back and forth. Do this on both the buccal (cheek) and the lingual (tongue) side of the tooth. Take care not to go too deep, and to cut only the attachments to the tooth.
10
Leverage. Next, loosen the tooth, because a firmly attached tooth will break if you do not loosen it first. Without proper dental tools, this step is vital, although with standard dental extractors, it is often omitted to avoid damaging the adjacent tooth. Place a thin blade (in our cases, a tiny right-angled screwdriver substituted for a straight dental elevator) between the bad tooth and the good one in front of it or between 2 adjacent teeth that need extraction. Turn the handle so that the blade moves the top of the bad tooth backward and loosens it. Grasp tooth. Support the gum and underlying bone with the thumb and finger of your nondominant hand and apply the forceps-grasping tool (in place of a dental extractor) to both sides of the crown, parallel with the tooth’s long axis. Grasp the tooth’s root beneath the gum line. Although it was not available for our patients, this tool should be shaped to adapt anatomically to the surface of the tooth’s root. The lingual jaw of a pair of pliers (called a “beak” on a dental extractor) should be seated first, followed by the buccal jaw. Push your grasping tool (extractor, pliers, and so forth) as far toward the roots as possible. Clinicians working in remote areas who anticipate doing extractions may want to have a universal upper and lower adult extractor available. Luxation, namely, dislocation-rocking. Rather than “pulling” the tooth, rock it back and forth to expand the tooth socket.
15
Move the tooth differently, depending upon how many roots it has. If a tooth has 1 root, rotate it. If a tooth has 2 or 3 roots, tip it back and forth, mostly in the labial and buccal directions, toward the thinner alveolar bone. Use a deliberate and slow motion, gradually increasing in force. If the tooth does not begin to move, loosen the forceps, push them deeper, and repeat the rocking movements. Some dentists prefer to push the tooth down and rotate it in a figure-of-8 pattern, with movement in each direction lasting 8 seconds. Rest period. No matter which methods you use, take your time. As Dr Murray Dickson wrote in Where There Is No Dentist, “Removing a tooth is like pulling a post out of the ground. When you move it back and forth a little more each time, it soon becomes loose enough to come out.”
10
To make the process easier, once the tooth begins moving, let it “rest” for 20 to 30 minutes and then attempt to extract it. This “resting period” allows blood to infiltrate into the periodontal ligament space, creating additional separation and pressure between the roots and the bone. Extracting the tooth. Once the alveolar bone has expanded sufficiently and the tooth has been luxated, the clinician can use relatively minimal traction, usually directed buccally, to extract the tooth. If the tooth is not loosened at this point, traction may fracture, rather than remove, the tooth. Hemostasis. Once you extract the tooth, stop any bleeding by squeezing the sides of the socket for 1 to 2 minutes, and then have the patient bite firmly against cotton gauze or absorbent cloth for 30 minutes. Tooth inspection. Carefully inspect the extracted tooth to confirm that its removal is complete. Postextraction care. Give the patient after-care instructions.
Conclusions
Tooth extraction is the final treatment for multiple dental problems, but often can be delayed, if not avoided by using analgesics and antibiotics to allow enough time to send the patient to a dentist for optimal treatment. When this cannot be done, attempt to use available communication methods, including photographs, to consult a dentist or oral surgeon for confirmation of your clinical decision and for additional advice on the extraction procedure. To prepare to do tooth extractions in remote settings, learn and practice dental blocks and review the extraction technique before the trip. Use the best possible equipment available that most closely approximates the appropriate tools; improvise when necessary. If done correctly, a dental extraction may take some time and should not be rushed.
Recommendations that could lessen the need for improvised tooth extractions in remote circumstances are 1) to have both physicians and dentists do predeployment screening; 2) to provide adequate dental equipment, especially for large, extended expeditions; and 3) to give physicians in these circumstances basic hands-on dental training. The usefulness of dental screening may be questionable, especially when the quality of the screen is not assured.
Footnotes
Acknowledgments
Thanks to Richard M. Wills, RODP, the on-board medic who improvised the suction device, and to Michael Grossman, DDS, Dan Klemmedson, MD, DDS, DMD, and General Lee Payne, MD, MBA (USAF) for providing information or reviewing the manuscript.