
Abstract
Objective
Injuries to the flexor tendons and flexor tendon pulleys are frequently reported in rock climbers. Osteoarthritic changes with bone spurs are also well known. We report on the less commonly described extensor tendon irritation caused by such osteophytes.
Methods
Thirteen high-level rock climbers (12 men, 1 woman; average age 33.8 years [range 17–55]; average years of climbing experience 19 [range 5–30]; average climbing level 10.2) with extensor hood irritation caused by dorsally located osteophytes of proximal interphalangeal (n = 10) or distal interphalangeal joints (n = 3) were evaluated and managed. Twelve climbers received conservative therapy and 1 climber was treated surgically.
Results
Before treatment, the climbers were unable to achieve their normal climbing ability due to extensor tendon irritations with resultant effusion noted in the ultrasound examinations. After conservative treatment, and in 1 case surgery, all patients achieved their previous climbing ability.
Conclusion
While all climbers were able to achieve their former climbing level after treatment, the condition is progressive and the osteoarthritic changes will likely cause further problems for these idividuals in the future. Extensor hood irritation must be considered in the differential diagnosis of finger pain in rock climbers.
Introduction
Finger injuries are the most common injuries occurring in rock climbers. 1 –3 Most often the flexor tendons and their pulleys are affected. 1 In long-time climbers progressive osteoarthritic changes of the small finger joints have been observed. 4 –6 These changes can present as large bone spurs, on both the flexor and extensor sides of the digits. 6 With intensive use of the crimp grip position during climbing (Figure 1), these bone spurs can produce irritation to the extensor tendons, an observation that has received little attention to date. 6
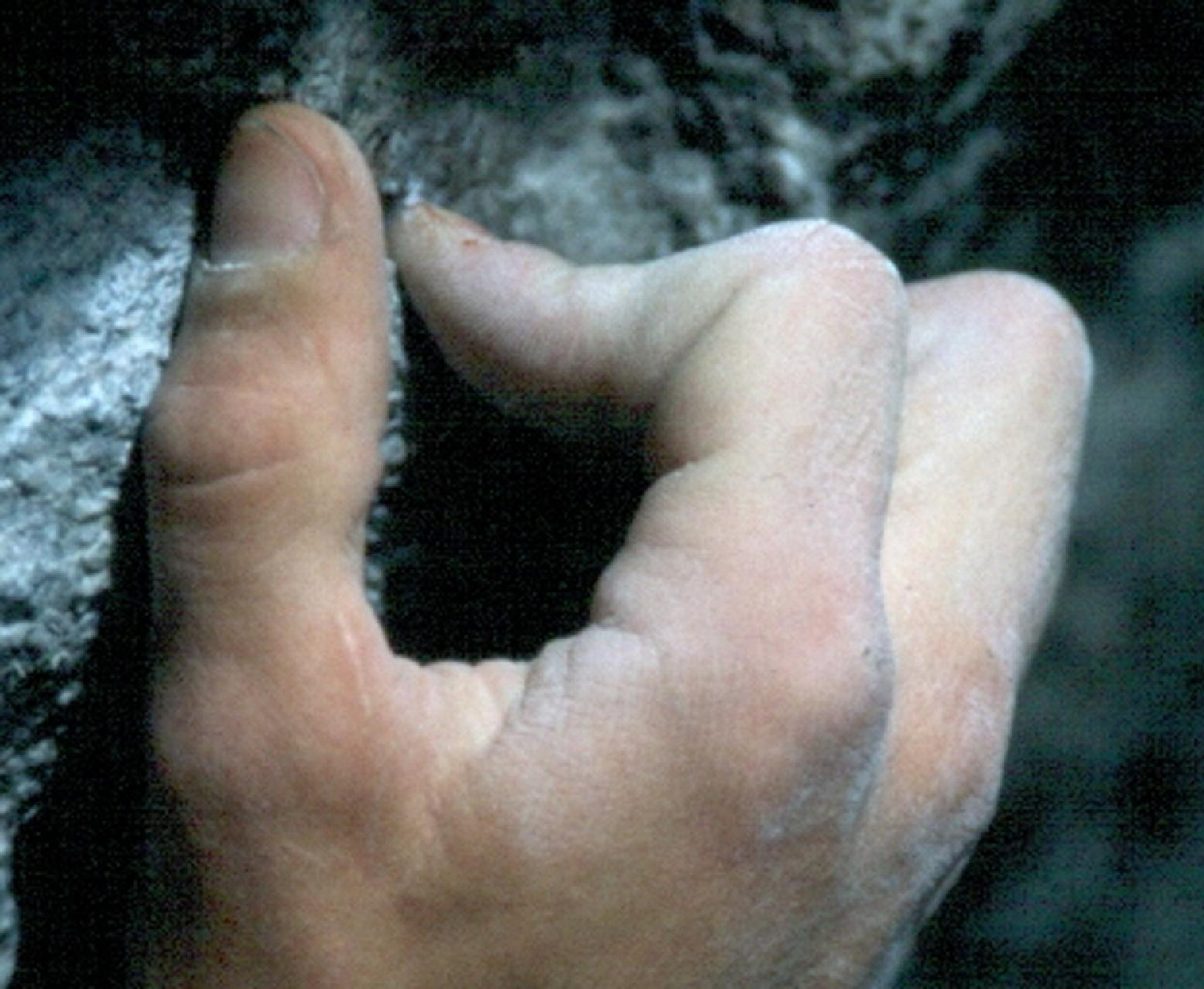
The crimp position.
Case Series
We treated 13 rock climbers in a 3-year period in our sportsorthopedic outpatient clinic (12 men, 1 woman; average age 33.8 years [range 17–55]) (see Table) complaining of dorsal-sided pain of the proximal and/or the distal interphalangeal (PIP/DIP) joints. They had been climbing at a high intensity for an average of 19 years (range 5–30) with an average climbing level of 10.2 (metric) (10+ UIAA [Union Internationale des Associations d'Alpinisme], or 5.14a US; range 9.0–11.3 metric). Physical examination demonstrated an extension deficit of 3–5 degrees of the PIP joint in 7 climbers, while flexion was mildly restricted in 4 climbers (distance of finger tip to palm in full flexion 0–1 cm). The PIP joint was affected in 10, and the DIP joint in 3 climbers. Ultrasound examination showed fluid and effusion around the extensor tendon hood, similar to a halo phenomenon in palmar sided tenosynovitis of the flexor tendons. Ultrasound also showed a change in the course of the extensor tendons due to osteoarthritic dorsal bone spurs. Plain radiographs revealed dorsal bone spurs (osteophytes) on the PIP joint in all climbers and on the DIP joint in 3 climbers (Figure 2). According to the Kellgren-Lawrence scale 7 the radiographs (in 7 cases bilateral) revealed 5 grade 2, 12 grade 3, and 3 grade 4 osteoarthritis. Each of these dorsal bone spurs was causing irritation to the extensor hood, resulting in fluid accumulation and tenosynovitis-like conditions, given that the extensor tendons do not have true tendon sheaths compared to the flexor tendons at the level of the DIP and PIP joints. In 2 cases the dorsal osteophyte had already broken off.
Description of climbers with extensor hood syndrome
Climbing level metric. DIP = distal interphalangeal joint; PIP = proximal interphalangeal joint.

Climber with 30 years of climbing with stage 4 osteoarthritis in the distal interphalangeal and proximal interphalangeal (PIP) joints and extensor hood irritation in the PIP joint.
In one young climber (20 years old, climbing level 11-/5.14b, climbing years 12, German Champion in Bouldering and Lead Climbing) the radiographs showed old epiphyseal fractures, which resulted in large bone spurs on both sides (Figure 3). These caused only mild irritation of the extensor hood and he has continued to perform at full level. Radiographs in this case were performed in follow-up after prior epiphyseal fractures some years earlier, during the yearly national team exams. One other young climber (17 years old) also had symptoms following epiphyseal fracture 2 years prior.

Extensor hood irritation after epiphyseal fracture. This 20-year-old athlete performs at full level and won the German Championships in both Bouldering and Lead Climbing.
All climbers initially received conservative therapy with stress reduction (avoiding crimping and limiting climbing to 2 levels under their highest ability), anti-inflammatory hand baths (eg, sulfur hand baths), ammoniumbituminosulfonate (20%) (Ichtholan®) ointment therapy, and nonsteroidal anti-inflammatory drugs. In 5 cases additional peri-tendineal local corticosteroid injection was performed. In all 12 symptomatic cases the conservative therapy led to good results: the climbers were pain-free after 3 to 4 weeks and were able to compete and climb at their previous levels. Although the bone spurs persisted, the inflammatory condition around the extensor hood was diminished in follow-up ultrasounds. In 1 case irritation persisted, and, therefore, the osteophyte was removed surgically (Figure 4). After recovery the athlete was able to regain his former level of performance.

The broken-off osteophyte at the PIP joint was surgically removed.
Discussion
Osteoarthritic conditions in long-time climbers are well known 2 –6 and several studies demonstrate that osteoarthritic changes in the hands of rock climbers increases with years of climbing.4,8 Epiphyseal fractures in young climbers can also lead to an early onset of osteoarthritis, especially if neglected and not treated correctly. 9 In young and highly active sport climbers (junior national team) stress-related osseous reactions were reported, 8 but a 5-year longitudinal study did not find that they lead to an early onset of osteoarthritis. 5 It is surprising that climbers with high-stage osteoarthritis in their fingers (Kellgren-Lawrence 7 grade 3 and 4) often do not complain about a high level of pain and discomfort. 6 Nevertheless they may have a remarkable decrease in range of motion and extensive radiographic findings. 6 It is not surprising that these dorsal- and palmar-sided osteophytes will lead to irritations of the tendons. In general, only flexor tendon problems, such as pulley ruptures, tenosynovitis, or tendon ruptures, 1 –3,10 have been reported in rock climbers. This is the first time extensor tendon problems have been reported in the literature. It is surprising that the climbers only presented with complaints of discomfort in the region of the extensor hood and not with osteoarthritic problems, other than minor morning stiffness. The clinical findings of osteoarthritic problems in climbers may not correlate with radiographic findings. Hochholzer and Schöffl 6 reported stage 4 osteoarthritic findings in rock climbers, which surprisingly lead to little discomfort. All but 1 climber recovered with conservative therapy alone. Rohrbough et al 4 assessed radiographs of the hands in veteran climbers (n = 65, average climbing experience 19.8 years) versus nonclimbing controls and found the rate of osteoarthritis not significantly different; however, the climbers were more often affected in specific finger joints. Nevertheless, the osteoarthritic conditions in these patients with bone spurs and osteophytes will persist and further future problems are to be expected. Ultimately, surgical removal of the osteophytes may become necessary.