
To the Editor:
Hiking from top to bottom of the Grand Canyon National Park in Arizona has been a popular endeavor for many years. The most common hike starts at approximately 2100 m above sea level and follows the South Kaibab Trail to Phantom Ranch at the bottom of the canyon (732 m above sea level) and back. The length (∼30 km), duration (6–9 hours), and inclination (∼13%) of this journey exerts extraordinary strain on the hikers' physique, which is influenced by dietary intake, backpack weight, and environmental conditions. The ambient temperatures at the canyon vary widely throughout the year, exceeding 38°C (100.4°F) in the summer months and falling below −18°C (−0.4°F) during the winter. 1 To prevent the risk of dehydration, heat stroke, hyperthermia, and hypoglycemia, especially in unacclimatized and inexperienced hikers, the Park Service does not recommend completing this journey in 1 day, as evidenced by numerous warning signs.
The intent of this letter is to highlight potential areas of further research regarding the physiological responses to desert hiking and severe environmental conditions. To carefully estimate the cardiopulmonary and metabolic demands during hiking in such an environment, 1 male (age: 31 years, weight: 77.2 kg, height: 179.0 cm) volunteered for a trial, following 5 days of acclimatization to the altitude. The hiker′s peak oxygen uptake (V
Accompanied by a research team, the volunteer hiker started from Yaki Point on the South Rim at 7:45
The ambient temperature during the day ranged from 15°C in the morning up to 29°C at 1:48
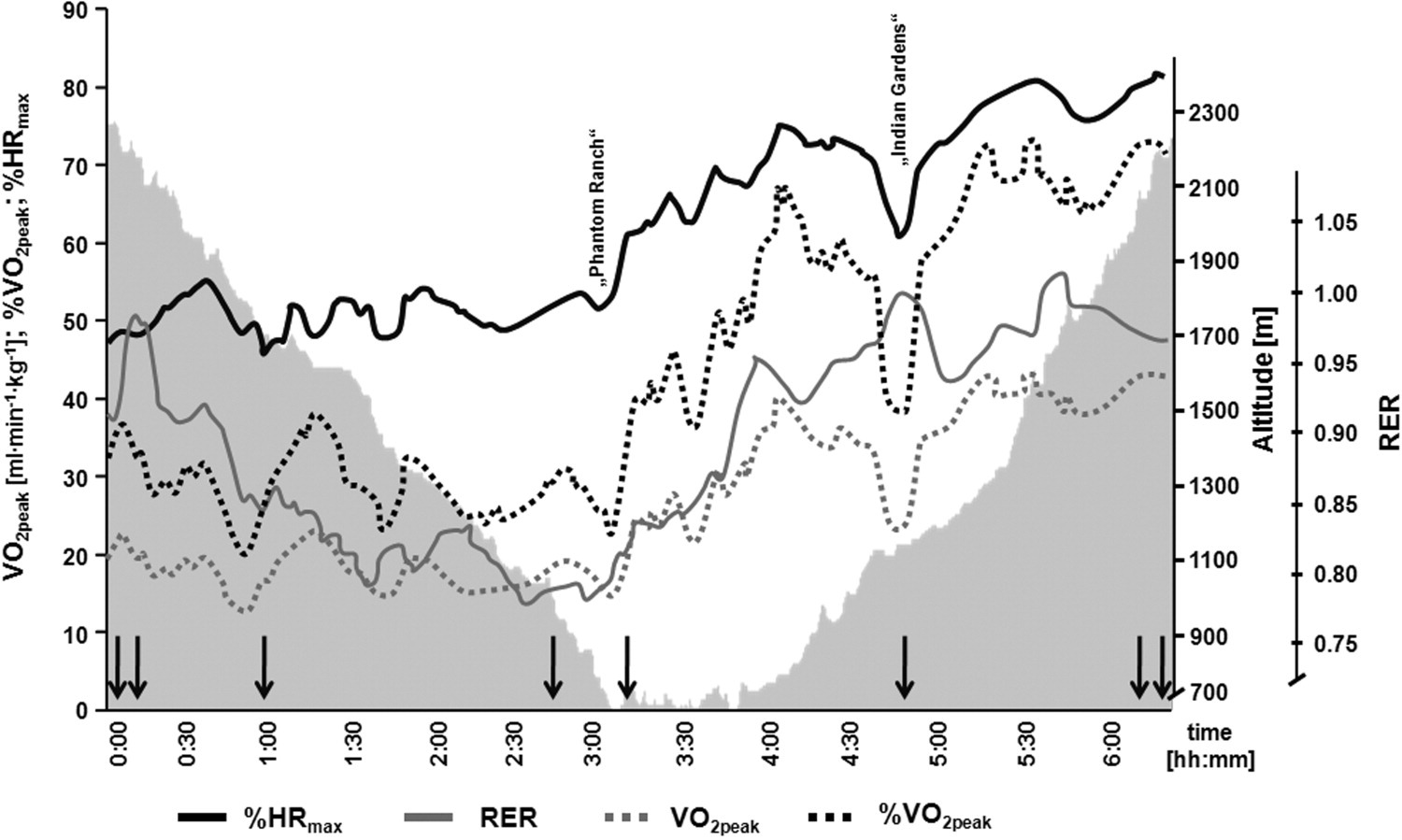
Subject's relative oxygen uptake kinetics (dotted grey), percent of V
Downhill Section
According to HR, V
Uphill Section
In general, the uphill part of the hike showed increasing cardiorespiratory values that peaked towards the end. Oxygen uptake and HR reached 75% to 80% of the individual's V
Close to Indian Gardens (a common resting point to collect water), Gluc levels declined from 138 mg·dL−1 to 58 mg·dL−1, indicating a hypoglycemic state. Food supply (Cliff Bar and 1.0 L of Gatorade) normalized the level of blood Gluc (96 mg·dL−1). The calculation of energy intake and energy expenditure at the end showed an energy deficit of 1226 kcal. This was due to an accumulated active energy expenditure of 3322 kcal, while the accumulated energy intake was 2096 kcal during the hike. This deficit demonstrates the need for proper caloric and fluid intake strategies to prevent harmful effects, such as hypoglycemia and compromised physical function. Nevertheless, despite the physical strain and the negative energy balance, blood Gluc levels were maintained as long as CHO were ingested.
Conclusion
Even though our volunteer could be classified as well trained and experienced in hiking, he developed hypoglycemia, reflecting the necessity for proper nutrition and hydration. From a physiological point of view, the profile of the hike exerts high demands on the cardiopulmonary and metabolic system and should not be recommended for physically untrained persons, especially during hot conditions. Despite the fact that this case only investigated 1 volunteer and 1 hike, this letter may help to highlight further research needs regarding the responses to desert hiking. These include: (1) nutrition; (2) clothing and equipment; and (3) physical fitness preparation for desert hiking.