
Abstract
Background
Rabies, although not preeminent among current infectious diseases, continues to afflict humans with as many as 55,000 deaths annually. The case fatality rate remains the highest among infectious diseases, and medical treatments have proven ineffective.
Objective
This study analyzes the rabies epidemic of 1929 to 1937 in Trinidad from a geographical perspective, using Geographic Information System (GIS) software as an analytical tool.
Setting
A small island developing country at a time when infectious diseases were rampant.
Methods
A review of the literature was undertaken, and data were collected on the occurrence of disease in both animal and humans populations and mapped using GIS software. Several factors identified in the literature were further explored such as land use/land cover, rainfall and magnetic declination.
Results
The bat rabies epidemic of 1923 to 1937 in Trinidad was migratory and seasonal, shifting to new locations along a definite path. The pattern of spread appears to be spatially linked to land use/land cover. The epidemic continues to present many unexplained peculiarities.
Conclusion
Despite the fact that this epidemic occurred almost 7 decades ago, the application of new tools available for public health use can create new knowledge and understanding of events. We showed that the spatial of distribution of the disease followed a distinct pathway possible due to the use of electromagnetic capabilities of bats.
Keywords
Introduction
High mortality rates have been associated with epizootics. Rabies, one of the oldest recognized zoonotic diseases, is caused by ribonucleic acid (RNA) viruses in the family Rhabdoviridae genus Lyssavirus, transmitted through the bite of an infected mammal in which the virus is present in the saliva. 1 –4 However, this is not the only mode of transmission, as rabies can be acquired with infected aerosolized tissue in caves inhabited by rabid bats and in laboratory accidents. 5 –7 Transmission is also possible by handling and skinning of infected carcasses.7,8 Human-to-human transmission other than by corneal transplantation has not been well documented,9,10 although, in 2004, rabies was identified as the cause of death among 4 patients who were recipients of organs and a vascular graft. 11 A potential risk also exists from contact with infected body fluids. 12 The only epidemic of rabies to have occurred on the island of Trinidad was in 1929 to 1937. In that epidemic, bats, for the first time, were identified as the mode of transmission. Bats are a major reservoir for variants of rabies viruses and transmit the disease through biting, which can sometimes go unrecognized. 5 ,13–18 Support for the effectiveness of this mode of transmission is derived from laboratory data with silver-haired bats (Lasionycteris noctivagans) and eastern pipistrelles (Pipistrellus subflavus) that demonstrated a higher likelihood of infection after superficial inoculation into cells of epidermal origin. 19 Infection is primarily of the central nervous system (CNS), leading to an acute progressive encephalomyelitis in which most cases are fatal.
The annual number of deaths worldwide caused by rabies is estimated to be 55,000, mostly in rural areas of Africa and Asia, while the annual estimated cost of rabies is $583.5 million (USD). 20 Although mortality from rabies is considerably less in the New World. Canada, documented 24 human rabies cases since 1924,21,22 emphasizing the global importance of this disease. Trinidad continues to provide a habitat for a wide variety of bats including the vampire bat. While reports exist of bats biting humans, there has been no confirmed human case of rabies in Trinidad since the epidemic of 1929 to 1937.
The historical and social forces that influence disease patterns in populations are critical in understanding the epidemiology of diseases. While the identification of biological processes is crucial, the contribution of other factors such as land use, change affecting vector or host habitats, human interaction with vectors, and climate are also important to identify and have a geographical dimension. Spatial diffusion or the movement of disease through time and space to new locations contributes to the understanding of the social and environmental factors that affect risk and susceptibility. While investigation of the 1929 to 1937 epidemics contributed to the further understanding of the biological processes, no study to date has described the geographical patterns. The aim of this study, therefore, is to use Geographic Information Systems (GIS) software capabilities to identify and add a geographical analysis of the epidemic.
Methods
A review of the literature was undertaken using the Med Carib database and Index Medicus, using the key words rabies, epidemic, and Trinidad. All scientific papers published on the epidemic, as well as extracts from the administrative reports of the Director of Agriculture for the years 1923 to 1948, were reviewed: for example, proceedings of the Agricultural Society of Trinidad and Tobago, the administrative report of the Surgeon General for the period 1925 to 1941, and the Central Board of Health, Hints Series No 3 were also reviewed. Data were collected on the number and location of all animal deaths.
All available human cases were reviewed, and data were collected on age at death, gender, and geographic location. Before mapping case distributions, careful consideration was given to all cases in the database with regard to case definition. The nature of the lesions in the nervous system as described by Knutti, 23 together with Negri bodies and positive animal inoculation, were the methods used to establish the diagnosis of rabies.
Mapping and spatial analysis were conducted using ArcGIS version 9.2. Several layers were superimposed on the distribution map of human rabies deaths. The first layer used represented land use/land cover for the island. Due to the scale of this dataset, 1:150,000, and the diversity of land use/land cover represented at the time, it was difficult to show land use/land cover in its entirety. For these reasons, a generalized version of this map was created. The other dataset used was a generalized rainfall map for Trinidad. Previous studies have demonstrated that bats detect and use the earth's magnetic field as an internal compass to re-orient and find their way back to their roosts. 24 Based on this evidence, the average declination for the period under study was calculated using information provided from the National Geophysical Data Center (NGDC). 25 The NGDC provides a free online service that calculates magnetic declination based on date and time and location on the earth's surface.
Results
The data collected showed that the epidemic really began in 1923 among cattle that were dying suddenly in Debe and Maraval. At that time, the deaths were attributed to the ingestion of oleander leaves. 26 In April of the same year, cattle continued to die, which attracted concern and encouraged further investigation. After a careful inspection to discover any poisonous weeds, particularly the local poisonous plants Brinvilliers (Spigelia anthelmintica) and wild ipecacuanha (Asclepias curassavica) or spraying of the area with insecticides, the cause of death was attributed to sodium chloride poisoning. 27 In the following year (1924), further reports of deaths among cattle in the same location (Maraval) went unrecorded. In July 1925, a disease thought unrelated to the events of the previous years broke out among cattle (young heifers) in St Anns, a suburb north of Port of Spain in which animals were dying of a peculiar disease, the chief signs being excessive salivation, marked constipation, and a staggering gait followed by paralysis. 28 In spite of early interventions by veterinary surgeons, all the animals died.
Preliminary investigations revealed that all the animals afflicted were left outdoors both day and night. Stock in stables in the same environment were unaffected. As a prevention strategy, healthy animals were removed from pasture; however, some of these animals continued to die at varying periods from the time of their removal. It was also noticed that stock previously stabled remained healthy, although they were placed in close contact with those removed from pasture. Postmortem examinations of animals that died conducted by the veterinary surgeon provided a differential diagnosis that included bulbar paralysis, botulism, and Grass tetany. The government pathologist confirmed the disease was botulism after discovering Clostridum boutulinus in some of the dead animals. 29 Towards the end of 1925 and early in 1926 similar reports of cattle dying were reported in Diego Martin 4 miles west of Port of Spain. In 1927, the disease reappeared in Diego Martin, while a few cases were also reported in St James, a town on the western outskirts of Port of Spain, and Laventille, 2 miles east of Port of Spain. In the same year, disease in cattle was also reported in Couva, 28 miles south of Port of Spain. With the exception of a few cases in Diego Martin during the rainy season of 1928, the disease appeared to be waning, when suddenly in August of 1929 there was resurgence in Siparia, 55 miles south of Port of Spain, in which occurred the heaviest losses in livestock yet.
By this time the disease had spread to new areas such as St Joseph to the north and Fyzabad to the southeast. In 1929, 1930, and 1931, the death rate averaged over 1000 animals per year, 90% were cattle, but the deaths of horses, mules, and donkeys, and even goats, sheep, and pigs were recorded. Only 2 of the cases occurred in dogs. At this time a full description of the disease was available, resulting in a diagnosis of ascending myelitis. Postmortem and laboratory findings were forwarded to research workers on botulism in the United States, and they reported that they were convinced the disease was botulism. As a consequence, antitoxin was imported, but its application did not seem to stop the disease. The data were mapped using street address and geocoding, and show both the location of all animal deaths and the direction of spread over time (Figure 1).
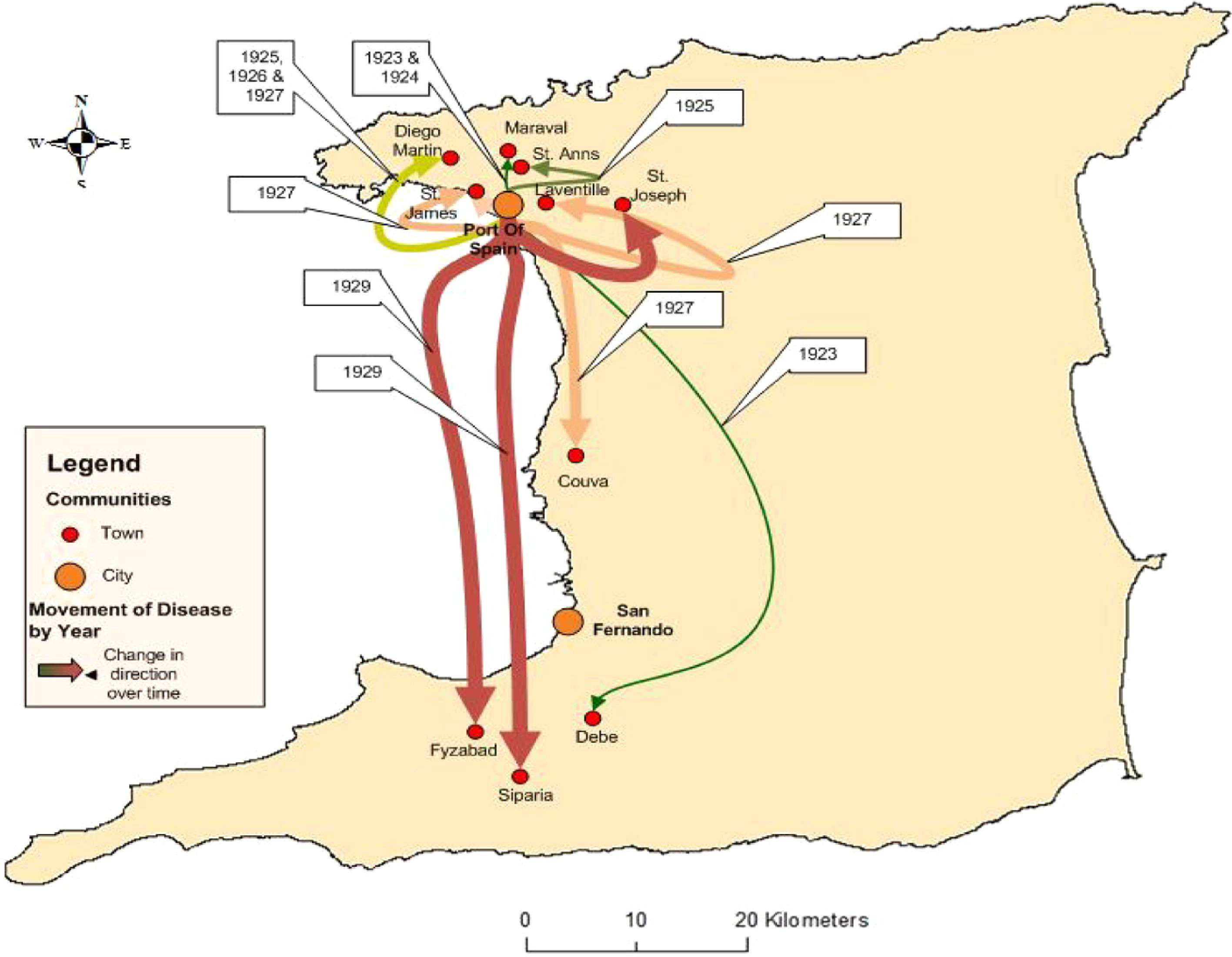
Map identifying communities (cities and towns) in Trinidad with reported animal deaths between 1923 and 1929, and the direction of spread.
The first reported case of the epidemic to occur in humans is presented here in detail. All subsequent cases had remarkably similar presentations. On July 16, 1929 at 10:00
The distribution of human rabies cases in Trinidad, 1929 to 1937
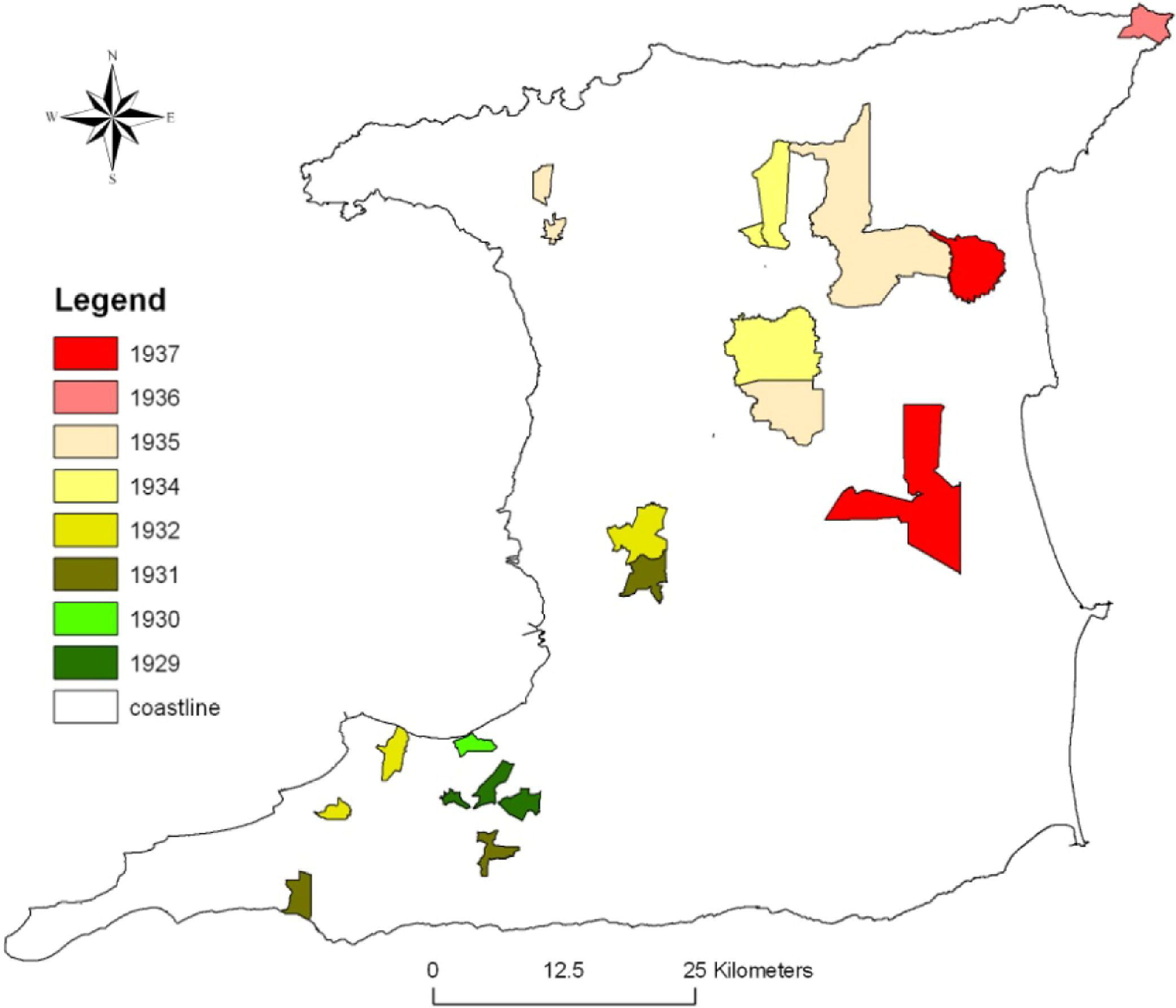
The distribution of human cases from 1929 to 1937 was mapped at the community level using geocoding (Figure 2). Eight maps were produced to show the progression and direction of spread by year starting with the first set of cases in 1929. Each subsequent map is an aggregate of all cases up to that year. A key to the distribution of cases by communities as mapped in Figure 2 is provided in Table 2. The adjacent island of Tobago 22 miles north never recorded any cases.
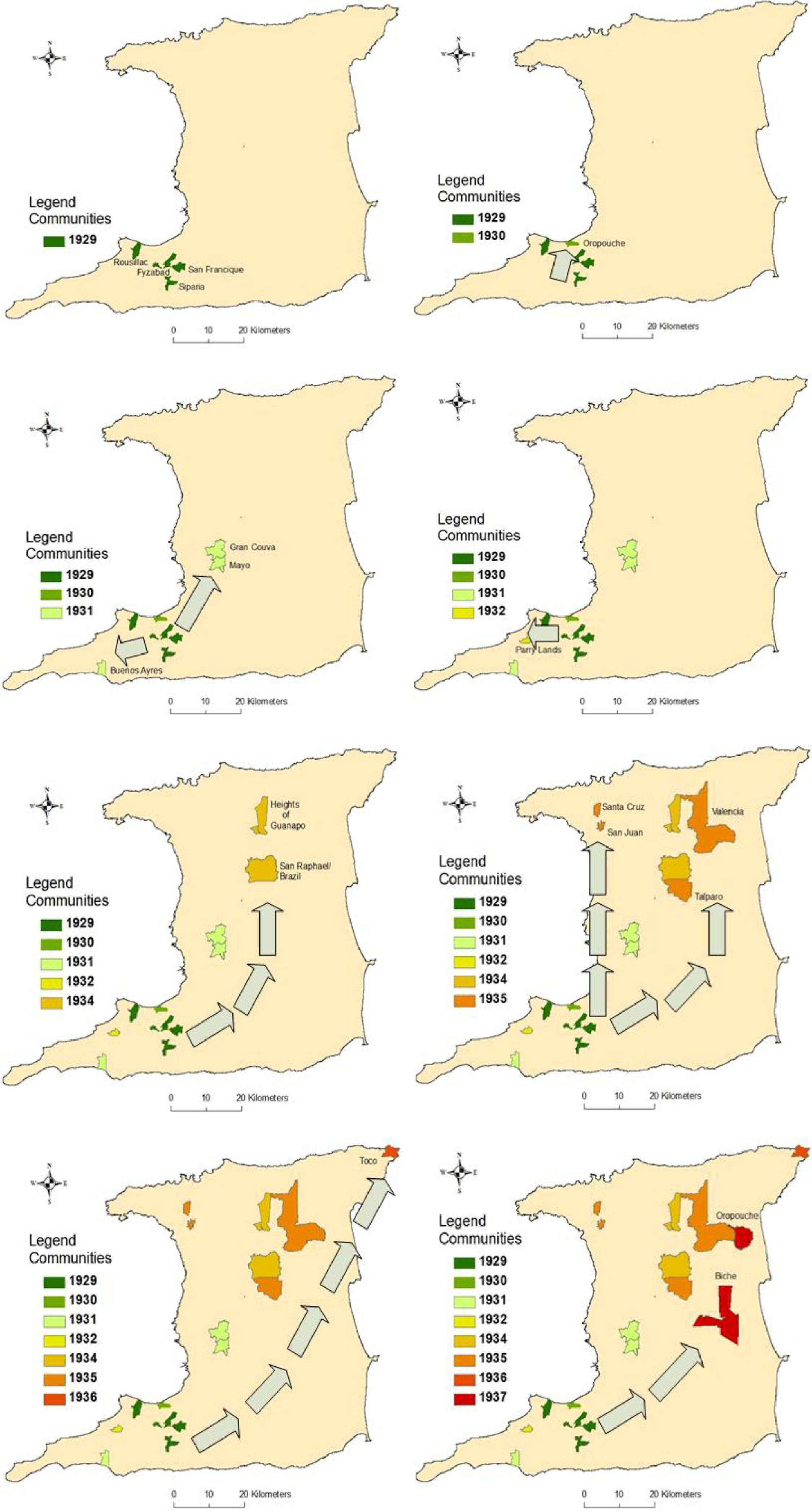
Distribution of human deaths caused by rabies, 1929 to 1937.
The number of human deaths in Trinidad caused by rabies, by location, 1929 to 1937
The mapped human deaths were overlaid on a land use/land cover map showing forest, urban, swamp, rice, cocoa, coffee, banana, and citrus (Figure 3). No reported cases occurred in forested areas, although they provided an ideal habitat for vampire bats. In addition, in urban areas, mainly Port of Spain and San Fernando, no deaths were reported, which may be partly attributed to better housing conditions, annoyances such as noise, and better lighting. On the other hand, there was an almost identical overlap of the occurrence of deaths and cultivation sites for cocoa, coffee, banana, and citrus production. Several factors may explain this finding: (1) cultivation sites provide farm animals for prey by hematophagous bats; (2) cultivation sites lack predators such as snakes, hawks, and carnivorous bats; (3) poor housing allows easy access to humans by bats; and (4) poor housing encourages children and adolescents to spend more time outdoors, increasing their exposure to bats. Over half of the deaths (38) occurred in the age group 0 to 15 years.
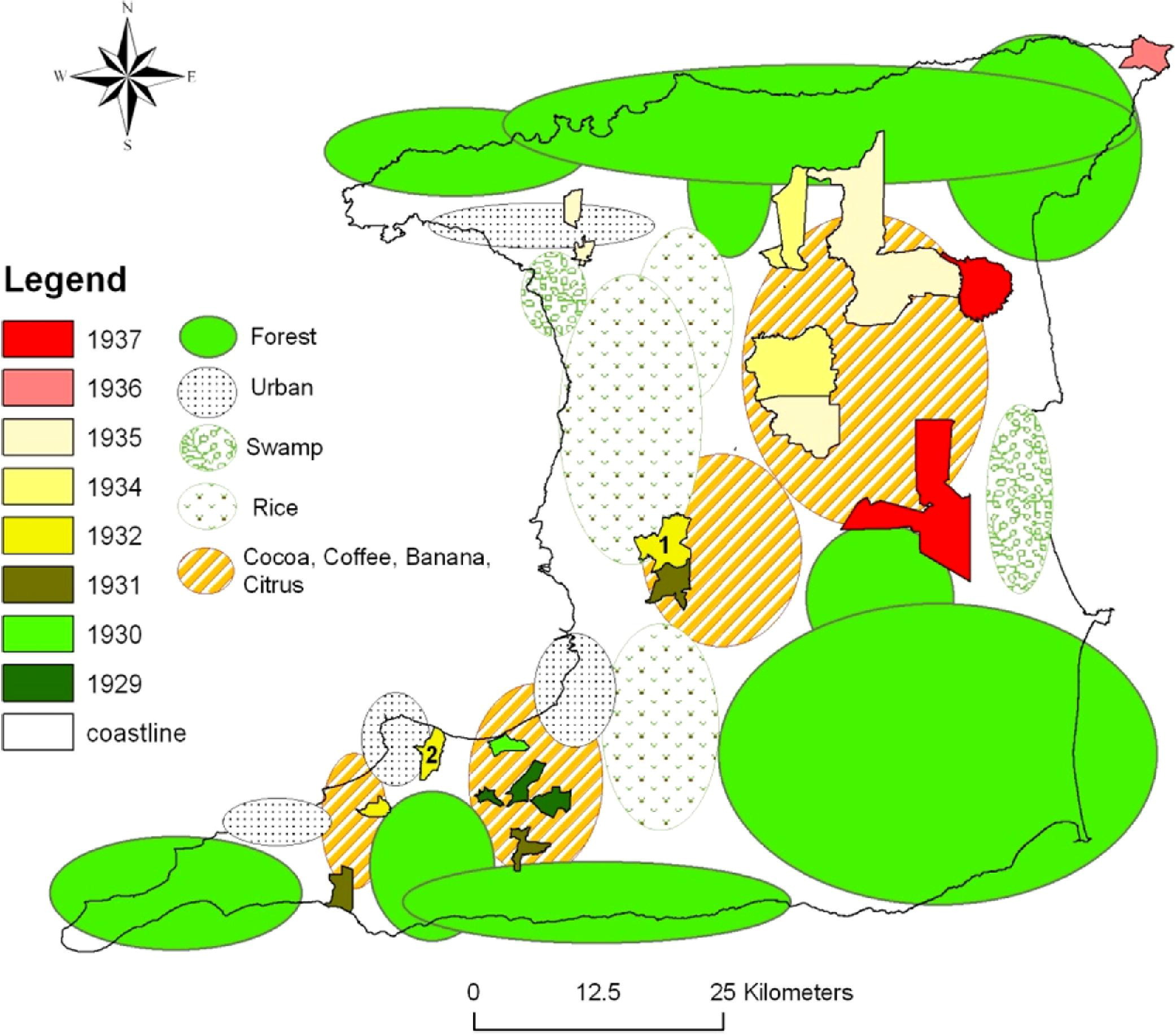
Distributions of human rabies deaths superimposed on to land use/land cover.
Trinidad is situated 11° north of the equator and has 2 seasons, the rainy season during the months of June to November and the dry season from December to May. Average rainfall was overlaid on the distribution of rabies cases (Figure 4); however, no relationships emerged. Although the epidemic lasted 9 years, there were no deaths reported in the months of November or December as shown in Figure 5.
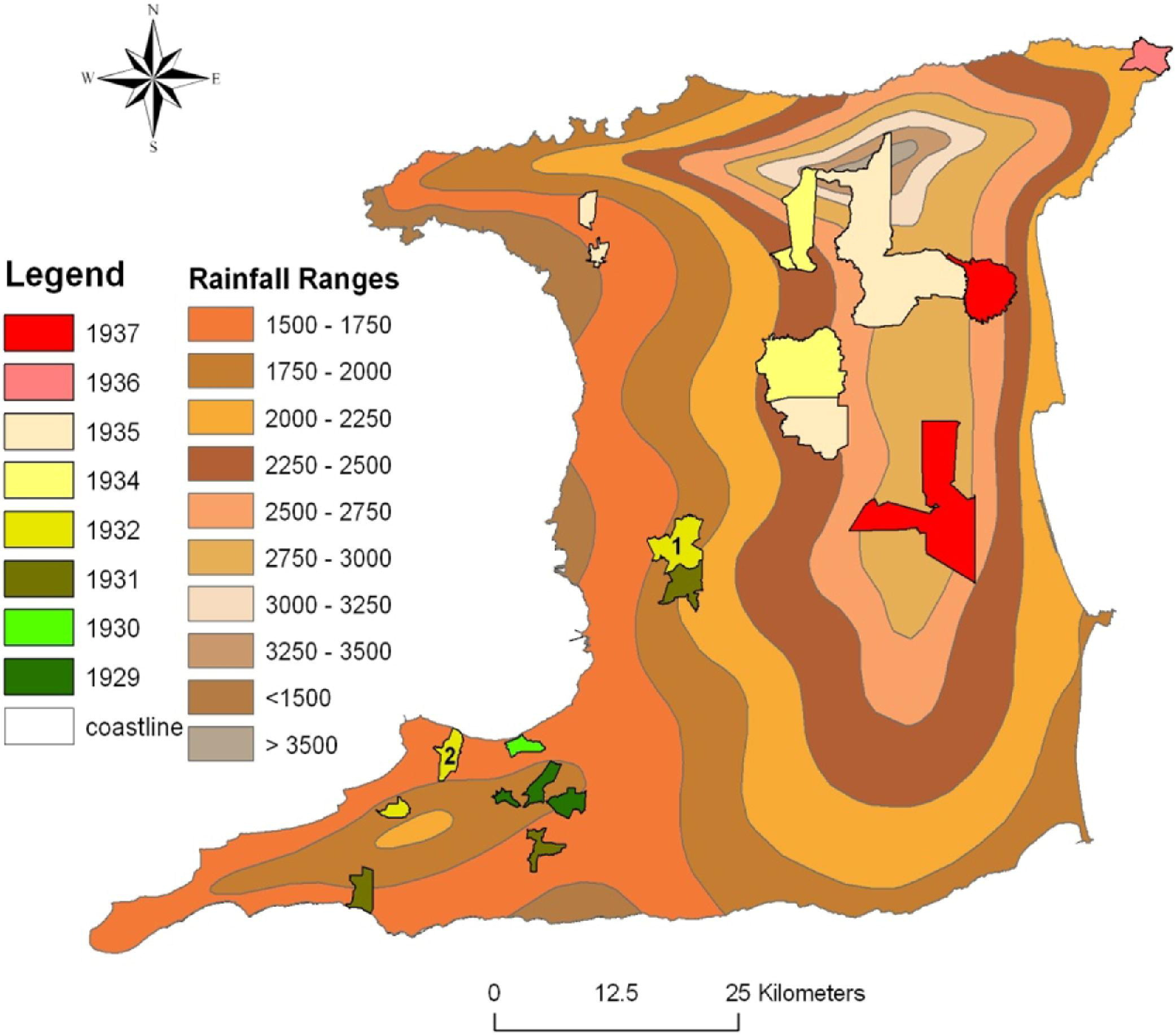
Distribution of human rabies deaths superimposed onto rainfall (inches).
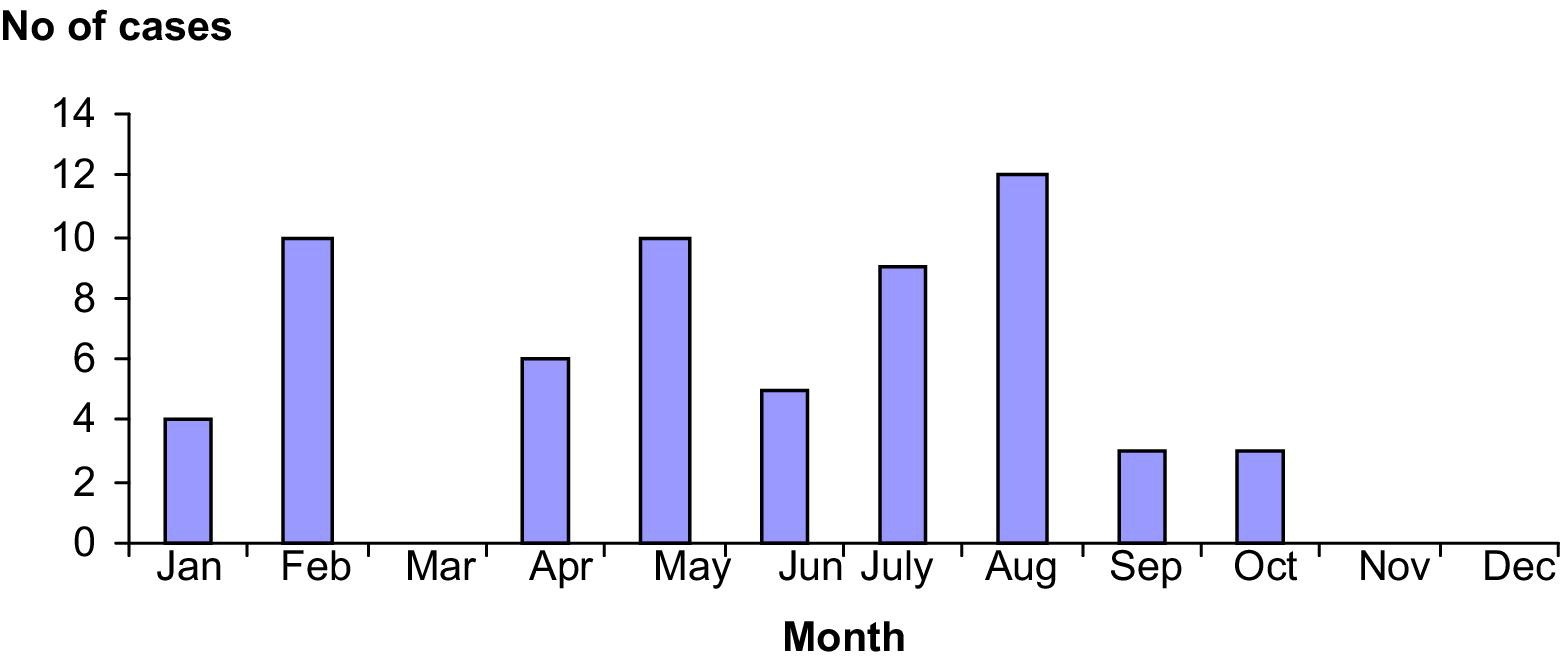
Distribution of cases by month, 1929 to 1937.
Spatial and temporal distribution of cases demonstrated that the epidemic progressed along a northeasterly direction (Figure 6). At the time of the epidemic, magnetic declination was calculated as 5°59' W changing by 0°7' W/year. The forward progression of the epidemic was approximately at right angles to magnetic north. In addition, the mean width of the outbreak was 4.5 km, and the forward annual velocity ranged from 7.5 to 30 km/yr, with a mean of 12.5 km/yr.
Distribution of rabies superimposed onto magnetic north.
Discussion
The major finding of the study was disease among animals followed a hierarchical diffusion pattern; ie, the disease among animals started in an urban setting and spread over time to medium-sized towns, then to smaller towns, mainly along the western half of the island in a southerly direction. On the other hand, disease among humans started in small towns, continued to affect small towns but followed a diagonal pathway to the northeast tip of the island. The use of GIS technology capabilities can now link the epidemic model and the spatial diffusion model to predict the movement of an epidemic and thus identify likely communities at risk. The benefit of these capabilities includes strategic planning, such as the availability of hospital beds, health-care professionals, equipment, and supplies required for an impending outbreak, as well as preventive interventions like immunization of communities at highest risk.
The spatial findings of our study also raise alternative explanations and several questions. Pawan explained the epidemic by suggesting (1) the flight or transit in sloops and other vessels of infected bats from the mainland to Trinidad and (2) the infection of bats in Trinidad by some latent, unrecognized “carrier” of the disease. 33 A more affordable explanation may now lie in the concept of compartmentalization, whereby specific virus variants within a genotype tend to perpetuate among particular hosts in different geographic areas. Such associations may last for decades or longer. 34 This is against the background that the last reported case of rabies in Trinidad prior to the epidemic was in 1912, a 17-year gap. Geographic features, such as mountains and rivers, may create physical barriers to animal movement and promote localized viral evolution in specialized host niches. 35 Also, the emergence of viral variants may occur with extension of the host range. 36 Notwithstanding, movements of infected animals to new unaffected areas have the potential to produce explosive, sustainable outbreaks. 34
Although much travel was conducted between the islands of Trinidad and Tobago, approximately 22 miles across the Caribbean Sea, the epidemic never reached Tobago. The outbreak is further characterized by many peculiarities, the first of which was the apparent disconnect between disease events occurring in animals and humans. The first phase of the outbreak between 1923 and 1931 was characterized predominantly by animal infections, and the first documented human case was not recorded until 1929. The disease occurring in animals and man was not established as the same until September 10, 1931, after much wrangling between veterinarians and physicians. Thus disease events in humans may have occurred but were misdiagnosed, particularly as acute poliomyelitis. However, during the period 1925 to 1928, there were 7, 2, 0, and 0 reported cases of infantile paralysis or acute poliomyelitis, and there were no reported deaths from either acute poliomyelitis or ascending myelitis. Lastly, several questions remain unanswered such as why did the pattern of human disease occur in only one direction without recurring in previously infected areas. It is unlikely that all rabies infected bats in a particular area would have succumbed as Pawan himself showed survival after inoculation with infected brain extract. 33 This raises the question, does survival then alter behavior or does the immunologic response confer incapability to further transmission? It appears from the data that the epidemic ended at the northeast coast of Trinidad, as all 15 cases that occurred in 1937 occurred in that region of the island. This epidemic clearly established that bats were the mode of transmission, and therefore, as the epidemic ended, it suggests that no susceptible bats remained.
During the period from July 16, 1929 to September 27, 1929, 13 cases of rabies occurred in humans with 100% mortality. On the other hand, there was only 1 reported case of acute poliomyelitis in February 1929. This prompted the governor, on September 21, 1929, to declare acute poliomyelitis, encephalitis lethargic, and cerebrospinal fever, infectious diseases of the nervous system, as compulsory notifiable diseases. The immediate public health reaction was an intense investigation of sanitary conditions of all premises and the surrounding environment where cases had occurred. Despite prompt measures to have all nuisances removed and the sanitary conditions improved, the epidemic did not abate.
Rainfall records for the period May to June in 1927 to 1929 did not reveal an epidemiological association with disease distribution, and there was no apparent seasonal variation in cases except that there were no reported cases during the months of November and December (Figure 4). This may be attributed to the use of decorative lights in houses and on trees, and the playing of music during the festive seasons of both Diwali and Christmas, which occur during these months.
Our findings support the assertions that bat rabies is migratory and seasonal, shifting to new colonies along a quite definite path. 37 The epidemic progressed in a northeasterly direction and approximately at right angles to the line of declination which approximates the earth's magnetic field in Trinidad.
In conclusion, the only epidemic of rabies in Trinidad not only established for the first time the transmission of rabies by hematophagous (vampire) bats but continues to provide peculiarities that even presently remain unexplained. The bat rabies epidemic of 1923 to 1937 in Trinidad was migratory and seasonal, and its spatial diffusion appears to have been linked to land use/land cover. The pattern of spread appears to be spatially linked to land use/land cover.