
Abstract
To the Editor:
The abstract from the Wilderness Medical Society's 2009 Annual Scientific Meeting by Lazio et al 1 provides data regarding 6-minute walking test (6MWT) feasibility at high altitude (4365 m) in 124 healthy trekkers. The authors regard these data as the first reported experience of 6MWT in a high-altitude setting.
However, in 2006 we performed extensive 6MWTs at low and high altitudes (500, 2000, and 2900 m) in both healthy people (24 subjects) and cardiac patients with left ventricular dysfunction (45 subjects). 2
Our own experience refers to a lower altitude, but in a mountain setting (Monte Rosa, Western Alps). At each altitude tests were repeated 3 times, and data from the second and third tests were averaged (while the first, performed to get the subject familiar with the test, was discarded). We recorded heart rate and blood pressure at the beginning and at the end of the exercise; 2 during the test respiratory parameters (ventilation, oxygen uptake, carbon dioxide output, oxygen saturation [SpO2], and all derived parameters) were recorded by a portable device (unpublished data).
A total of 621 tests were performed (of which 207 were at 2900 m); each subject's performance was directly compared to his own at low altitude. A comparison between healthy people and cardiac patients was available at each altitude.
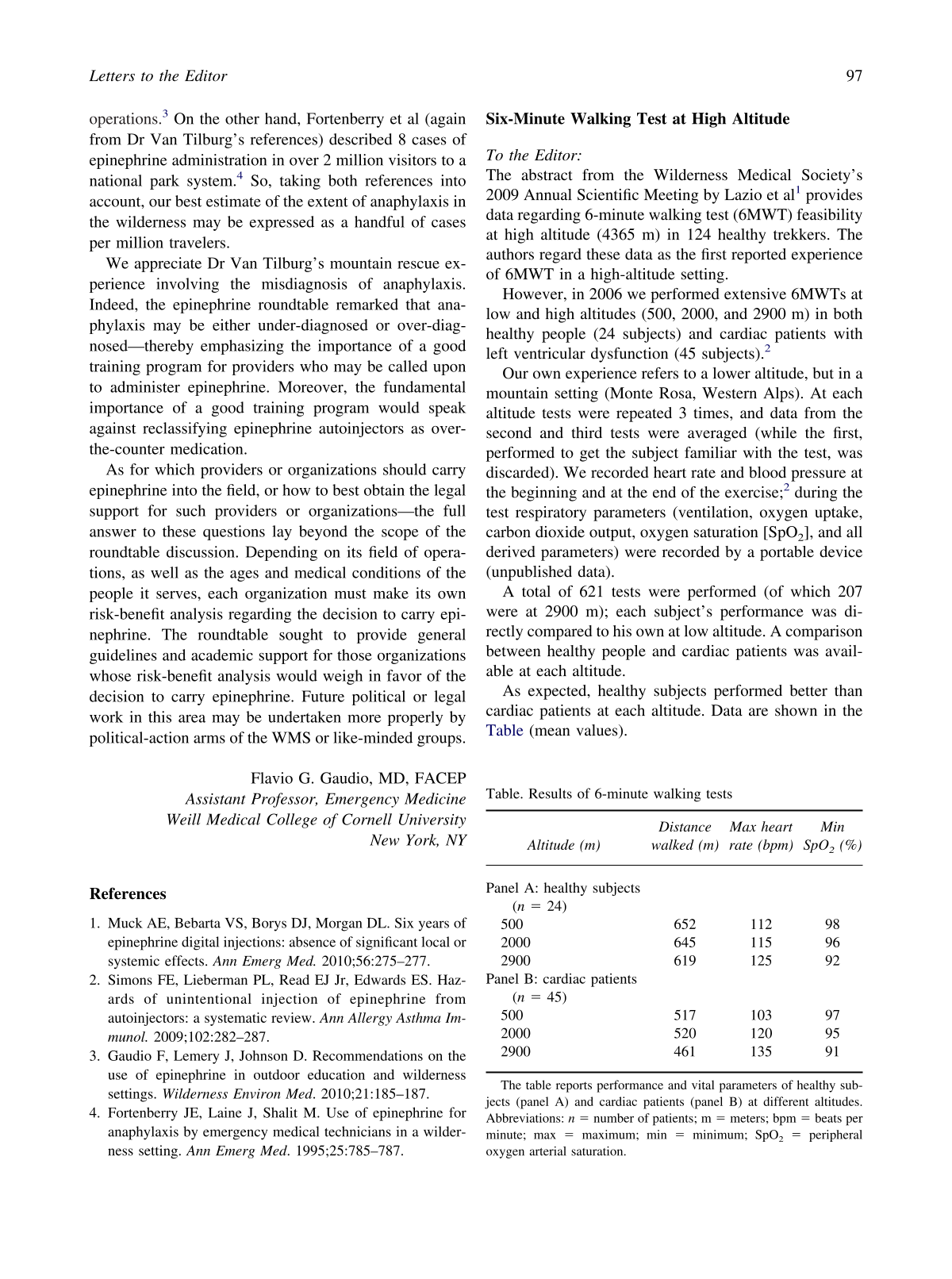
As expected, healthy subjects performed better than cardiac patients at each altitude. Data are shown in the Table (mean values).
Results of 6-minute walking tests
The table reports performance and vital parameters of healthy subjects (panel A) and cardiac patients (panel B) at different altitudes. Abbreviations: n = number of patients; m = meters; bpm = beats per minute; max = maximum; min = minimum; SpO2 = peripheral oxygen arterial saturation.
Performance at high altitude proved to be predictable by noninvasive functional evaluation at low altitude (echocardiogram, cardiopulmonary exercise stress test).
We believe our previous experience in 6MWTs at high altitude provided an extensive pool of data both in healthy subjects and cardiac patients. Despite the fact that the primary interest of our work was focused on rehabilitation of cardiac patients, we presented reference values of healthy subjects, compared to low altitude.