
Abstract
Only a few cases of nontraumatic orbital subperiosteal hematoma due to scuba diving have been reported, and this is the first of such cases that underwent surgical intervention. This injury results from negative pressure within the face mask, suctioning orbital tissues into the mask after incomplete equilibration of pressure on descent. Valsalva maneuver is a second mechanism implicated in the etiology of this injury. Recognition of this injury is of the utmost importance because vision loss is a possible complication if there is compression of the optic nerve or increased intraocular pressure. In many cases of nontraumatic orbital hematoma, conservative management is adequate; however, this case was an exception due to worsening exam findings. Divers may be able to prevent this injury by frequent and gentle equilibration of mask pressure on descent.
Introduction
Subperiosteal hematomas of the orbit are rare and most often result from trauma. Unequilibrated pressure in a scuba diver's mask is one nontraumatic cause. Four prior cases associated with scuba diving have been reported. 1 –4 This is only the fifth case of a scuba diving-induced orbital subperiosteal hematoma described, and it is the first case to undergo orbitotomy to correct worsening signs. Recognizing this entity has significant clinical value because compression of the optic nerve and intraocular pressure elevation are possible and can result in vision loss.
Case Presentation
A 45-year-old male recreational scuba diver with a history of occasional difficulty equalizing pressures within his mask was diving in Puget Sound and had difficulty equilibrating his mask pressure during descent at 45 feet (14 m) deep. He admitted having to blow very hard out of his nose to successfully relieve his mask pressure. Afterwards, he had mild left eye discomfort but no vision abnormalities. Using a dive computer, he dove to a maximum depth of 130 feet (39.6 m) and finished his dive without further incidence. All previous episodes of poorly equalized mask pressure were able to be equilibrated with positive pressure from nasal breathing. He was not experiencing nasal or sinus congestion and was not using decongestants. He reported no other reason he would have trouble breathing through his nose. His past medical history included hypertension, hyperlipidemia, and a gastric bypass 1 year prior. His medications included a daily 81 mg aspirin, bupropion, benazepril, and simvastatin.
The following morning, he presented to the emergency department because he noticed blurred vision, particularly with peripheral gaze. He reported a mild pressure-like headache behind his left eye. He denied chest pain, shortness of breath, focal motor or sensory deficits, and ataxia. Initial vital signs were blood pressure 156/90 mm Hg, heart rate 64 beats per minute, respiratory rate 12 breaths per minute, oral temperature 96°F (35.6°C), and 100% oxygen saturation on room air. On examination, he had diplopia on peripheral gaze in any direction but most notable on upward gaze. While the right eye was capable of all normal extraocular movements, the left eye failed to elevate completely on upward gaze. The patient's visual acuities were 20/25 in the right eye and 20/20 in the left eye. The remainder of his neurologic examination was normal.
A computed tomography (CT) scan of the head and face was performed and demonstrated a left-sided subperiosteal hematoma on the orbital surface of the frontal bone (Figure). Maximum dimensions of the hematoma were 22 × 22 × 8 mm. There was no evidence of encroachment on the optic nerve. No laboratory tests were performed. An ophthalmologist was consulted. After verifying normal visual acuities, intraocular pressures, slit lamp exam, and fundoscopy, it was felt no immediate surgical intervention was necessary.
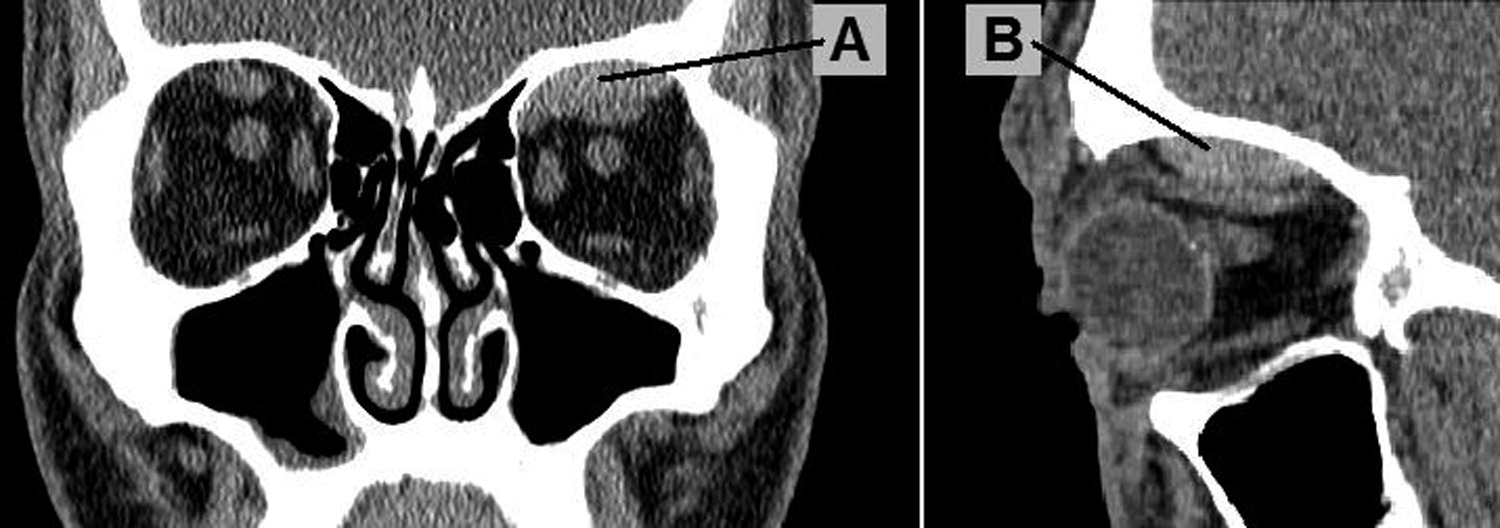
Noncontrast CT scan of the patient's face, revealing a subperiosteal hematoma on the orbital surface of the left frontal bone (A, coronal view; B, sagittal view).
On 48-hour follow-up with ophthalmology, decreased color vision, an afferent pupillary defect, 3 mm proptosis, and 2 mm inferior displacement of the globe were noted in the affected eye. Intraocular pressures were 16 mm Hg in both eyes. The ophthalmologist felt the hematoma was expanding and unlikely to reabsorb with observation alone. The patient underwent urgent surgical drainage via anterior orbitotomy 2 days after initial presentation. An incision was made superior to the globe using a superior orbital nerve block with procedural sedation. The periostium was dissected, and 3 mL of hematoma were evacuated with suction.
All signs and symptoms completely resolved immediately after the orbitotomy. The patient was informed by the ophthalmologist that he may be at increased risk of suffering a recurrence of this injury with further scuba diving. He was instructed to refrain from scuba diving for at least 2 months, which was the minimum time felt necessary for the orbit to recuperate from surgery. It was further recommended that he abstain from scuba diving indefinitely because of potential recurrence. A CT scan of the orbit 2 weeks after surgery revealed no remaining hematoma.
Discussion
Orbital hematomas are categorized into intraorbital and subperiosteal types. The less common subperiosteal hematoma is almost exclusively caused by orbital trauma.5,6 Nontraumatic causes of subperiosteal hematomas are most commonly associated with sudden elevations of cranial venous pressure such as weight lifting, 7 vomiting,8,9 and coughing. 10
Nontraumatic subperiosteal hematomas are more common in younger patients and have a tendency toward the orbital surface of the frontal bone. 11 The explanation for the location of injury centers on the fact that the periosteum is only loosely adherent to the underlying orbital bone everywhere except for along orbital fissures, the optic canal, and orbital margins. The orbital surface of the frontal bone is the largest uninterrupted boney surface in the orbit, making it the most susceptible to periosteal separation. The relationship between the periostium and underlying bone is believed to be weaker in younger patients before calcification occurs. 11
A review of the literature yielded only four prior case reports of scuba diving–induced orbital subperiosteal hematomas. 1 –4 The pathogenesis of these injuries due to diving is relatively straightforward. As a diver descends with face mask in place, the surrounding water pressure increases creating a relative negative pressure within the mask. This negative pressure, acting as a vacuum, is transferred through the orbital and facial contents inside the mask and to the orbital periosteum. Separation, vascular injury, and hemorrhage occur when this pressure exceeds the strength of the adhesion between the periosteum and underlying bone. Such injury can be prevented by mindful exhalation through the nares into the mask during descent to equalize pressure. Unfortunately, Valsalva maneuver, which can be created when equilibrating such negative pressure, is another mechanism implicated in the etiology of nontraumatic subperiosteal hematomas. 7 Blowing through the nose too aggressively while equilibrating mask pressure or hesitating to equilibrate mask pressure to the point where a much larger effort is required may contribute to the occurrence of a subperiosteal hematoma because Valsalva maneuver is mimicked in doing so. Thus, it is prudent for divers to equilibrate mask pressure gently and frequently as they descend. The patient in this case was subject to both the negative pressure of his mask and Valsalva maneuver created from the effort of equilibrating the pressure in his mask.
Inexperienced or inattentive divers may neglect or be unable to equalize mask pressures appropriately. This is typically uncomfortable and can cause capillaries to rupture when subject to the negative pressure. This is referred to as a mask squeeze, and subconjunctival hemorrhage, petechiae and ecchymoses of the skin, lid edema, and hyphemas can result. Divers may be asymptomatic despite the stigmata of their mask squeeze. Our patient did not present with these findings; however, these stigmata would be consistent with mask barotrauma when present.
Common to the scuba diving-related orbital subperiosteal hematoma cases published are pain, proptosis, limited extraocular movements, and diplopia. Of note visual acuity was grossly normal in all cases. The hematoma in this patient was pressing on his superior rectus muscle, interfering with its proper function, elevation of the anterior surface of the globe. Our patient's exam worsened on follow-up, and the ophthalmologist felt orbitotomy was indicated to prevent hematoma expansion from impairing the patient's vision. The four previous cases required no intervention and resolved over time without any major long-term sequaela. 1 –4 One patient did report at 3 months' follow-up that her affected eye remained more prominent than the other. 4 Our case is novel in that it is the first reported nontraumatic orbital subperiosteal hematoma where an orbitotomy was felt necessary. An orbitotomy was preferred over an image-guided needle aspiration for two reasons. First, the clot that had slowly formed would likely have been difficult to remove with needle aspiration alone. Second, orbitotomy would allow for safe visualization of other orbital structures that might not be seen well on image guidance, preventing inadvertent injury to a nonvisualized structure during the procedure.
Diagnosis of subperiosteal hematoma with CT or magnetic resonance imaging (MRI) has been successful. 1 –11 Treatment recommendations for nontraumatic subperiosteal hematomas center around conservative management, but needle aspiration or orbitotomy with drainage may be necessary. Surgical indications include elevated intraocular pressures, vision loss, or worsening signs and symptoms that suggest an expanding hematoma and impending vision loss. In the acute setting of significant vision loss or severely elevated intraocular pressures when expert ophthalmology consultation is not readily available, an emergent lateral canthotomy can be done as a temporizing measure to preserve vision until definitive ophthalmologic treatment is available. 4 ,12,13 If an orbitotomy is indicated, it should be performed by an ophthalmologist and necessitates expedient evacuation from a remote setting if vision is to be preserved. We recommend all patients with this injury be evaluated by an ophthalmologist whenever possible, but a patient with a stable examination, normal intraocular pressures, and no vision compromise may only need observation.
Decompression sickness (DCS) and arterial gas embolism (AGE) are two important entities that should be in the differential diagnosis of scuba diving injuries. Their consideration is important because both need treatment with oxygen and recompression. Both entities were felt not to be the etiology of this patient's signs and symptoms. AGE tends to be associated with lung injury on ascent and subsequent symptoms due to air embolism shortly thereafter. A patient may experience stroke-like symptoms if an AGE travels to the brain. DCS tends to occur due to air bubbles expanding in tissues on ascent. If air bubbles expand in cerebral or spinal tissues, neurologic deficits may occur. Both mechanisms did not match the history given by this patient: his initial symptoms occurred on descent not ascent, developed slowly over the next day, and were preceded by his mask barotrauma.
Footnotes
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of the Army or the Department of Defense.