
Abstract
Emergent cricothyrotomy is an infrequently performed procedure used in the direst of circumstances on the most severely injured patients. Austere environments present further unique challenges to effective emergency medical practice. Recently, military trauma registry data were searched for the frequency of cricothyrotomy use and success rates during a 22-month period. These data revealed that cricothyrotomy performed in the most rigorous austere environment (ie, battlefield) had many successes, but also a large number of failed (33%) attempts by medics owing to many factors. Thus, the aim of this review article is to present what is known about cricothyrotomy and apply this knowledge to any austere environment for qualified providers. The National Library of Medicine's PubMed was used to conduct a thorough search using the terms “prehospital,” “cricothyroidotomy,” “cricothyrotomy,” and “surgical airway.” The findings were further narrowed by applicability to the austere environment. This review presents relevant airway anatomy, incidences, indications, contraindications, procedures, and equipment, including improvised devices, success rates, complications, and training methods. Recommendations are proffered for ways to optimize procedures, equipment, and training for successful application of this emergent skill set in the austere environment.
Introduction
Medicine in the austere environment is uniquely challenging because many factors such as logistics, manpower, and evacuation must be considered in addition to patient care. An emergency cricothyrotomy performed in the austere setting illustrates the “principles versus preferences” of medical care, an adage that is frequently described by Norman McSwain, MD. 1 With regard to surgical cricothyrotomy, the principle is the requirement to open the airway through the cricothyroid membrane to oxygenate, ventilate, and protect the airway. The preference is how the principle is realized using the cricothyrotomy procedure and tools of choice. Even though there are many cricothyrotomy devices and procedures, not all are relevant for use in the austere environment. Thus, the intents of this review are to present what is known about cricothyrotomy and apply this knowledge to austere environments, and to give recommendations for optimizing procedures and training for successful skill application.
Background
Airway management is not only a top priority in initial resuscitation—it quite literally is the difference between life and death for many critical patients. In fact, airway control is one of the few procedures in prehospital emergency care that significantly affects outcome in the critically injured patient. 2 There are myriad modalities for securing a definitive airway, although the most common is endotracheal (ET) intubation. Yet, all difficult airway algorithms have a common final pathway ultimately leading to cricothyrotomy.3,4 A surgical cricothyrotomy is almost always a procedure of last resort because of its invasiveness and provider comfort or lack thereof. 5 Most patients who require cricothyrotomy in the emergency department (ED) have failed multiple ET intubation attempts and are possibly critically hypoxic, requiring further intervention. In the prehospital setting, most cricothyrotomy candidates have either cardiac arrest or blunt trauma and failed ET intubation attempts. Survivors frequently have poor neurological outcome and high mortality rates. 6 –8 In austere settings, the use of ET intubation and supraglottic devices may not be possible or appropriate because of tactical or situational constraints, even when appropriate for the patient. Thus, cricothyrotomy is even more relevant in these environments. 9 –12
Although cricothyrotomy is becoming less common as other alternative airway devices are introduced, such as the laryngeal mask airway, King LT-D (King Systems Corp, Noblesville, IN), and other supraglottic devices, there is, and likely always will be, a role for cricothyrotomy in a subsection of patients with difficult airways, especially in environments in which such devices are unlikely to be available. A common emergency medicine aphorism is: “If you do one cricothyrotomy, you're a hero; if you do two, work on your airway skills.” True perhaps in a hospital, but in an austere environment many factors besides failed ET intubation lead to early cricothyrotomy. Wilderness providers must be not only technically skilled, but also adequately trained to recognize the key indications and situational decision triggers for cricothyrotomy that differ from in-hospital practice.
Research on cricothyrotomy varies in terms of the procedures and tools evaluated. Additionally, outcomes such as procedure time, success rates, and complications, as well as other variables (eg, training models, research environments, provider level and specialty, and patient-related factors) are not uniform across studies. Furthermore, cricothyrotomy is, at most, an infrequently performed procedure, and research on trauma and emergent patients is exceedingly difficult. Case studies and retrospective analyses abound, but there are few prospective, randomized, controlled, crossover studies. This review will focus on surgical cricothyrotomy outside the hospital setting, but draw from hospital-based studies when relevant to the performance of this procedure in austere environments.
Anatomy
Sound anatomic knowledge and a good technique are synonymous. The landmarks are obvious, but this simple procedure becomes an adventure when the landmarks are obscured—S.D. Eyer, MD6(p835)
To be successful, an intimate familiarity of the underlying laryngeal anatomy is essential. Tube misplacement is the main reason for cricothyrotomy failure.13,14 Correct identification of landmarks is even more difficult in austere environments owing to limitations of sensory perception, poor lighting, lack of equipment, and added environmental stressors. Boon and others state that solid knowledge of the anatomy is imperative to lessen complications, and is a key component in reducing anxiety among providers.15,16
Landmarks
Anatomical landmarks for cricothyrotomy are located in the anterior midline of the neck. From superior to inferior they are as follows: 1) hyoid bone; 2) thyrohyoid membrane (also known as the thyroid membrane); 3) thyroid notch; 4) thyroid cartilage; 5) cricothyroid membrane; and 6) cricothyroid cartilage and sternal notch (Figure 1). In most patients, it is fairly easy to palpate the thyroid cartilage, particularly in males, while sliding down the midline with the index finger from the thyroid notch (located on the superior border of the thyroid cartilage). The cricothyroid membrane is located just inferior to the large thyroid cartilage and superior to the cricothyroid cartilage. The only complete cartilage ring in the larynx and trachea is the cricothyroid cartilage, which is important for airway patency before and particularly after a cricothyrotomy. These landmarks are easiest to identify when the neck is extended. 17
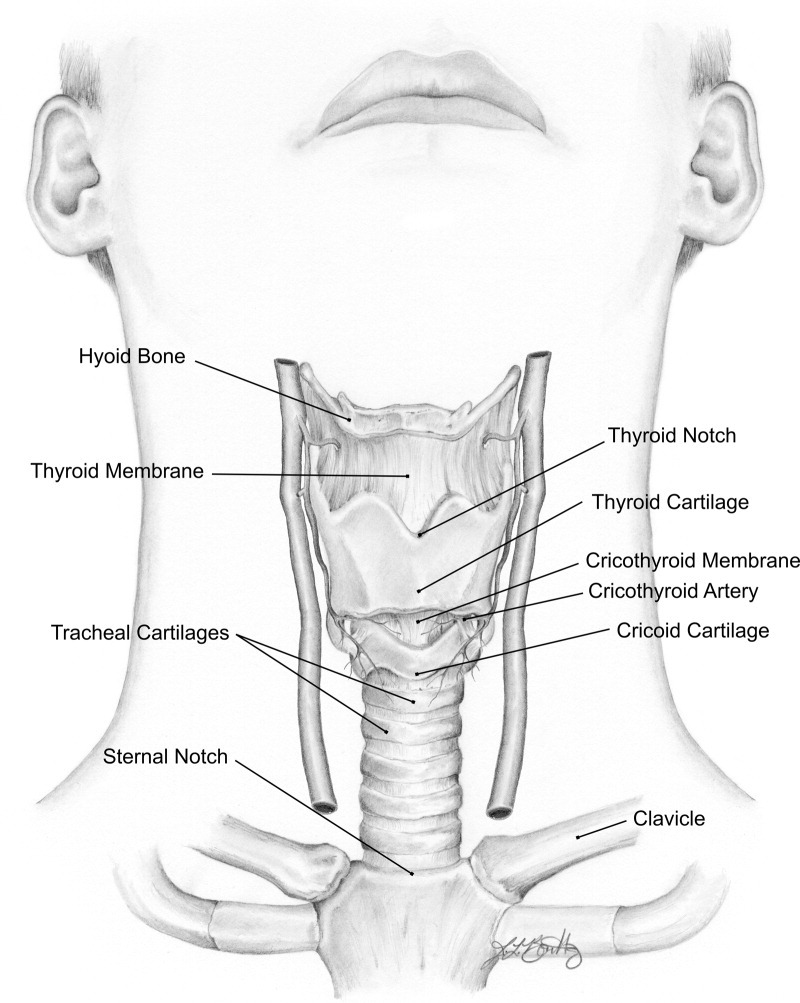
Anatomy of the larynx.
Elliot et al 13 studied 18 anesthesiologists to determine whether they could correctly locate the cricothyroid membrane on 6 adult humans within a 10-second period, simulating an urgent cricothyrotomy. The anesthesiologists correctly identified the cricothyroid membrane only 30% of the time. These authors and others suggest that ultrasound may elucidate difficult anatomy and ensure correct cutaneous point of entry overlying the cricothyroid membrane. 18 Ultrasound's availability for use in austere environments is increasing in specific settings, eg, disaster medicine, high altitude clinics, and military forward aid stations, but normally would not be available. It is important to note that the use of ultrasound to identify anatomical landmarks for cricothyrotomy has not been validated clinically to improve success rate and decrease complications. 18
Owing to soft tissue swelling from trauma, traditional anatomical landmarks can be very challenging to feel, which may delay an emergent cricothyrotomy.19,20 Clues for use when landmarks cannot be palpated because of trauma or obesity are that the cricothyroid membrane can be found 1) approximately 1 to 1.5 fingerbreadths below the laryngeal prominence (thyroid cartilage) in the neck midline; and 2) 4 finger widths (index, middle, ring finger, pinky) above the superior border of the sternal notch.5,17 The general location of the cricothyroid membrane can also be approximated using the angle of the mandible and hyoid bone. 21
Cricothyroid Membrane
The cricothyroid membrane is a dense, trapezoidal fibroelastic membrane between the inferior border of the thyroid cartilage and the superior border of the cricothyroid cartilage. The cricothyroid muscles border the cricothyroid membrane laterally. The average dimensions are 8.2 mm wide and 10.4 mm high, with women having consistently smaller cricothyroid membrane dimensions than men. 16 Based on this size the cricothyrotomy tube's outer measurement should not exceed 8 mm. 22 Many commercial kits now use a 6-mm tube, small enough for easy insertion and reduced risk of cartilage fracture, while still large enough for adequate ventilation.
Vasculature
A vertical midline incision will avoid all major vessels of the neck. Boon et al 15 reported no major arteries, veins, or nerves in the cricothyroid membrane region, yet Dover et al 16 reported extensive collateral anastomoses in the area. Interestingly, the cricothyroid artery transverses the upper third of the cricothyroid membrane in 93% of 15 cadavers. 16 Even though the cricothyroid artery is not considered clinically significant, 15 a transverse stab through the lower portion of the cricothyroid membrane adjacent to the cricothyroid cartilage is recommended to avoid this small artery.5,16 The location of the cricothyroid artery may account for the fact that some surgical cricothyrotomies are bloody whereas others are not.
Vocal Cords
The vocal cords are attached to the thyroid cartilage and are at least 1 cm superior to the incision through the cricothyroid membrane. 5 Tube insertion should be aimed caudally to avoid injuring the vocal cords via retrograde intubation. Other complications relating to anatomical considerations and the techniques to avoid them are discussed below.
Incidence, Indications, and Contraindications
Incidence
Cricothyrotomy usage has decreased during the past 2 decades primarily in the ED, in large part because of less invasive adjuncts such as the laryngeal mask airway, Combitube (Kendall-Sheridan Catheter Corp, Argyle, NY), and King LT.23,24 These supraglottic devices have reduced the number of patients in the “can't intubate, can't ventilate” (CICV) category. 24 Furthermore, the increased use of neuromuscular blocking agents for rapid sequence induction has increased the success of nonoperative airway management. Walls et al 25 reported 8937 intubations across 31 EDs based on a multicenter trauma registry from September 1997 to June 2002. Of these, the need for surgical cricothyrotomy occurred 17 times (0.19%). This low incidence of ED cricothyrotomy is less than other studies reporting 1.7% to 2.7% of all attempted intubations, and 2.1% to 14.9% of attempted intubations in the prehospital setting. 2 ,6,25,26
A compromised airway is the third potentially preventable cause of death on the battlefield 10 and results in 1% to 2% of all combat fatalities in modern military conflicts. 11 ,27,28 Mabry and Frankfort 29 state that the surgical cricothyrotomy procedure in combat casualties has a much higher incidence rate and is nearly double that reported for civilians (0.32% vs 0.62% of trauma admissions, respectively). Furthermore, these authors state that airway deaths are low compared with hemorrhage on the battlefield. However, the impact of airway-related injuries from inadequate oxygenation and ventilation is not known. 29
To date, there has been only one case report of a surgical cricothyrotomy performed in the wilderness setting. Wharton and Bennett 30 reported using a surgical cricothyrotomy on a 31-year-old rock climber who fell 24.4 m (80 feet). Endotracheal intubation was impossible owing to oropharyngeal bleeding and facial fractures, which created an unstable airway especially when placed in a supine position during prolonged litter evacuation. Most likely there are other cases in which a surgical cricothyrotomy has been improvised in a wilderness setting, but they have not been reported.
Indications
Common indications for surgical airway intervention in any situation are oropharyngeal hemorrhage, edema of the glottis (as seen with anaphylaxis or inhalation injuries), facial trauma, anatomic abnormalities, trismus, or other CICV scenarios. 2 Trauma is by far the most frequent indication, reported in 82.4% to 100% of cricothyrotomy patients.6,8 Fortune et al 6 retrospectively examined 15 686 trauma cases over the course of 5 years in which 376 patients required prehospital advanced airway intervention. Within this group, 56 patients (14.9%) received a prehospital cricothyrotomy, an unusually high figure reported for use in the prehospital setting. The 5 leading indications for cricothyrotomy were facial fractures (32%), blood in the airway (30%), failed intubation attempt (11%), clenched teeth (9%), and traumatic airway obstruction (7%). McIntosh et al 31 reported similar findings for use of cricothyrotomy by emergency medical service (EMS) flight crews. The need for this procedure exists in the backcountry for head and facial trauma, airway swelling for anaphylaxis, or any other incident resulting in a CICV scenario.
In a study by Adams et al 8 from Operation Iraqi Freedom, 5.8% of the 293 casualties needing advanced airways received a cricothyrotomy, and the vast majority (97%) of those who needed airway intervention were trauma patients. Other data by Mabry et al 9 indicate that 18 of 982 battlefield casualties had airway compromise as the most likely primary cause of death. Of these 18 cases, all had traumatic injury to the face and neck. Nine casualties had multiple injuries to major vascular structures with significant hemorrhage. In 5 of 9 cases a surgical cricothyrotomy was noted at autopsy.
The challenges of combat and other wilderness situations, such as longer medical procedure time, light constraints, 32 or complicated positioning or extrication, 33 may necessitate cricothyrotomy vs conventional airway management. Thus, the indications for cricothyrotomy in these settings are broader than the indications when this procedure is used in the hospital. Additional patient-related factors that may require cricothyrotomy in the austere environment include suspected cervical spine trauma and a “crashing” patient without intravenous access along with one or more physiological indices (eg, Glasgow coma score < 8, oxygen saturation < 80%, systolic blood pressure < 80 mm Hg). 8
Since 1996, the Tactical Combat Casualty Care guidelines recommend airway management with either manual airway maneuvers, nasopharyngeal airway, or casualty recovery position. 10 When these efforts are unsuccessful, a surgical airway should be considered, but only after allowing a conscious patient to maintain his own airway by sitting and leaning forward so blood drains out of his mouth. 11 A position of comfort should take precedence as supine positioning may create a preventable airway emergency. This same approach to airway management has been adopted by the civilian law enforcement for tactical emergency medical support 12 and seems appropriate to most wilderness settings as well.
Contraindications
The loss of airway patency is not compatible with life; thus it is generally stated that there are no absolute contraindications to cricothyrotomy. 34 The only absolute contraindication to cricothyrotomy is the ability to secure an airway with less invasive means, 35 but this is not always an option in austere environments. 10 Airway trauma that renders cricothyrotomy a hopeless procedure, such as tracheal transection in which the distal end retracts into the mediastinum or a significant cricoid cartilage or laryngeal fracture, can also be absolute contraindications. 35 Relative contraindications to surgical cricothyrotomy include massive swelling or obesity with loss of landmarks. 34 Age younger than 10 to 12 years is a contraindication because anatomical considerations make surgical cricothyrotomy extremely difficult, children are prone to laryngeal trauma, and they have a higher incidence of postoperative complications from surgical cricothyrotomy than adults. 36 Therefore, children should undergo needle cricothyrotomy if no other airway can be obtained.
Cricothyrotomy Procedures and Equipment
There are numerous variations of cricothyrotomy equipment, including several commercially available sets for needle percutaneous and open surgical procedures. Many of these procedures are hospital-based techniques and are beyond the scope of this review. Some of these procedures have more tools, and therefore additional steps to complete the procedure, and are less practical as described for use in austere environments. Table 1 provides a listing of 12 surgical cricothyrotomy procedures. 13 ,20,32,37–45
Cricothyrotomy procedures
ET, endotracheal.
Initial surgical cricothyrotomy incisions are either vertical (longitudinal) or horizontal (transverse) based on the selected procedures. Technique is a provider preference based on training, anatomical knowledge, laryngeal trauma, and whether there is a loss of anatomical landmarks. The vertical midline incision is now the preferred surgical cricothyrotomy technique on the battlefield, as loss of anatomical landmarks is common. 20
Wang et al 46 found that reports comparing the speed of different techniques were inconclusive. However, when 12 studies were compared, most traditional surgical cricothyrotomy procedures or other surgical variations were faster than, or as fast as, percutaneous techniques, with the average speed 83 ± 44 seconds (range, 28–149 seconds). 47 –58 These studies were not standardized for provider level, airway experience, procedure, or model. We recommend the 3-step procedure as fast, simple, and easy to perform with basic tools even in remote or austere locations.
Improvised Cricothyrotomy
The equipment in various commercial cricothyrotomy kits can be complicated. and providers may prefer more familiar basic tools. 59 Moreover, a wilderness provider is unlikely to have a “cricothyrotomy kit” and more likely to have assembled his or her own multipurpose equipment. Austere environments necessitate ingenuity and creativity to overcome lack of resources or environmental challenges. 60 Adams and Whitlock 61 emphasize use of equipment that optimizes “ergonomics, simplicity, and reliability,” especially in a combat scenario; this equipment may include items not traditionally used for medical procedures. The Committee on Tactical Combat Casualty Care published a list of preferred cricothyrotomy kit features that may be applicable to providers in other austere environments. 14 Small commercial kits (North American Rescue, Tactical Medical Solutions, and H&H Associates) targeted for military and law enforcement personnel are ideal for any austere environment medical provider.
Published cases indicate that many everyday objects can be used for cricothyrotomy. In the words of Dr Nancy Shannon, “a field expedient tube or object may be utilized.” 37 Reported objects include a sport bottle drinking-straw, 61 a modified nasal speculum, 62 a cutoff syringe barrel (3 mL with 7.0 ET tube adapter), intravenous tubing chamber with spike, 63 ET tubes, 32 ,33,37 ballpoint pens, 64 specialized keychains, 65 and others. The Lifestat keychain (French Pocket Airway, Inc, New Orleans, LA) is a specially designed device with built-in trochar, cannula, and adapter pieces for field-expedient cricothyrotomy. This device can be used for pediatric patients as well as adults. In a small retrospective review, it was placed correctly in 17 of 17 patients with no complications. 65
Prolonged use of ballpoint pens may be used successfully for cricothyrotomy tube device if the lumen is greater than 4 mm. 64 Owens et al 64 tested 8 commonly available pens for airway resistance at various airflow rates and speed of disassembly for fashioning an airway tube. The 2 pens ultimately deemed acceptable were the Baron retractable ballpoint pen and the Bic Soft Feel Jumbo. Although urban legend and the aforementioned study indicate that one can perform a cricothyrotomy with a ballpoint pen barrel, there have not been any published case reports to date. Also commercially available are convenient penlike devices specifically designed for cricothyrotomy, Wadhwa Emergency Airway Device (Cook Critical Care, Bloomington, IN). Similarly, recent work by Michalek-Sauberer et al 66 examined different cricothyrotomy devices in a controlled lung model for compliance and resistance of airway device diameters. They reported that a spike and drip chamber device for an improvised airway, previously documented by Huber, 63 does not provide effective ventilation. The device's inner diameter needs to be at least 4 mm, confirming the results of Owens et al. 64 They also found that cuffed cricothyrotomy devices, which prevent air leakage around the tube, are essential for best ventilation. 66
Because airflow resistance is inversely proportional to the lumen's radius taken to the fourth power (Poiseuille's law [R = 8ηl/πr4], where R is resistance, l is length, η is viscosity, and r is radius), a decreasing lumen size decreases ventilation exponentially. Thus, smaller items can only be used as a bridge to definitive airway management, as they provide oxygenation but not ventilation. The intravenous tubing chamber with spike, described above, has been documented in a case series with good results when combined with a jet ventilator. 63 A person can breath spontaneously through a small catheter after percutaneous needle cricothyrotomy.67,68 Once the major goal of opening the airway is accomplished, many different tools can be used to provide varying degrees of oxygenation and ventilation. 59 On the other hand, Scrase and Woollard 35 documented the inadequacy of needle cricothyrotomy with low-pressure ventilation as would typically be the case in wilderness situations. However, needle cricothyrotomy can be quickly and easily converted to surgical cricothyrotomy. In one series, 11 of 17 needle cricothyrotomies required conversion to surgical cricothyrotomies. 68
Several authors have devised cricothyrotomy techniques to overcome massive swelling, morbid obesity, or complete darkness. In the “blind technique,” 37 the provider makes a vertical midline incision and dissects until the landmarks are palpable, and then makes a horizontal stab through the cricothyroid membrane. A bent 14-gauge needle tip can be used as a cricothyrotomy hook, and a hemostat can be used to dilate the membrane opening. Other techniques for rapid, reliable placement in the setting of obscured anatomy are insertion of a flexible ET tube stylet into the trachea with a tube “railroaded” over it, or use of a cutdown 6.0-mm ET tube with a preloaded stylet secured just beyond the tip, which is inserted as a unit before removing the stylet. Morris et al 33 and others 50 ,69–71 have described the bougie as a similar cricothyrotomy introducer with good result. The bougie may even assist cricothyrotomy when wearing night-vision goggles, although close range visual acuity with night-vision goggles poses challenges on its own. 32 A wilderness provider may be able to improvise one of these techniques with the tools on hand.
Success Rates
In the civilian prehospital environment, surgical cricothyrotomy is relatively fast, safe, and highly successful, 2 ,5,6 especially considering that it is infrequently performed, invasive, emergent, and often performed in suboptimal conditions with very basic equipment. Tables 2a and 2b present cricothyrotomy success rates for 13 EMS flight crews studies 31 ,72–83 and 11 EMS ground studies, 2 ,4,6–8,12,33,68,84–86 respectively.
Success rates for flight emergency medical service cricothyrotomy studies
Success rates for field emergency medical service cricothyrotomy studies
ALS, advanced life support; CRNA, Certified Registered Nurse Anesthetist; IDF, Israel Defense Forces; PA, physician assistant; TEMS, Tactical Emergency Medical Support.
A meta-analysis by Hubble et al 87 indicates a 90.5% success rate in a prehospital cricothyrotomy series of 485 patients across 18 studies. Ground and aeromedical teams performed similarly (90.8% and 90.9% success rates, respectively). Interestingly, needle cricothyrotomy in prehospital studies had a much lower pooled success rate than surgical cricothyrotomy (65.8%; range, 25.0%–76.9% vs. 90.5%; range, 83.3%–97.1%) despite being less invasive. 87
Walls 5 relates 2 major problems when performing an emergent cricothyrotomy that can affect success rates: 1) the stress of the operator owing to the life-threatening nature of the situation; and 2) anatomical distortions caused by injury. The definition of a successful cricothyrotomy is a tube that transverses the cricothyroid membrane with the distal end in the trachea. Positive patient outcome is not a requirement for procedural success, as a large number of these patients will die despite prompt, proper airway control.
Mabry and Frankfurt 29 reported the first retrospective analysis of the Joint Theater Trauma Registry, which revealed 72 cricothyrotomies performed on the battlefield (n = 45) or at battalion aid stations (n = 27) during a 22-month period during Operation Enduring Freedom (Afghanistan) and Operation Iraqi Freedom (Iraq). They found that prehospital cricothyrotomy by medics (personnel trained to an Emergency Medical Technician-Basic level) was successful in 62% of the cases, although 33% were incorrectly placed. This failure rate is 3- to 5-fold higher compared with civilian prehospital studies (personnel trained to an Emergency Medical Technician-Paramedic level). Additional data revealed a 77% success and 15% failure rates by junior physicians and physician assistants working at battalion aid stations. These authors conclude that additional solutions are needed to master this procedure.
Complications
Complications are reported to occur in 18% of cricothyrotomies. 4 Procedures in the field are more prone to complications than in-hospital procedures owing to inclement weather, poor lighting, inability to maintain a sterile field, positioning of patient and rescuer, tactical environment, and lack of equipment. Bair et al 75 reported complications in 14% and 54% of all hospital and field cricothyrotomies, respectively. In this study, the high rate of field complications could be attributed to attempts taking more than 2 minutes.
Complications can be grouped by immediate vs. delayed and major vs. minor. Emergency care providers are most concerned with immediate complications because they have to be handled straightaway. Notable immediate complications include misplaced incision (leading complication in military and civilian data) with incorrect placement through the thyrohyoid (thyroid) membrane, 13 ,14,26 iatrogenic injury to the thyroid or cricothyroid cartilage when using a cricothyrotomy hook, aspiration of blood or vomitus, tube occlusion with blood,61,88 false passage, retrograde intubation, 89 mainstem intubation, 61 excessive edema, hemorrhage or hematoma formation,63,90 posterior tracheal laceration, inadvertent extubation, and others.
There are several strategies to remedy or mitigate these complications. Thorough anatomical knowledge and use of ultrasound help identify landmarks. If an incision is misplaced, provided it is longitudinal midline, it can be extended superiorly or inferiorly. To avoid causing injury to the vocal cords, use a small cricothyrotomy hook and pull inferiorly on the cricothyroid, or pull superiorly on the larger thyroid cartilage. Both cartilages will fracture if too much force is applied with either a hook or an oversize ET tube. No studies have confirmed the potential problem of tearing the ET tube cuff with a hook.
Hemorrhage can be minimized with a superficial skin incision and blunt dissection to the cricothyroid membrane. A horizontal stab made through the inferior cricothyroid membrane avoids the nearby cricothyroid artery.5,15 If hemorrhage occurs, use direct pressure to stop it. Avert posterior tracheal laceration using extra caution, an angled scalpel position when stabbing the cricothyroid membrane, and a depth no greater than 13 mm. Prevention of ET tube mainstem intubation can be avoided by advancing the tube no farther than loss of sight of the balloon. Maintain manual control of the tube until secured with a girth hitch around the tube at the midpoint of approximately 30 inches of roller gauze. Use the long tails to wrap behind the patient's neck and tie firmly back on the ET tube.
If mainstem intubation has occurred, retract the tube until bilateral chest movement and breath sounds are appreciated, then resecure. To minimize false passage always keep an instrument or finger in the trachea once percutaneous access has been achieved. Watch the tube pass through the tracheal ring. When available, a bougie or stylet introducer can also prevent false passage. The rare retrograde cricothyrotomy has only been reported once, 89 but care should be taken to angle the tube inferiorly on insertion.
If edema renders the standard 2- to 3-inch tracheostomy tube too short to reach the trachea, or dislodges it as swelling increases, an ET tube may be used.33,70 If delayed swelling occurs, swap the tracheostomy tube over a bougie and replace with an ET tube. Use of suction, if available, may reduce the risk of aspiration. A bougie can be used to dislodge clots from ET tubes occluded by blood when suction is not available. 88
Cricothyrotomy Training
Infrequent procedures need frequent training.—S.D. Eyer, MD6(p835)
Elliott et al 13 state one of the main reasons for cricothyrotomy failure is the lack of clinical experience. Therefore, cricothyrotomy requires regular refresher training for skill maintenance. Most cricothyrotomy training uses simulation, self-made trainers, mannequins, cadavers, or animal models. 57 ,91–95 Each training modality has strengths and limitations; a common problem is that low-stress and low- to medium-fidelity cricothyrotomy simulation only prepares providers for the step-by-step procedure, and not the emergent, high-stress application of this skill when needed. Thus, the most effective method of cricothyrotomy training is unknown. Common questions asked are what is the minimum training frequency needed and which training model provides the best skill preparation?
A limited number of quality studies have addressed these questions. Wong et al 96 recommend at least 5 cricothyrotomy attempts or a consistent procedure time of 40 seconds or less. Minimum training of 5 attempts was also reported by Greif et al. 97 Recently, Siu et al 93 reported that despite standardized training, provider age and years from residency were associated with decreased proficiency.
Bennett et al 14 conducted a bottom-up review of surgical cricothyrotomy training as part of a tactical combat casualty care 4-day course. This study was initiated based on battlefield lessons learned, which indicated a significant 26% overall failure rate across all providers attempting emergent cricothyrotomy. 29 This study indicated 5 deficiencies: 1) limited gross anatomy review; 2) lack of “hands-on” human laryngeal anatomy practice; 3) nonstandardized cricothyrotomy equipment and procedures; 4) inferior mannequins for laryngeal anatomy; and 5) lack of refresher training frequency. These authors 14 also provided novel step-by-step cricothyrotomy training recommendations.
Limitations to the use of mannequin cricothyrotomy trainers include synthetic tissue texture; poorly developed laryngeal anatomy, particularly incorrect dimensions; and no replication of complications. For these reasons, as well as the lack of cricothyrotomy skill application in the clinical setting, many have used live-tissue animal models. 57 ,95,98–101 Live-tissue animal models provide real-time and realistic feedback including hypoxia, irregular respirations, and bleeding. Alternatively, the use of fresh or preserved human cadaver models more accurately reflects correct airway anatomy and some tissue characteristics. Nonanimal simulation currently does not provide the realism or physiological responses in sufficient fidelity to replace live-tissue training. The use of live-tissue training for developing enhanced cognitive fitness and psychological resilience from exposure to traumatic events is also very important.
A follow-up question about cricothyrotomy training is how to maintain a skill that is rarely used. 102 Wong et al 96 found that a 1-month refresher interval was superior to a 3-month interval for skill maintenance. 103 A panel discussion conveyed a strong consensus that surgical cricothyrotomy providers should have refresher training every 6 months at the minimum. 6 More recently, Kudavilli et al 102 evaluated cricothyrotomy skills evaluation at baseline, 6 to 8 weeks, and 6 to 8 months and concluded that simulation-based cricothyrotomy training on a medium-fidelity simulator enhanced performance at weeks 6 to 8, but not beyond, and recommended refresher training at least every 6 months.
Recommendations
Table 3 provides recommendations and supporting justification for surgical cricothyrotomy principles, procedures, and training in the austere environment. The recommended fast and simple cricothyrotomy 3-step procedure algorithm is outlined in Figure 2, and is developed based on the studies by MacIntyre et al, 32 DiGiacomo et al, 39 and others. 50 ,69–71 Rigorous attention to these recommendations will optimize success and minimize complications in austere environments.
Recommendations for surgical cricothyrotomy principles, procedures, and training
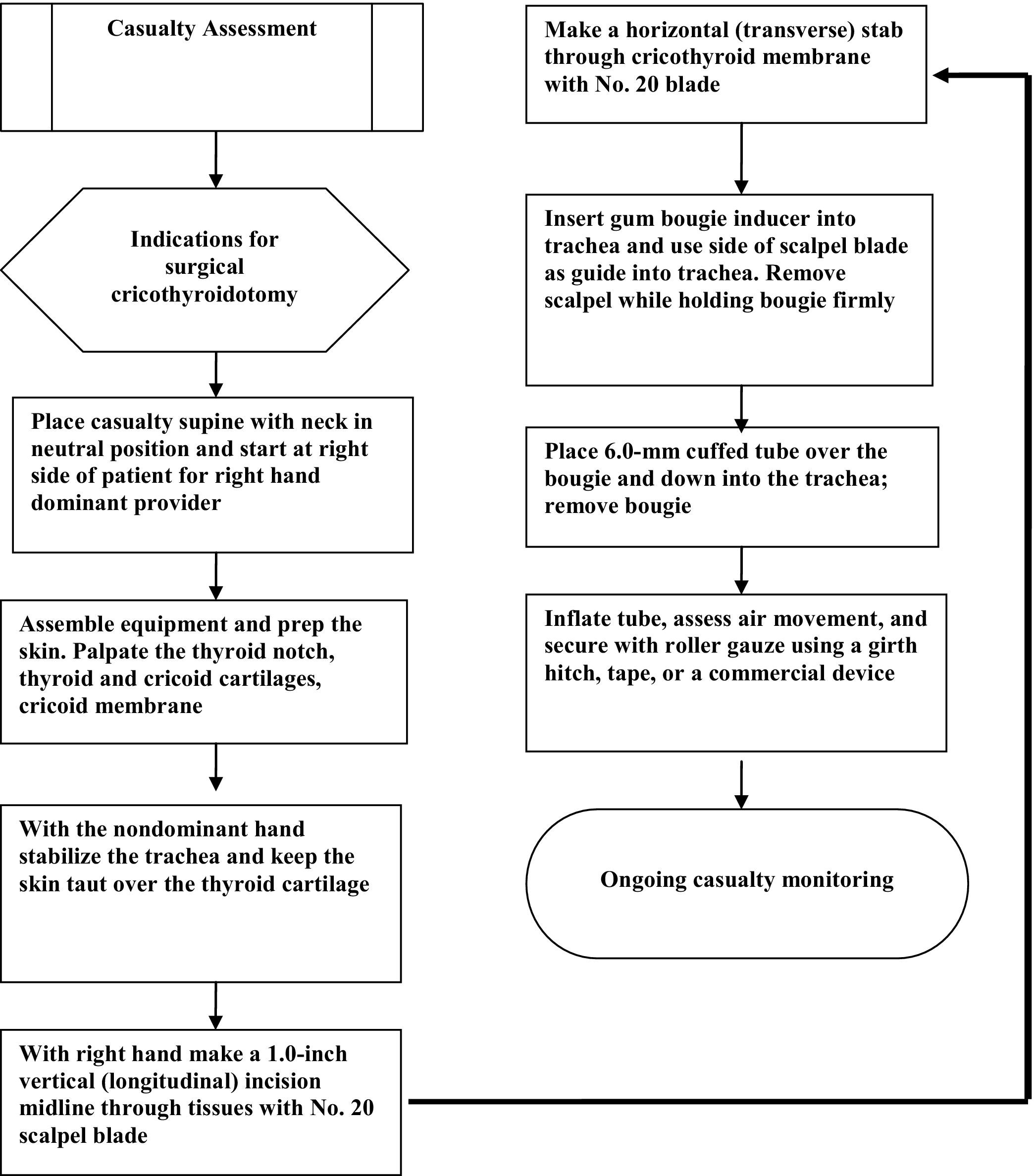
Recommended 3-step cricothyrotomy algorithm.
Conclusions
Cricothyrotomy in the austere environment may seem like a formidable challenge and it is; yet, it can be achieved with the right preparation. Emergency medical providers must have a strategy ready for use at a moment's notice when faced with a critical patient who has an unsecured airway and meets the indications or physiologic triggers for cricothyrotomy. A fast and simple 3-step surgical cricothyrotomy procedure with multipurpose tools is appropriate in the austere environment for trained medical providers with sound anatomical knowledge (Table 1, Figure 2). Training should progress from laboratory-based skills practice to a more stressful, high-fidelity scenario-based trainer with semiannual refresher training. A combination of anatomical knowledge, familiarity with procedures and equipment, and the confidence to make the decision to perform cricothyrotomy with troubleshooting and improvisation as necessary will improve provider comfort, optimize cricothyrotomy success, and ultimately save lives.
Footnotes
Disclaimer: The views expressed in this article are those of the author(s) and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense or the United States Government.
I am a military service member. This work was prepared as part of my official duties. Title 17 U.S.C. 105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a United States Government work as a work prepared by a military service member or employee of the United States Government as part of that person's official duties.