
Abstract
A 28-year-old nursing student working in Juba, South Sudan, suddenly developed a rash over her mid-right clavicle. Beginning as a 10-cm-diameter erythematous patch with an irregular border, within 24 hours it had developed an increasingly gray, necrotic center, appearing similar to a burn. The patient was seen by 2 local physicians without a diagnosis being made. Ultimately, it was diagnosed as being caused by the toxic hemolymph, pederin, from the Nairobi fly (Paederus). The rash usually affects body parts not covered by clothing; healing time ranges from 7 to 28 days, usually with permanent skin discoloration. Preventive measures include typical antivector precautions, including bed nets, long-sleeve clothing, and avoiding fluorescent lights. If the beetles are found on the skin, brushing them off, rather than crushing them, avoids producing dermatitis. Treatment includes rapidly washing the affected area, applying cold, wet compresses, and possibly treating with antibiotics, steroids, and antihistamines.
Case Report
A 28-year-old nursing student working in Juba, South Sudan, suddenly developed a rash over her mid-right clavicle. Beginning as a 10-cm-diameter erythematous patch with an irregular border, within 24 hours it had developed an increasingly gray, necrotic center, appearing similar to a burn. The woman had no significant past medical history or allergies and was unaware of any insect contact within the 48 hours before the lesion appeared. She did have fluorescent lights in the compound where she resided.
During the first 24 hours after noticing the lesion, it produced only mild discomfort. During the subsequent 48 hours, the pain increased significantly. A large central vesicle developed, accompanied by smaller vesicles scattered over the patch and along its circumference. Satellite patches, with progression similar to that of the original site, appeared on her hand where she had touched the original lesions and on her chest and arm where she had subsequently touched those areas. The patient's spouse developed the same type of rash on his posterior hand where he had made contact with the patient's rash.
The patient was seen by 2 local physicians. The first physician, seen on day 3, told the patient that her lesion was not from a Nairobi fly (Paederus sp) and prescribed cloxacillin (beta-lactam penicillin effective against some Staphylococcus spp). A second physician, seen on day 4, claimed he “had seen this lesion before” and dispensed fusidic acid (a topical antibiotic effective against gram-positive organisms, particularly Staphylococcus spp) and flucloxacillin (similar to cloxacillin). Neither suggested cleansing or covering the lesions or warned of possible contact transmission. Several pharmacists suggested debriding the necrotic tissue, or applying lemon juice, steroid cream, or triple antibiotic ointment to the lesion.
Within 24 hours of using the fusidic acid and taking flucloxacillin, the pain increased and she developed more pustules. Forty-eight hours after starting treatment, the vesicles and pustules began to decrease in size, and the pain began to subside. Subsequently she was told that this was a classic Nairobi fly rash and presentation. She then discontinued all medications; after 8 days, the lesions dried and the epidermal and dermal skin peeled. The residual scarring and discoloration is similar to a healed burn.
Discussion
Cause/Prevalence
“Nairobi fly” describes 2 East African beetle species, Paederus crebinpunctatus and Paederus sabaeus. Both cause an acute, painful toxic epidermolysis when the female beetle is crushed on similar skin. Also known as “Kenya fly dermatitis” and “Nairobi eye” (with ocular manifestations) in East Africa, the skin lesions caused by local Paederus beetle species are referred to as the Manipal bug or Nitte police (India), el podo (South America), or other local names, such as spider-lick and whiplash dermatitis. “Blister beetle dermatitis,” sometimes used for Paederus dermatitis, is more properly dermatitis caused by cantharidin from blister beetles. Western medicine did not recognize the toxic effects of Paederus until the 20th century, although Chinese clinicians have recognized it for more than a millennium.
Paederus or rove beetles are prevalent in most warm tropical climates and in many temperate climates around the world, with at least 20 of the more than 600 species having been associated with dermatitis, even though they neither bite nor sting. The East African Paederus do not fly, despite their local name, although some other species do.1,2
Adult Paederus are vividly colored compared with other Staphylinidae, considered a type of aposematism (warning coloration). 3 They are small (7–10 mm long and 0.5 mm wide) with soft, dark-orange bodies and black heads, tips of the abdomen, and, if they have them, front wings (elytra) (Figures 1 and 2). 1 ,4,5

“Nairobi fly” Paederus in Juba, South Sudan.

Paederus size comparison.
Many species prefer to lay their eggs and develop in the moist, decaying vegetation of marshes, agricultural fields, and areas surrounding fresh water. At night, light towers and other bright light sources can attract the flying species of adult beetles from habitats that are several miles away. Paederus beetles sometimes fly in large numbers on warm nights, particularly after heavy rains or floods.1,5 Paederus adults are also active in daylight, with some species able to run on water. 2 The population increases rapidly at the end of the local rainy season and then rapidly diminishes with the onset of dry weather.
Pederin
Crushing the Paederus beetle releases the unique amide, pederin (also known as pederine), a hemolymph vesicant toxin. Pederin has two tetrahydropyran rings and the chemical formulation C25H45NO9 (Figures 3 and 4).
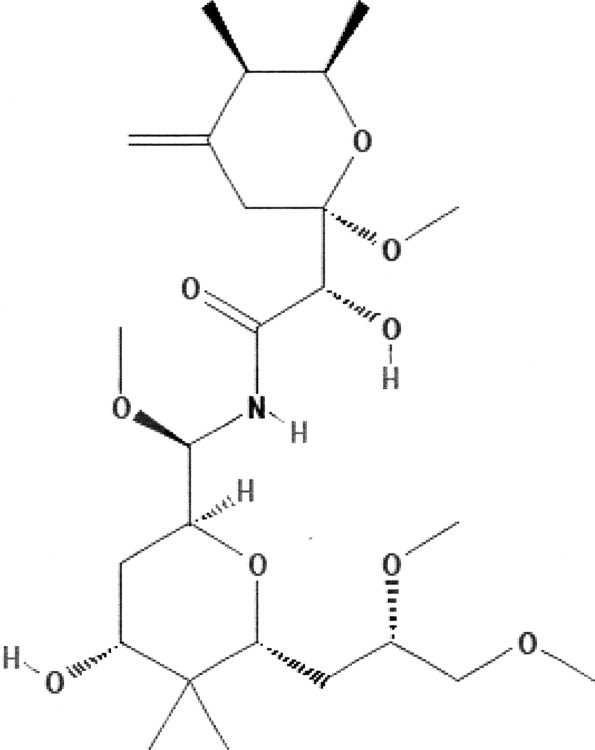
Pederin chemical structure. Two-dimensional diagram.
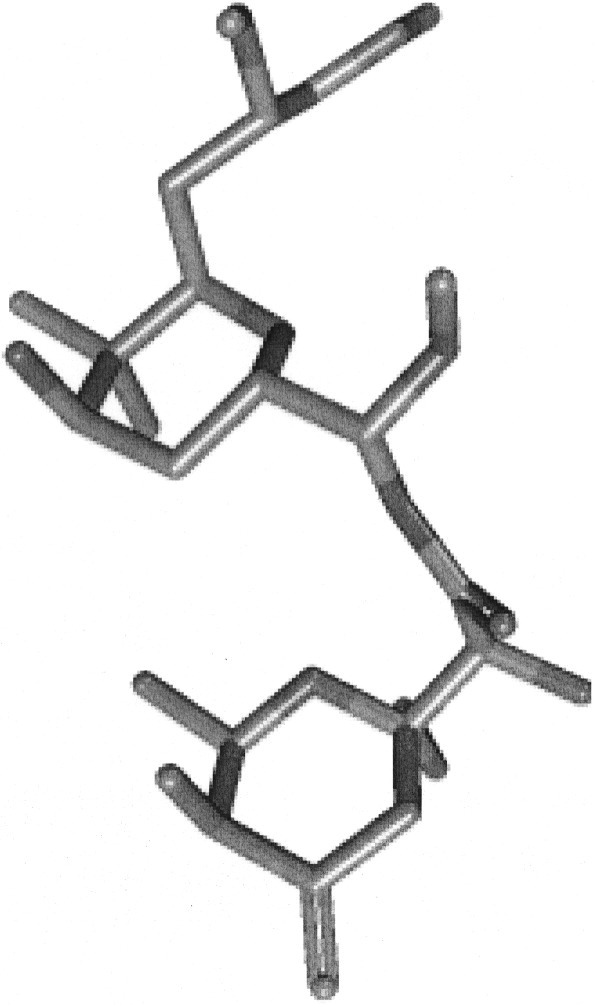
Pederin chemical structure. Three-dimensional diagram.
Pederin is the most complex nonproteinaceous insect secretion. The beetles, however, do not manufacture it. Rather, an endosymbiont (organism living within the body or cells of another organism) bacteria, probably a Pseudomonas aeruginosa species, produces it.2,6 In all Paederus species, up to 90% of the females contain high levels of pederin (about 1–1.5 μg of pederin per specimen), 3 and only these positive females transfer this trait to their female offspring.6,7 Larvae and males only store pederin acquired maternally (ie, through eggs) or by ingestion.
Pederin is highly cytotoxic, and as little as 1 ng/mL blocks the synthesis of DNA and of eukaryotic cell proteins in ribosomes (60S subunit). 2 ,3,6 For these reasons, it has garnered interest as a potential anticancer treatment. Thirty-four pederinlike molecules have been described, with nearly all 8 isolated from marine sponges. 6
Typical Presentation
Releasing pederin by crushing a Paederus beetle against the skin may cause little to no immediate effect, but usually results in itching, burning, erythema, and oozing 12 to 36 hours later. 9 As in this case, the lesion's cause may not be recognized, because dermatitis appears only several hours after contact with Paederus hemolymph. 10 The burning sensation is more pronounced than pruritus. Patients rarely complain of pain, although in the case presented, it was a prominent feature. In some regions, up to 20% of patients are totally asymptomatic, presenting only with the skin lesions.
Skin lesions vary by the type of Paederus beetle—and the potency of its toxin. Regional variations go from severe lesions to relatively benign rashes. Skin lesions are usually linear, vesicobullous, or pustular on an erythematous base. Some may present with large bullae. In some regions (eg, southern India), the lesions may be linear, geographic, erythematous plaques with a “burnt” appearance. 11 Some pederin toxins produce lesions with numerous micropustules interspersed with the primary vesicular lesions. Marked epidermal necrosis or diffuse desquamation may also occur. Systemic immunoglobulin E-mediated hypersensitivity reactions are exceptionally rare. 9
The most commonly affected body parts are areas usually not covered by clothing, especially the face (including periorbital) and neck, followed by the shoulders, arms, and area around the waist. 9 Patients may not seek medical treatment for several days after lesions appear. Most patients have more than 1 lesion, and some have “kissing lesions” (lesions on opposing skin surfaces)—which occurred in the patient presented. In many cases, another family member is also affected. 12 This patient's husband developed lesions on his hand where he touched the initial blisters. How often this secondary transmission of pederin occurs is unclear.
In Africa, lesions often appear in the periorbital area, with associated conjunctivitis known as “Nairobi eye.” Although mucosal surfaces are relatively less affected by pederin than the skin, introducing it into the eye can cause intense pain and temporary blindness. 9
Histopathologic examination of pederin lesions demonstrates acute irritant dermatitis in the upper epidermis. The basal and suprabasal layers show mitotic figures and apoptotic changes, such as chromatin condensation and DNA fragmentation. 13
Healing
The rash develops into blisterlike lesions that dry out within 1 week, and become crusted and scaly. Healing time ranges from 7 to 28 days, with most healing in 14 to 21 days. In some regions, nearly all patients heal with residual skin discoloration (about 80% hypopigmentation, about 20% hyperpigmentation), whereas in others it is rare. 14 Scarring rarely occurs.5,9
Preventive Measures
Limiting Paederus contact is the most effective preventive measure to avoid pederin dermatitis. Especially during the rainy season, when the beetle is active, avoid working or resting under bright lights, especially fluorescent and neon lights and insect electrocution devices (eg, Bug Zappers) that use ultraviolet light to attract insects. 4 ,11,12,15 This is especially important in regions with flying Paederus beetles. Wearing long-sleeve shirts and hats at night (also a preventive measure against other insect vectors) diminishes the likelihood of skin contact with Paederus beetles. Window screens help to prevent Paederus beetles and other insects from traveling toward indoor light sources. Remove any decaying vegetation around buildings and work areas to eliminate potential harborage for the beetles and their larvae. 16
If a Paederus beetle settles on a person's clothing or skin, the person should gently shake or brush it off with something other than his or her hands.2,15
To check for the presence of Paederus beetles as a public health measure, use mosquito light traps, sticky traps, glue boards, or shallow containers filled with water and a few drops of dishwashing detergent set out at night beneath bright light sources to trap adult beetles. Pederin is known to be soluble in alcohol, so be careful when handling alcohol that has been used to preserve Paederus beetle specimens. 16
Treatment
If a Paederus beetle is accidentally crushed against the skin, immediately wash the affected area with soap and water. Pederin slowly penetrates the skin. Washing shortly after exposure will remove much of the toxin before it has time to harm the skin. The skin reaction to pederin is delayed and may take between 12 and 36 hours to occur after the initial exposure. If lesions appear, initial treatment may include cold, wet compresses, followed by the application of calamine lotions or topical corticosteroids. 15
In a study of 50 adult patients with a definite history of contact with the Paederus beetle, 14 of the more severe cases (diffuse desquamation or marked epidermal necrosis) were treated with oral prednisolone (30 mg once daily for 7 days) or intralesional triamcinolone acetonide (diluted to 10 mg/mL). Half of the remaining 36 patients received twice-daily topical diflucortolone valerate (0.001%), along with once-daily oral cetirizine hydrochloride (10 mg); the other half also received twice-daily ciprofloxacin (500 mg). Healing time ranged from 14 to 28 days, and lesions in all the patients healed with residual dyschromia. Healing time was shorter in the group also receiving ciprofloxacin, which may have been related to a concurrent bacterial infection. 9
Although clinicians in endemic areas may be familiar with the appearance of Paederus lesions, these unusual skin lesions may also appear in those returning from endemic areas, especially from East Africa. Not recognizing this delayed-onset reaction can lead to unnecessary diagnostic and therapeutic interventions, as in this case. 11 An extensive literature exists on Paederus “epidemics,”2,3 and in at least one instance, multiple cases in rural Liberia led to panic—even though local clinicians quickly determined the cause. 17