
Abstract

To the Editor:
I'm writing in response to Dr Forgey's editorial, 1 Drs Welch, Clement, and Berman's research article (both published in Wilderness and Environmental Medicine), 2 and the new Boy Scouts of America (BSA) Wilderness First Aid (WFA) curriculum scheduled to take effect in March 2010. (Note: Dr Forgey was the task force chairman.) I understand that the BSA has requested endorsement for its program by the Wilderness Medical Society (WMS), and the WMS board has not, to date, taken any action.
Courses in wilderness medicine were originally developed in the early to mid-1980s because the urban first aid courses offered by volunteer organizations (American Heart Association, American Red Cross, National Safety Council, etc) and state emergency medical services/department of transportation courses did not—and do not—meet the specialized needs of outdoor leaders and search and rescue (SAR) teams. It currently falls to independent and unregulated providers to develop the curriculum and delivery methods for each course type and to the public to choose the course and provider that best meets its needs. Although this may not be the best overall construct for the future, the competition among providers has served to promote pedagogical diversity and has led to increasingly better curricula, materials, and delivery methods than were previously available.
Unfortunately, it is also increasingly more difficult for the general public and outdoor program administrators to decide what course and what provider best suits their needs. The challenge to the wilderness medicine community is to provide curriculum guidelines without negatively impacting the ability of individual providers to continue to develop pedagogical advances.
Wilderness medicine may be subdivided into two broad categories: expedition medicine and rescue medicine. Whereas the anatomy, physiology, and pathophysiology remain the same within both categories, specific skill sets vary. Medical training for trip leaders must focus on prevention, field assessment, and treatment (including evacuation decisions), whereas training for rescue team members requires more advanced treatment skills and equipment; evacuation is generally less of a concern as SAR teams tend to arrive on scene with evacuation plans and methods intact.
Courses in wilderness medicine, especially those marketed to outdoor leaders, must address a broad range of traumatic, environmental, and medical topics. As remote communication with rescue organizations increases, so too does the need for field judgment and, perhaps, rescue insurance. The medical training needs of individual outdoor organizations vary with their environments, activities, and participants. No single course fits all needs, and some minimum standardization would benefit outdoor program administrators in balancing the competency of their field staffs with the designs of their outdoor programs.
Similar to wilderness medicine, outdoor program risk management can also be subdivided into two broad categories: incident prevention and incident response (Figure 1). Training in wilderness medicine is integral to both. An effective wilderness medicine course should increase instructor awareness surrounding potential problems inherent in a program's course design and provide enough education and insight to prevent many of them. At the same time, it should teach the necessary assessment and treatment skills required to address the most severe problems should they arise.
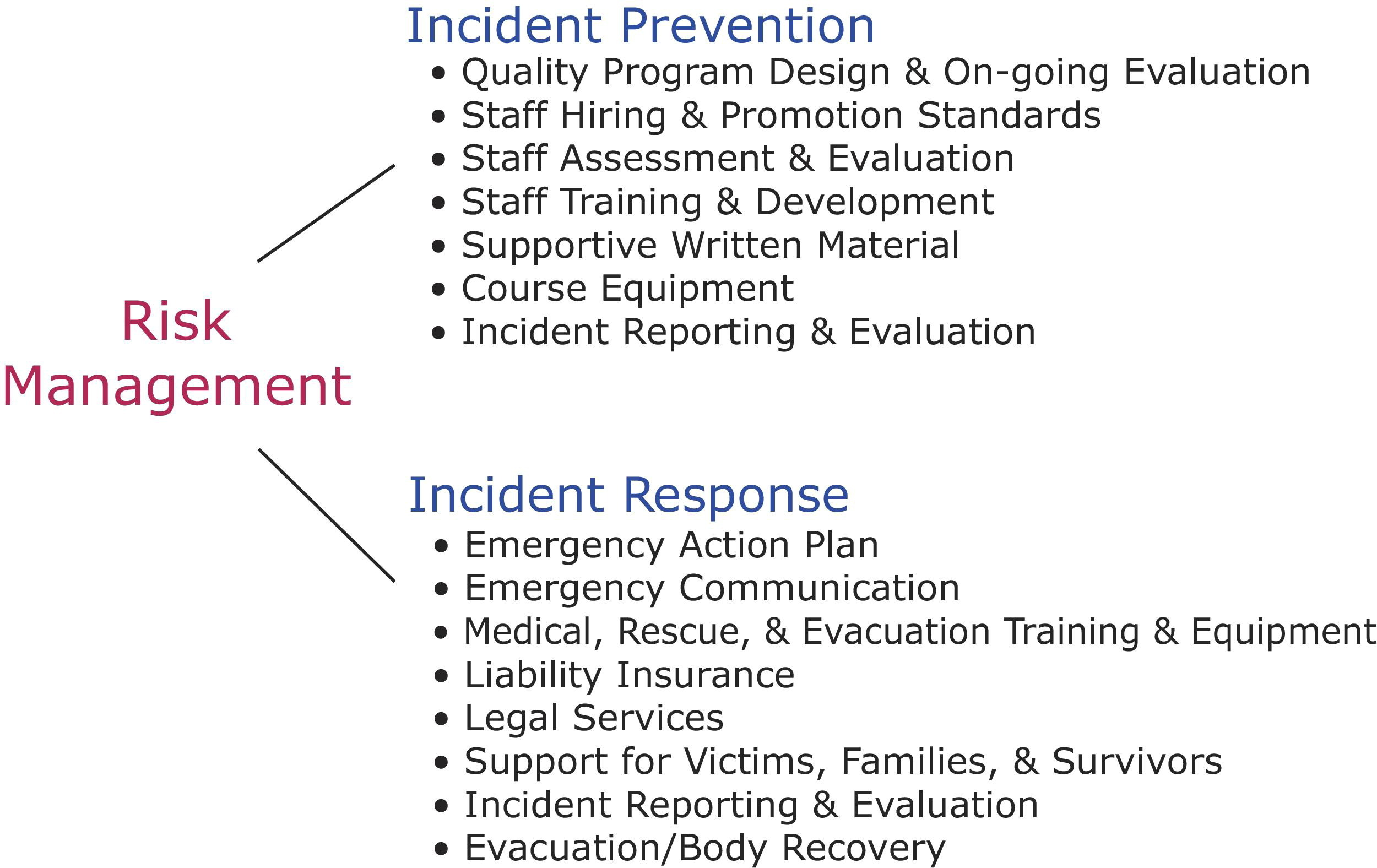
Outdoor program risk management categories.
There are three essential skill sets required to be effective in a field or administrative role within an outdoor program. They are outdoor skills, human skills, and educational skills. Briefly, outdoor skills are those skills required to ensure the safety of the trip participants and are specific to the trip activities (climbing, skiing, hiking, boating, etc). Human skills are the skills required to connect with, teach, and manage other people in a wilderness environment. Outdoor instructors must also have a solid grasp of the educational methodology—educational skills—required to ensure that their participants master the outdoor and human skills required for their safety.
Outdoor skills may be further subdivided into six separate skill sets that culminate with the mastery of the site management skills necessary to safely manage the program's activities (Figure 2). Although site management concepts and theory may be applied to all programs and activities, in practice site management skills are activity specific. Effective site management means a safe program and, like all instructor skills, requires training and mentoring to master. Mastery of the remaining five outdoor skill sets—technical, equipment, rescue, medical, and hazard recognition—are prerequisites to learning effective site management.
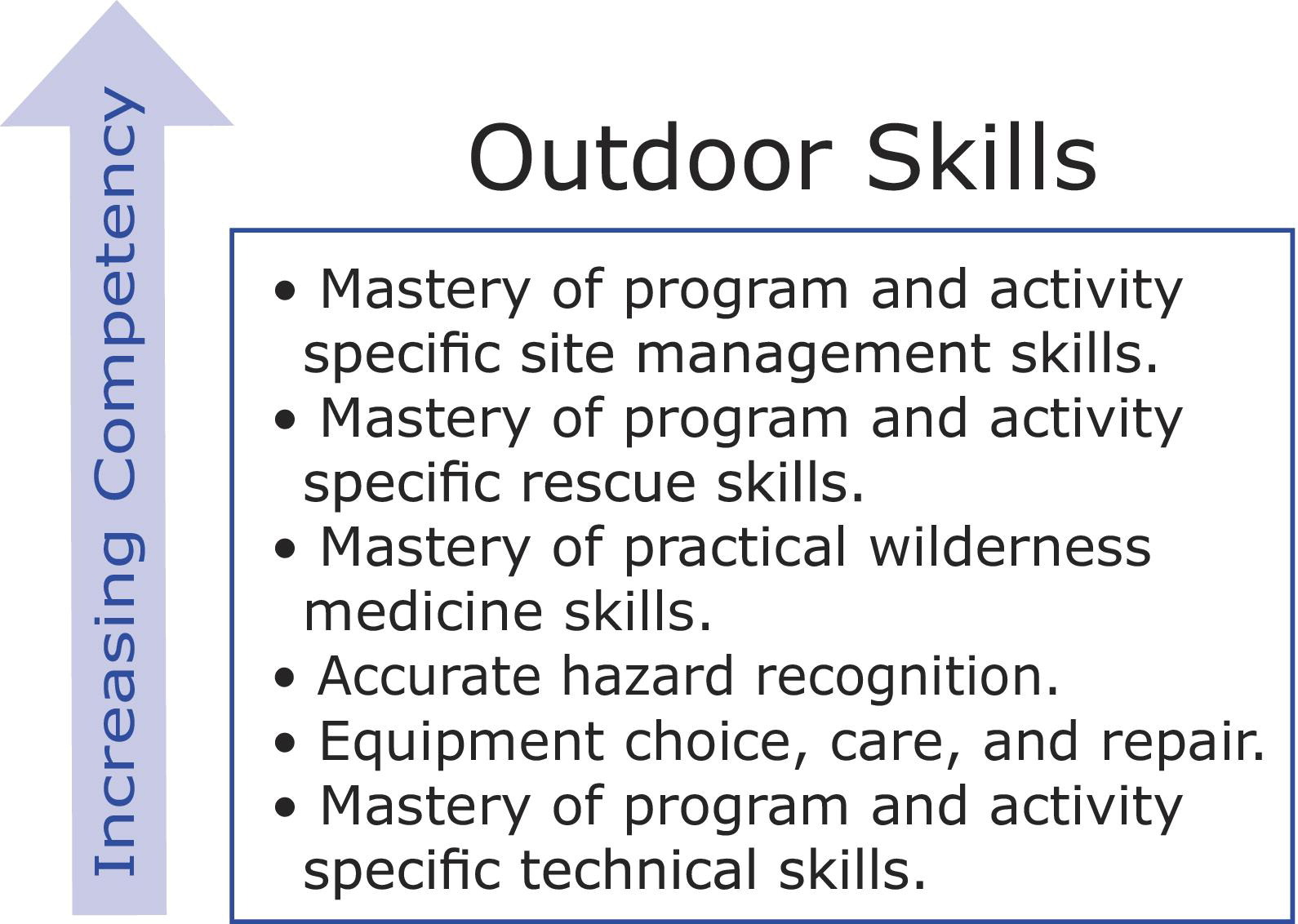
Outdoor leadership skills required for participant safety.
The wilderness medicine skills required for safety within a specific course design vary with the design (eg, mountaineering courses carry a greater inherent risk of injury than on-trail backpacking courses; trip leaders working at altitude require training in altitude medicine; etc). Varying course designs create the need for different types of wilderness medicine courses: Wilderness First Aid (WFA), Wilderness Advanced First Aid (WAFA), Wilderness First Responder (WFR), Wilderness Emergency Medical Technician (WEMT), Wilderness Advanced Life Support (WALS), and so forth. A WFA course may meet the needs of a day trip from a local camp with reliable emergency communication, whereas a 3-week expedition into a remote wilderness region with harsh environmental challenges and unreliable emergency communication will require a longer more comprehensive course (WFR). Regardless of the course type and curriculum, it falls on the outfitter or organization to ensure that its staff is trained to meet the specific needs of its program.
Designing effective courses in wilderness medicine is a complex process that must take into account numerous variables: (1) curriculum; (2) instructor training; (3) course materials; and (4) cost.
Curriculum
Although outdoor leaders should be proficient in operating within their course environments and capable of preventing, assessing, and treating minor injuries and illnesses inherent in their course designs, they are unlikely to encounter life-threatening problems. Therefore, their training must focus on the minor problems they are likely to encounter as well as those life-threatening and expedition medical problems they may—however unlikely—see. Though most wilderness medicine providers follow the WMS practice guidelines and/or guidelines presented in National Association of EMS Physicians (NAENSP) position papers, their curricula, materials, and delivery methods vary according to their pedagogical beliefs.
That said, there appear to be four basic curriculum requirements for all courses in wilderness medicine directed to outdoor instructors and trip leaders: A firm foundation in normal anatomy and physiology and the pathophysiology of the problems addressed to avoid ineffective “grocery list” assessment and treatment. Skills sessions that address the specific skills required for a trip leader within a specific course/program type (eg, splints, wound cleaning, basic life support, etc). Such skills must be demonstrated and practiced to a predetermined level of mastery if the training is to be effective. Realistic simulations that provide experience and lead to field judgment. Retention and judgment are directly related to field experience, and field experience is acquired through a thorough after-response analysis of an incident. For the overwhelming majority of trip leaders, this analysis must occur within the context of a course if it is to occur at all. This simple reality dictates that a large part of an effective wilderness medicine course must contain enough simulation time to allow students to make mistakes and to correct them. A progression and methodology that links all three of the above components into a cohesive whole.
The weighting of the above points is potentially arguable. It has been my experience that at minimum roughly 60% to 75% of any wilderness medicine course should consist of practical skills sessions, simulations, and case study review.
Instructor training
Effective wilderness medicine instructors should be experienced outdoor leaders with patient care experience, preferably in an outdoor environment, and have both training and experience delivering courses in wilderness medicine according to a carefully designed curriculum and methodology. Ideally, wilderness medicine instructors should have mastery of the outdoor skills required by their clients' programs as it is vitally important to teach practical field judgment, and said judgment is not possible without a complete understanding of the activity. Although advanced and extensive patient care experience is desired, it is generally not practical. Most professional outdoor leaders do not have the time or interest to pursue medical expertise nor do most medical professionals have the time or interest to pursue expertise in outdoor leadership. A balance is required, and instructor training must make up the gap.
The standard American Heart Association, American Red Cross, National Safety Council, and so forth, instructor first aid training model where a student becomes an instructor by taking a short—usually 1 day—instructor course does not work. In most cases, volunteers do not have either the medical or outdoor leadership experience to make good wilderness medicine instructors.
Course materials
Course materials vary with each wilderness medicine provider and may include a text, a waterproof or paper field manual, a case study workbook, patient field notes (commonly referred to as SOAP notes, an acronym for subjective, objective, assessment, and plan), data discs (CD or DVD) or videos, on-line testing, and so forth. The quality and depth of the materials also varies with the provider. As quality, quantity, and depth of materials increases, so does the cost.
Cost
Cost is generally a function of course quality and increases with higher instructor standards and training and the development of practical course curricula and materials. Courses delivered by providers with well-trained professional instructors and high-quality materials will necessarily cost more than courses with less well-trained instructors and lower-quality materials. It is a tribute to the well-respected professional wilderness medicine providers that they are able to reach and maintain their current rather high level of quality while at the same time keeping the costs of their courses significantly lower than those of corresponding training in other industries.
Standardization
Though there may be an advantage to the administrators of outdoor programs to have national minimum standards for individual course types—WFA, WAFA, WFR, WEMT, WALS, and so forth—it does not serve the outdoor industry as a whole to have strict curricula guidelines and an administrative bureaucracy. The current climate of competition permits a wide variety of delivery options that would not otherwise be available in a highly regulated climate.
Effective standards should be based on the length of the trip, the trip's activities and operating environments, whether or not reliable communication with a physician or SAR team is available, and the length of time to definitive care once the proper authorities have been reached.
The role—if any—WMS should take in proposing standards or curriculum guidelines is unclear. Certainly the WMS should continue to research and develop practice guidelines for wilderness care. I believe the WMS board should consider lobbying federal and state governments to legalize effective treatments that are currently illegal in many states (eg, epinephrine use, acute mountain sickness drugs for alpine guides, etc). Contrary to Dr Forgey's statement in his editorial, the WFR curriculum guidelines established by the WMS in 1999 have been embraced by most wilderness medicine providers. If similar guidelines for WFA, WAFA, WEMT, and WALS courses were also established—and the WFR guidelines updated—they would likely be embraced by the wilderness medicine providers, outdoor programs/outfitters, and the public at large if said providers had representatives on the guidelines committee.
The BSA Wilderness First Aid course as it is currently written provides an urgent case in point. Ironically, the course embodies many of the pedagogical errors discussed in Drs Welch, Clement, and Berman's research article. Whereas the content conceptually follows WMS practice guidelines, the length of the course—16 hours—is simply too short to effectively cover the topics listed in the syllabus; there is not enough time devoted to skills labs or scenarios to permit even rudimentary mastery. The errors are compounded when one considers the 14-year-old minimum age.
There is a risk that if the WMS board endorses this curriculum, the public at large will assume that this “should” be the way all WFAs are taught. I believe endorsement would be a disservice to all concerned and a grievous error. I believe the BSA and the general public would be better served if the BSA identified a core curriculum and minimum hours, leaving providers free to deliver the material in the manner—including hours—they think best. Perhaps an even better solution would be—as suggested earlier—for the WMS to form a committee composed of current providers to set minimum guidelines for WFA, WAFA, WFR (update), WEMT, and WALS.