
Abstract
Objective
The “Register's Annual Great Bike Ride Across Iowa” (RAGBRAI) is a 7-day recreational bicycle ride with more than 10,000 participants covering 500 miles. The heat and humidity of late July in Iowa, the prevalence of amateur riders, and the consumption of alcohol can combine creating the potential for a significant number of injuries. The purpose of this study is to determine the type, quantity, and severity of injuries on RAGBRAI and gather data on the factors related to these incidents.
Methods
This retrospective chart review examined ambulance “run sheets” for patients requiring transport to the hospital from the bike route between 2004 and 2008. These run sheets included name, age, chief complaint, anatomic location of injuries, medications administered, procedures performed, and a full narrative describing the initial scene, patient's account of the incident, services provided, and ongoing condition of the patient while en route to the hospital. Chi-square tests, Pearson's correlation tests, and t tests were applied to determine significant statistical outcomes.
Results
From 2004 to 2008, Care Ambulance Inc provided on-route medical services for 419 RAGBRAI participants. Of these participants, 190 (45.3%) required transport to a local hospital by Care Ambulance Inc. Females were more likely to require transport, as they comprised 46.3% of transported patients while only representing 35% of all RAGBRAI participants (P = .001). For men, increasing age was a significant predictor of transport, particularly males between the ages of 60 and 69 years old (P = .01). Of the 148 run sheets where mechanism of incident was documented, 114 incidents were caused by rider factors (77.0%), 29 by road factors (19.6%), and 5 by bicycle factors (3.4%). Higher heat indexes were correlated with an increased number of dehydration cases (r = 0.979, P = .02). Of participants who reported with minor injuries to a mobile first aid station and did not require transport, 90.1% had not imbibed any alcohol. Bony injuries were more common above the waistline as 39/45 (86.7%) fractures occurred to the clavicle, shoulder/proximal humerus, hand, or head. The most common bony injury each year of RAGBRAI was a clavicle fracture, which represented 44.4% of all recorded fractures from 2004 to 2008. Lacerations and abrasions were also more common above the waist, as 63.5% (127/200) of soft tissue injuries requiring treatment were either to the head or upper extremities. No specific event day showed any correlation with increased injury (P >.05).
Conclusions
This study suggests that females and older males are more likely to require transport for injuries sustained on RAGBRAI, the majority of injuries occur around the head and upper extremities, dehydration case load is correlated with heat index, and that incidents are usually caused by rider factors. This research could be used by multiday recreational bicycle tour organizers to continue educating riders on riding carelessness and etiquette and prepare medical services for certain quantities and types of injuries.
Introduction
In 1973, 2 writers on staff with the Des Moines Register challenged each other to a bicycle ride across the state of Iowa and printed an open invitation in their newspaper for any who would join them in their journey. That year 114 cyclists rode across the state of Iowa in 6 days. In 2008, 10 000 participants rode across Iowa in 7 days, in what is now referred to as the “Register's Annual Great Bicycle Ride Across Iowa” (RAGBRAI).
RAGBRAI, currently in its 38th year of existence, occurs annually the last full week of July. The event is limited to 10 000 registered riders each year but often sees up to 3000 additional nonregistered riders join the course daily. The entirety of the ride is 450 to 500 miles and held exclusively on county and state roads. Individual day rides are between 50 to 85 miles long. Traffic on daily routes is limited, although not completely blocked by the Iowa State Patrol.
Participants start RAGBRAI in a town near the Missouri River, the western border of Iowa and camp in 6 “overnight” towns as they bike across the state to finish at the Mississippi River, the eastern border of Iowa. Much of the camping is in residential yards, fairgrounds, high school baseball fields, etc. There are 6 to 10 “pass-through” towns on each day's route between the respective overnight towns. These pass-through towns provide food, drink (including alcoholic beverages), and entertainment along the daily route.
Since RAGBRAI's inception, 44 states have initiated noncompetitive multiday recreational bicycle tours. Providing medical support for these events is challenging. While previous studies done on touring bicycle rides in Maryland produced evidence for the predictive value of touring bicycle experience concerning injury, 1 and similar studies in California showed a correlation between heat and dehydration, 2 few studies have categorized the mechanisms causing incidents and none have compiled more than 1 year of data.
In this study, we quantify the incidence and predictors of injury from 5 consecutive RAGBRAI's dating 2004 to 2008 while also categorizing the mechanisms causing bicycle incidents, epidemiologic factors associated with injury, and the effect of temperature and humidity on dehydration case loads. Identifying injury incidence and predictors may enable medical personal to properly prepare and organize for similar events, while information on accident etiology, demographics, and proper hydration will prove useful to event coordinators hoping to inform and protect participants from possible hazards.
Methods
A retrospective chart review of medical services provided on RAGBRAI from 2004 to 2008 was performed. Medical services provided during RAGBRAI are divided between the participating towns that usually provide a local hospital or paramedic service to attend to medical issues arising within that town's limits and a privately owned ambulance service, Care Ambulance Inc, which is contracted by RAGBRAI coordinators to provide first aid and transport for riders injured between participating towns. Four Care Ambulance Inc ambulances split the medical support responsibilities, each ambulance being assigned a quarter of that day's bicycle route. Each ambulance is staffed by a certified emergency medical technician (EMT), a nurse, and a first-year resident of the Emergency Medicine Residency Program at the University of Iowa Hospitals and Clinics (UIHC).
The University of Iowa Hospitals and Clinics also provides a mobile first aid unit that is parked near the center of that day's route. This mobile first aid unit provides participants with non-emergent care such as minor cut and blister bandaging, icing/wrapping, sun block, and over-the-counter analgesics.
The information used for this research was provided by Care Ambulance Inc and the UIHC mobile first aid station and included only medical services provided between towns. Information regarding medical services provided within town limits by each participating town's hospital or ambulance service was not available. This study was created as a cross-sectional sampling of medical service requirements, specifically on-route services, and not a comprehensive listing of all injuries occurring on RAGBRAI.
The study used transport records and injury logs from RAGBRAIs completed between 2004 and 2008. Participants with minor injuries (sunburn, blisters, joint aches, minor cuts, etc), who presented to the mobile first aid station or parked Care ambulances, were documented in a paper injury log. Entry into the injury log included age, state of residence, chief complaint, services/products provided, miles trained prior to the event, and number of alcoholic beverages consumed that day. Participants whose injuries were severe enough to require transport to a local hospital as determined by responding medical services were documented in ambulance transport records or “run sheets.” These run sheets included name, age, address, chief complaint, anatomic location of injuries, medications administered, procedures performed, and a full narrative describing the initial scene, patient's account of the incident, services provided, and ongoing condition of the patient while en route to the hospital. Due to a change in documentation, transport run sheets from 2004 through 2005 were documented on paper, while transport run sheets from 2006 to 2008 were documented electronically into an online medical record database.
Patients who presented with symptoms including cramps, nausea, vomiting, dizziness, weakness, or hypotension and subsequently treated with intravenous fluids were classified as “dehydrated.” To assess the effect of heat on these participants, the ambient air temperatures and dew points of each RAGBRAI day were gathered from a weather archive on
Mechanism of incident was interpreted from the run sheet narratives describing initial scene of incident and patient/bystander accounts of the incident. The mechanisms were separated into 3 general categories: rider factors, road factors, and bicycle factors. Rider factors included any contact with other riders or the admitted inability to control one's own bicycle. Road factors pertained to any noted defect or obstacle created by the riding surface. Bicycle factors were any incident caused by complication or failure of bicycle equipment.
This research was approved by the University of Iowa's Institutional Review Board.
Results
From 2004 to 2008, Care Ambulance Inc and the UIHC first aid station provided medical services for 419 RAGBRAI participants. Of these participants, 190 (45.3%) required transport to a local hospital by Care Ambulance Inc. Females were more likely to require transport, as they comprised 46.3% of transported patients while only representing 35% of all RAGBRAI participants (P = .001) (Table 1). For males, increasing age was a significant predictor of transport, particularly males between the ages of 60 and 69 years old (P = .01) (Table 2). Of the 148 run sheets where mechanism of incident was documented, 114 incidents were caused by rider factors (77.0%), 29 by road factors (19.6%), and 5 by bicycle factors (3.4%) (Table 3). Higher heat indexes were correlated with an increased number of dehydration cases (r = 0.979, 2-sided P value = .020) (Figure). Of participants who reported with minor injuries to the UIHC mobile first aid station and did not require transport, 90.1% had not imbibed any alcohol. Bony injuries were more common above the waistline, as 39/45 (86.7%) fractures occurred to the clavicle, shoulder/proximal humerus, hand, or head. The most common bony injury each year of RAGBRAI was a clavicle fracture, which represented 44.4% of all recorded fractures from 2004 to 2008. Lacerations and abrasions were also more common above the waist, as 63.5% (127/200) of soft tissue injuries requiring treatment were either to the head or upper extremities (Table 4). The average number of transportable injuries per event day ranged from 3.6 average transports per year on day 7 to 6.2 average transports per year on day 5, but no day showed any significant correlation with increase in injury (P >.05).
Percentage of males and females requiring transport for their injuries the separate and combined years of RAGBRAI 2004–2008 and the statistical significance when compared to the consistent annual demographic of male participants (65%) and female participants (35%)
Distribution of participants of RAGBRAI 2004–2008 requiring transportation according to age and gender
Total and percentageof incidents credited to rider factors, road factors, and bike factors the combined years of RAGBRAI 2004–2008 with delineation of specific occurrences
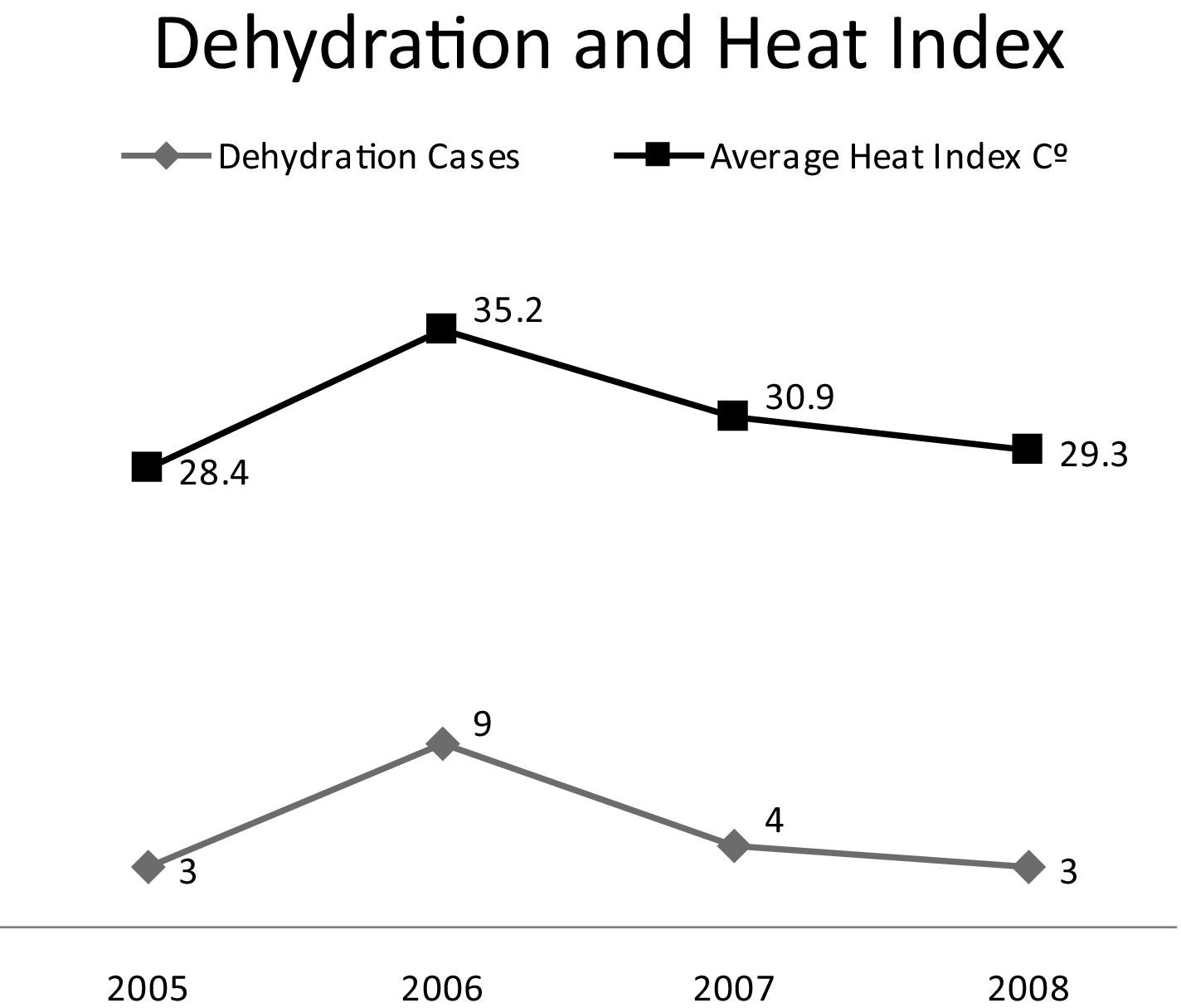
Correlation of increasing dehydration cases requiring transport to increasing average heat index (°C) the week of RAGBRAI 2005–2008.
Number and anatomic location of bony and soft tissue injuries each year of RAGBRAI 2004–2008
Discussion
The purpose of this study was to quantify the incidence and mechanism of incidents occurring on route on a multiday recreational bike ride while also gathering information on other injurious factors such as alcohol and heat.
The majority of incidents were caused by rider-related factors such as contact with other riders and loss of balance. This finding of rider liability was contradictory to a common belief among RAGBRAI participants that road conditions, including cracks, unfinished shoulders, and sand, are to blame for the majority of accidents. An attribution error likely rooted in news stories of bicycle incident injuries caused by poor road quality, including the highly publicized 2004 death of a rider from severe head trauma whose front wheel caught a crack in the highway. 3 The family of the rider sued and collected from the county responsible for the maintenance of the road, leading the county to bar RAGBRAI from being held within the county thereafter. 4 Information about rider complicity in injury should sway organizers to focus the majority of their injury prevention information on rider etiquette and contact prevention while still pursuing road quality and personal health surveillance by riders.
Analysis of dehydration cases requiring intravenous fluids showed a significant correlation between average heat index for the week and the number of transportable heat-related cases. This correlation was most apparent from 2005 to 2006 when severe dehydration cases tripled from 3 to 9, as the average weekly heat index rose 6.8°C, from 28.4°C in 2005 to 35.2°C in 2006. Heat-related injury has been noted in previous research as one of the more common injuries on multiday recreational bike rides,5,6 but this correlation between heat index and emergency medical resource use gives special credence to the need to escalate appropriate hydration efforts as temperature and humidity combine to cause heat indexes over 30°C.
Female participants were more likely to require transport for their injuries. Annual RAGBRAI demographics remained steady between 2004 and 2008 with 65% of riders being male and 35% female, while total ambulance transport demographics for males and females from 2004 to 2008 were 54% and 46%, respectively. Being female as an injury risk factor was indicated with a 1-day recreational bike tour of New York 7 but was not found statistically significant in a multiday recreational bicycle tour of Massachusetts. 8 The reasons for women requiring increased medical assistance during a recreational bicycle tour are unclear. It is possible that women are more likely to be injured seriously after bicycle incidents. It is also possible that men are injured with equal or increased frequency but are less likely to seek medical aid.
Previous research done concerning recreational bicycle rides found younger participants (<35 years old) were more likely to be injured but were unclear as to the demographics of participants requiring transport. 9 This survey found participants older than 45 years of age were more likely to require transport for their injury or illness. This was especially true for older males between the ages of 60 and 69 years. It is likely that this rise in transport with age is due to age-related deconditioning as most injured participants in this age group presented with symptoms of dyspnea, tachycardia, or chest pain.
Both bony injury and soft tissue injury were more common above the waistline. Disproportionate localization of injuries to the upper half of the body could be due to “clipping in” (wearing shoes that attach to the pedals of the bicycle). As clipped in riders fall they may be unable to free their legs for use as protection, leaving the wrists, elbows, shoulders, and head to absorb the majority of the force caused by the accident or fall. Clipping in will likely remain a mainstay of recreational bike tours as it allows for longer, less effortful riding. Medical personnel should prepare appropriately by stocking shoulder slings, c-spine collars, and other upper body-specific medical supplies.
Alcohol was not found to be a significant factor with respect to injury prevalence, although there is a statistically significant correlation between alcohol and serious or fatal bicycle injuries outside of the mass gathering environment. 10 It should be noted that individual alcohol consumption records were acquired through self report at the UIHC mobile first aid station or parked ambulances and may have been under-reported due to embarrassment or fear of legal recourse.
There is no increase in transportable events early, mid, or late in the week of RAGBRAI as no specific event day showed any correlation with the number of transports. The final day (day 7) averaged the least number of transports with 3.6 per year and was the most likely to be a statistical outlier but is also consistently the day where the fewest miles of RAGBRAI are ridden.
Other limitations to this study were similar to those confronted with other retrospective chart studies. Personal information such as name, age, and sex were standardized on each run sheet, but the circumstances of each individual incident, although well documented, were written in prose and therefore open to interpretation. An example of this is the interpretation of dehydration, which could be similar in presentation to gastroenteritis or even hyponatremia due to excessive water consumption, both of which require either further observation or laboratory results to verify. Five years of data provided a sufficient sample size but fostered inconsistencies across years in data collectors (different ambulance staff) and data collection forms due to a switch from paper to electronic file entry in 2007. To avoid these limitations, future studies of recreational bike tours that have alcohol en route could acquire blood alcohol content on scene and gather pre-ride verifications of training/experience to better ascertain their effects on injury occurrence. Also, standardized accident and injury log sheets could be created prior to the ride to increase uniformity across different years and different EMTs. Future prospective studies could examine the effects of pre-ride education concerning proper hydration and rider etiquette on dehydration and rider factor injury, respectively.
In conclusion, this study suggests that females and older males are more likely to require transport for injuries sustained on RAGBRAI, the majority of injuries occur around the head and upper extremities, dehydration is correlated with heat index, and incidents are usually caused by rider-to-rider contact or rider error. This research could be used by multiday recreational bicycle tour organizers to continue educating participants on rider etiquette and appropriate hydration while preparing medical services for certain quantities and types of injuries.
Footnotes
Acknowledgments
The authors thank Bob Libby and his crew with Care Ambulance Inc, T.J. Juskiewicz with RAGBRAI for demographic information, and Drs Schwemm and Trigger for previous data and guidance. Also, thanks Jeff Boeke for “living the dream” with me for 471 miles.
Supported by the University of Iowa Carver College of Medicine Summer Research Program.