
To the Editor
We suspect most of your readers are familiar with the EpiPen. Its black needle tip and gray safety cap have been standard for almost 40 years. In the fall of 2010, the EpiPen colors were changed: the black needle end became orange and the gray safety cap became blue. Other changes were made to the EpiPen autoinjector that might not be readily apparent to all providers or users, especially in the excitement of a life-threatening anaphylactic reaction.
Figure 1 shows a number of autoinjectors. One of them is not epinephrine, but might find its way into your hands or your patient's, and would allow a patient in anaphylaxis to die. There is no warning that it is not epinephrine despite its nearly identical appearance to traditional epinephrine autoinjectors. The drug name administered by the nonepinephrine autoinjector is Alsuma, an antimigraine medication whose autoinjector version was approved by the Food and Drug Administration in 2010. The Alsuma autoinjector has colors identical to the new EpiPen also released in 2010 and a casing identical to the old EpiPen (Figure 2), even down to the design of the caps (Figure 3). Nine-year-old EpiPens still have 63% efficacy, 1 and many consumers and physicians are aware of this, so it is likely we will have this problem of confusion with both old and new EpiPens for several more years even as old EpiPens expire.

Different autoinjectors: 4 of these 5 autoinjectors are intended for anaphylaxis; 1 is an autoinjector intended for migraine treatment.

From left to right: new post-2010 EpiPen autoinjector; Alsuma autoinjector first introduced in 2010; pre-2010 EpiPen autoinjector.

Alsuma (left) and EpiPen (right) safety caps have identical construction and markings. The blue coloring of the Alsuma safety cap is identical to the blue used in the new EpiPen (see Figure 2).
This problem is especially pressing in the wilderness setting. A recent expert panel studying the management of anaphylaxis in the wilderness noted that “even the simple autoinjector is not so simple to use when a patient [in the wilderness] is in extremis.” 2 In addition, the Wilderness Medical Society has released a formal position statement that, in situations when access to standard medical care will be delayed owing to weather or geography, that “properly trained, non-medical professionals … be trained to appropriately administer epinephrine for the treatment of anaphylaxis.” 2 The unique recommendation that nonmedical professionals independently diagnose and treat a medical condition with a prescription drug increases the importance that the drug be appropriately labeled and uniquely identifiable. It also underscores the importance that the wilderness medicine community be aware of possible look-alikes, to ensure that “proper training” of nonmedical professionals includes awareness of this situation.
We urge that all Alsuma autoinjectors be labeled “NOT EPI” in red and black letters on the white container (Figure 4). There are other epinephrine autoinjectors in a white container. This warning and request for relabeling is being sent to the Food and Drug Administration, who we hope will require Alsuma to apply strong adhesive labels to both device and case stating NOT EPI until both can be redesigned to more clearly differentiate this product from epinephrine autoinjectors.
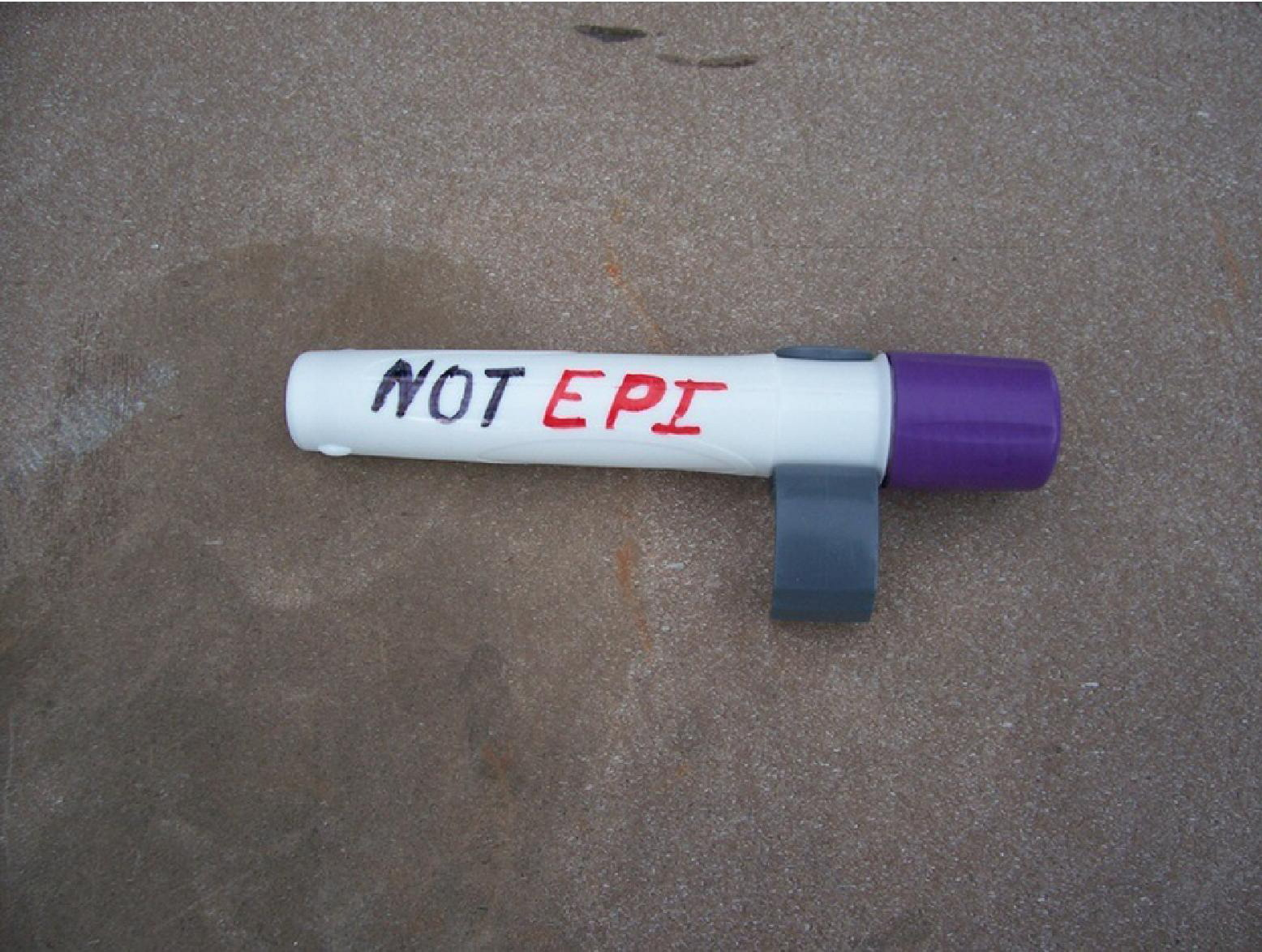
Proposed markings for Alsuma autoinjector.