
Abstract
A 44-year-old male presented to us with right hip pain and limb shortening following road traffic accident. He was diagnosed to have blunt abdominal injury, right hip posterior fracture dislocation, right knee dislocation with vascular injury. Though vascular repair was attempted, he ended up with an above knee amputation. Hip joint was unstable even after closed reduction and intraoperatively, gluteus medius avulsion was noted. This is the second reported case of abductor tendon avulsion in posterior hip dislocations.
Introduction
Posterior hip fracture dislocation with gluteus medius avulsion is a rare injury. To the best of our knowledge, there is only one case of such an injury which was previously reported. 1 Our patient also had an ipsilateral knee dislocation with popliteal artery injury further complicating the management. We present here the management of this complex injury.
Case report
A 44-year-old male presented to the emergency room with complains of pain over right hip, knee and inability to move the right foot following road traffic accident. The time duration from accident to arrival at the hospital was 5 hours. His vital parameters were glasgow coma scale (GCS-15), BP: 80/60 mmHg, pulse rate (PR): 102/min. On clinical examination, he had diffuse tenderness and guarding over the lower abdomen. Right lower limb examination revealed an unstable knee, tenderness over the hip, right lower limb shortening and absent distal pulses with foot drop. Hand held Doppler examination could not pick any pulse and saturation of the toes was not recordable.
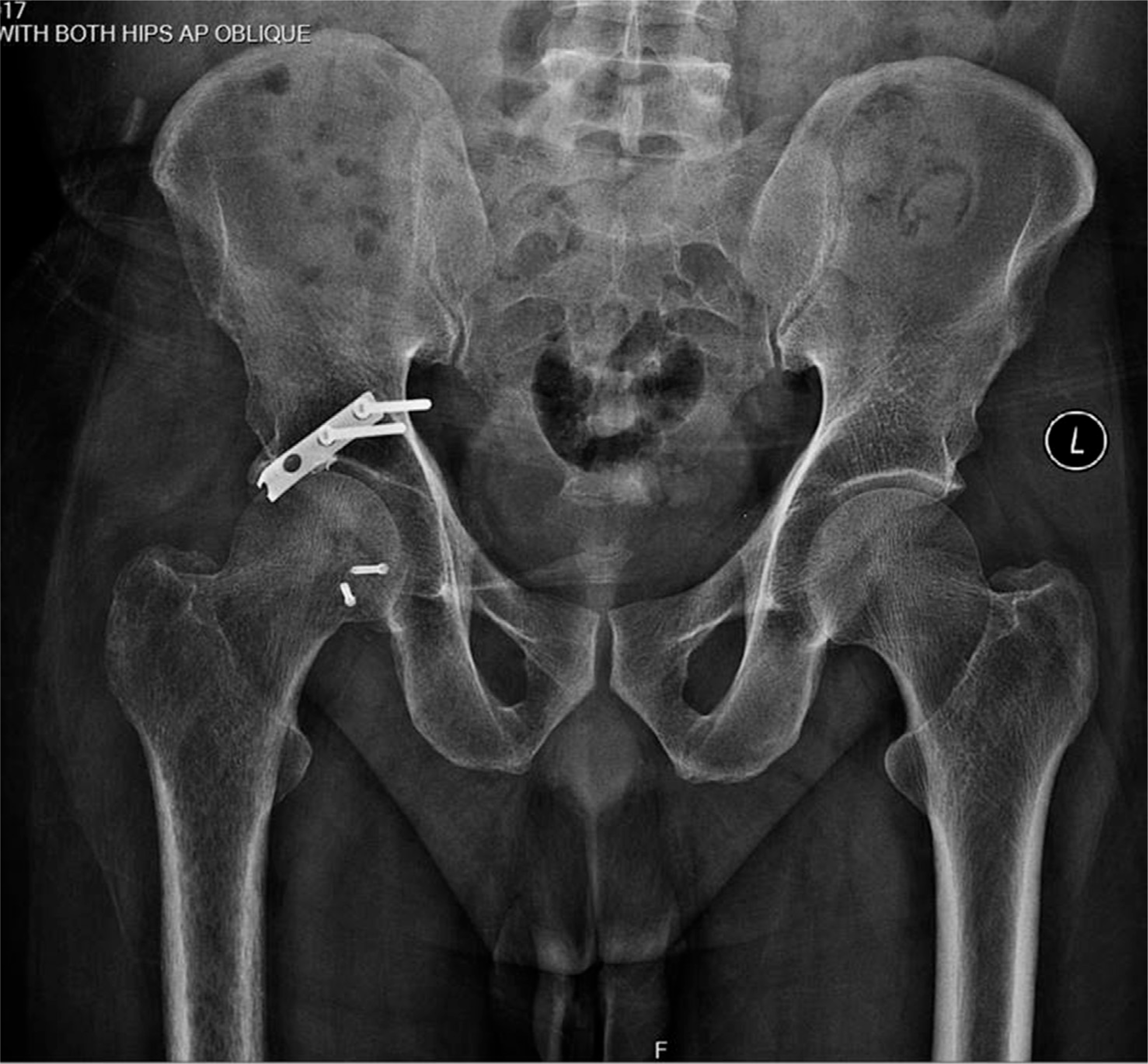
Patient was immediately resuscitated with fluids and blood. Plain radiographs and whole body computerised tomographic (CT) scans with contrast revealed air specks in the perihepatic region with minimal free fluid in perigastric region, jejunal perforation, right hip fracture dislocation, reduced calibre of right popliteal, posterior tibial, anterior tibial and peroneal arteries with segmental opacification of right posterior tibial in the middle and distal part (Figure 1).
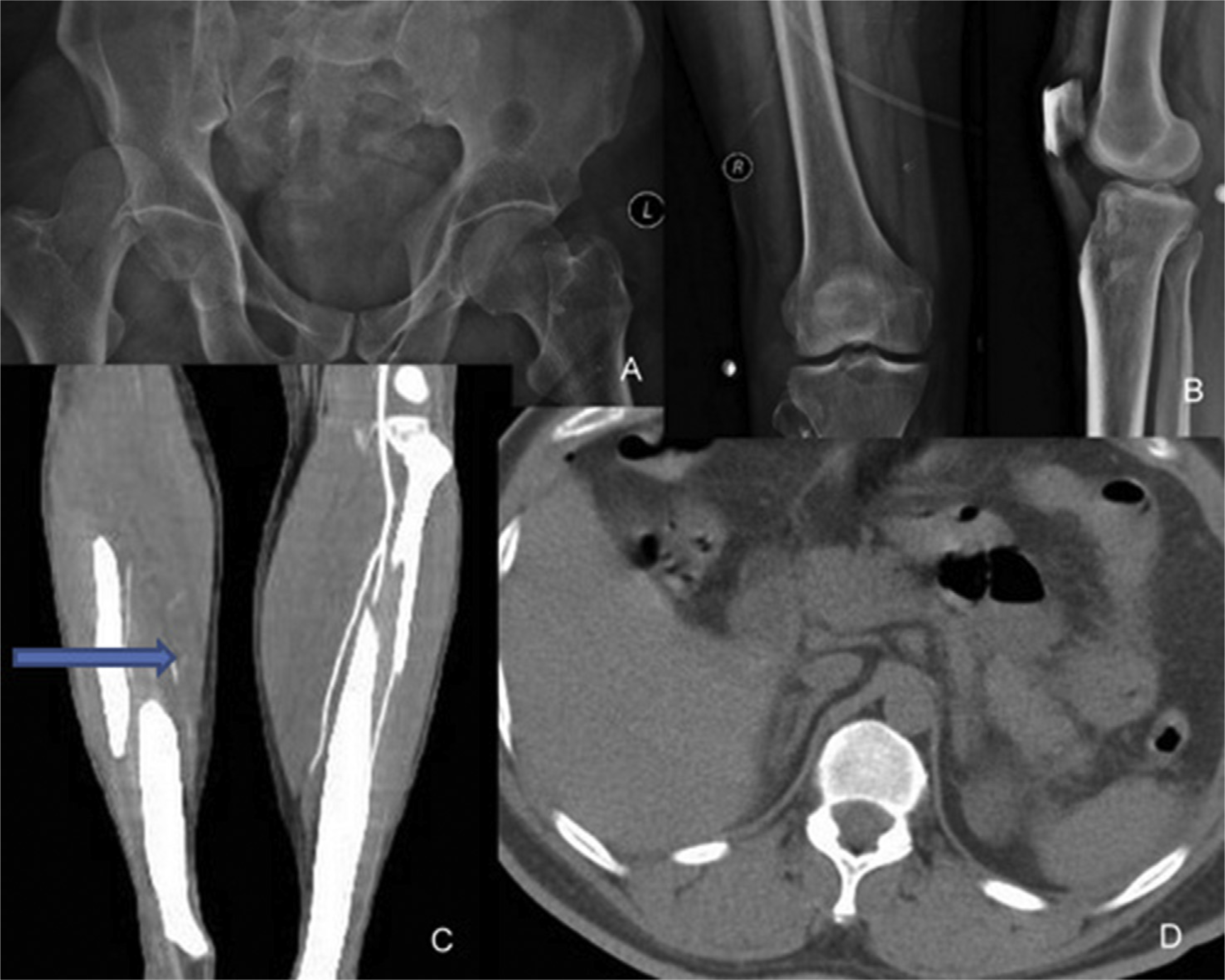
(A) Anteroposterior (AP) radiograph of pelvis showing right hip fracture dislocation; (B) knee radiographs after reduction in emergency room; (C) CT angiography showing reduced calibre of right posterior tibial and anterior tibial arteries; (D) CT abdomen showing air specks in perihepatic region.
Under general anaesthesia, patient underwent emergency laparotomy with repair of jejunal perforation, closed reduction of right knee joint and knee spanning external fixator application. As the limb ischaemia time was around 8 hours, patient was turned to prone position and popliteal fossa exploration was done. No pulsation was detected in the popliteal artery beyond a segment. This was repaired by bridging it with short saphenous vein graft harvested from the same leg. Following clamp release, good flow was seen across the graft site, and the foot was pink. However pulse and saturation could not be detected. We did not do a prophylactic fasciotomy. Patient was again turned supine and closed reduction of hip joint was performed, but it was found to be unstable.
Postoperatively, the patient developed deranged renal function tests and acidosis requiring dialysis. Limb vascularity was documented postoperatively with doppler and saturation probe but showed irregular waveforms. However his urine output decreased with worsening acidosis and blackening of right lower limb. He underwent above knee amputation 2 days following arterial repair and recovered well in the postoperative period.
Postreduction hip CT showed that the hip joint was still dislocated with a small posterior wall acetabular fracture and Pipkin II femoral head fracture. This injury was classified type 5 according to Thompson and Epstein classification (Figure 2). Five days following above knee amputation, he was taken up for acetabulum fixation. Under combined spinal and epidural anaesthesia, patient was positioned left lateral. Two 6.5 mm Schanz pins were applied to the femur in the antero-posterior and medio-lateral planes for providing traction. Through Kocher–Langenback approach, hip joint was exposed. Intraoperative findings included (1) femoral head fracture, (2) posterior acetabulum rim fracture, (3) capsulolabral avulsion and (4) complete gluteus medius avulsion. First, the femoral head fracture was fixed with two AO Herbert screws. Next the hip joint was relocated by applying longitudinal traction with the femoral Schanz pins. Then the posterior acetabular rim fracture was reduced and fixed with semitubular plate and suture anchors. Capsule and gluteus medius were repaired with transosseus ethibond sutures (Figure 3). After surgery, the hip joint was stable and congruent (Figure 4). Patient was initiated with passive hip range of motion exercises from 2 weeks and was non–weight-bearing for 8 weeks. Hip abductor strengthening was started after 4 weeks. Prosthesis was fitted at 2 months and tolerated–weightbearing was allowed with walker. At 6 months follow-up, patient is walking full–weight-bearing with above knee prosthesis without support and hip abduction power is grade 4 (Figure 5). Follow-up radiographs showed satisfactory healing without avascular necrosis (Figure 6).
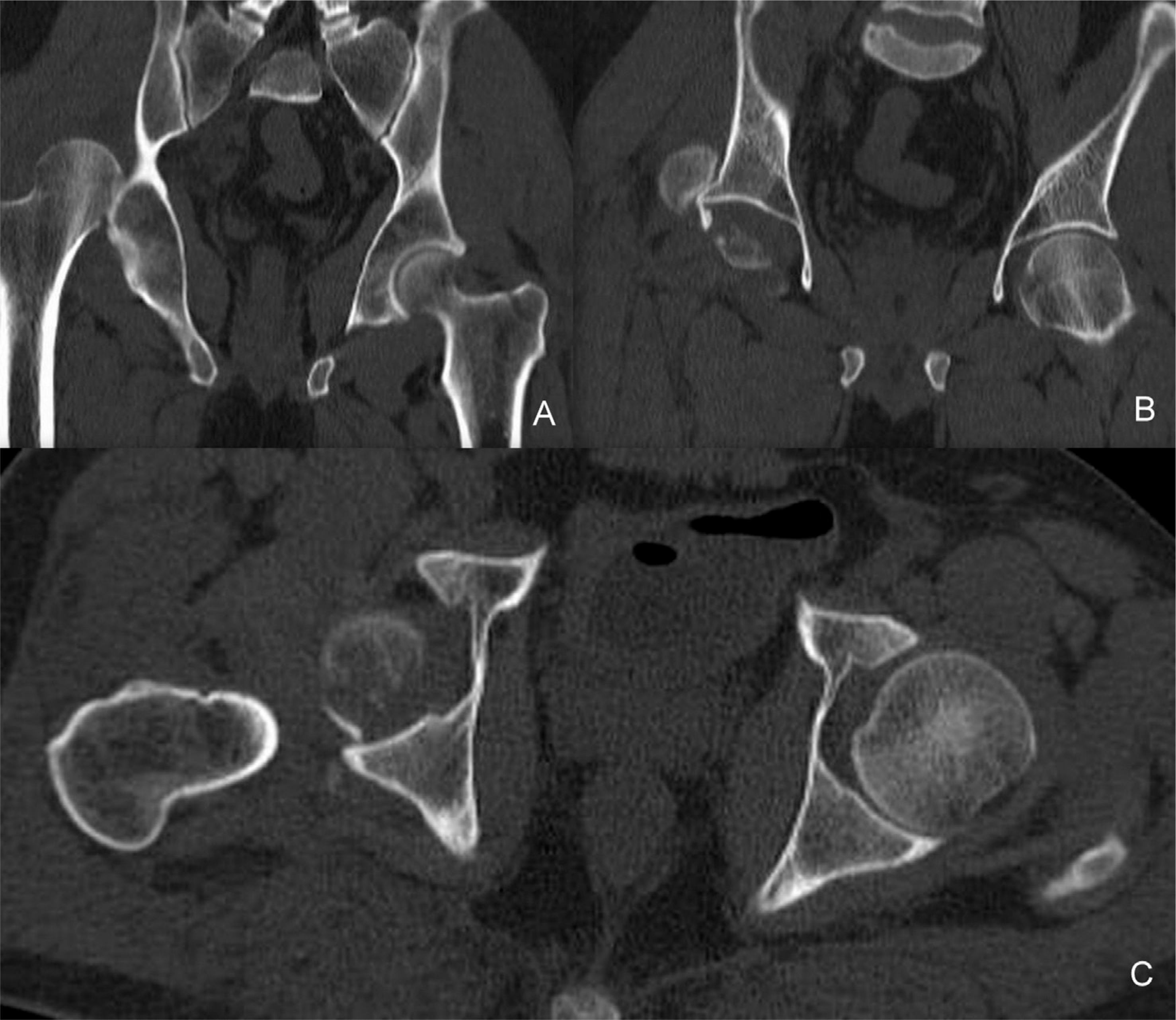
Representative CT cuts showing posterior hip dislocation with Pipkin’s II femoral head fracture. (A, B) Coronal cuts; (C) axial cuts.
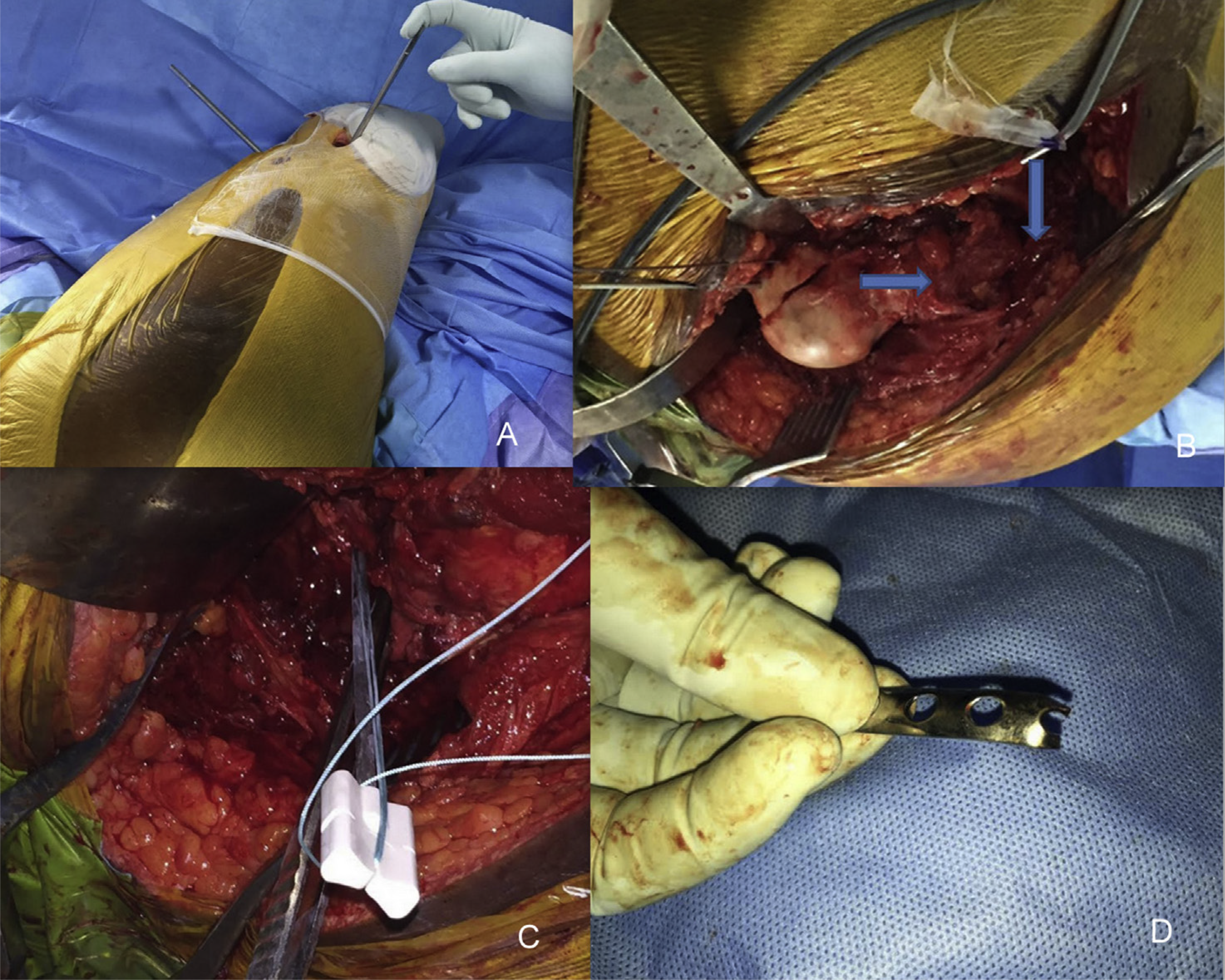
(A) Patient positioned lateral with two Schanz pins applied perpendicular to each other for providing traction; (B) arrowmark showing gluteus medius tendon avulsed off greater trochanter; (C) suture anchor applied to secure capsule and posterior wall fragment; (D) semitubular plate cut and bent at one end for use as spring plate.
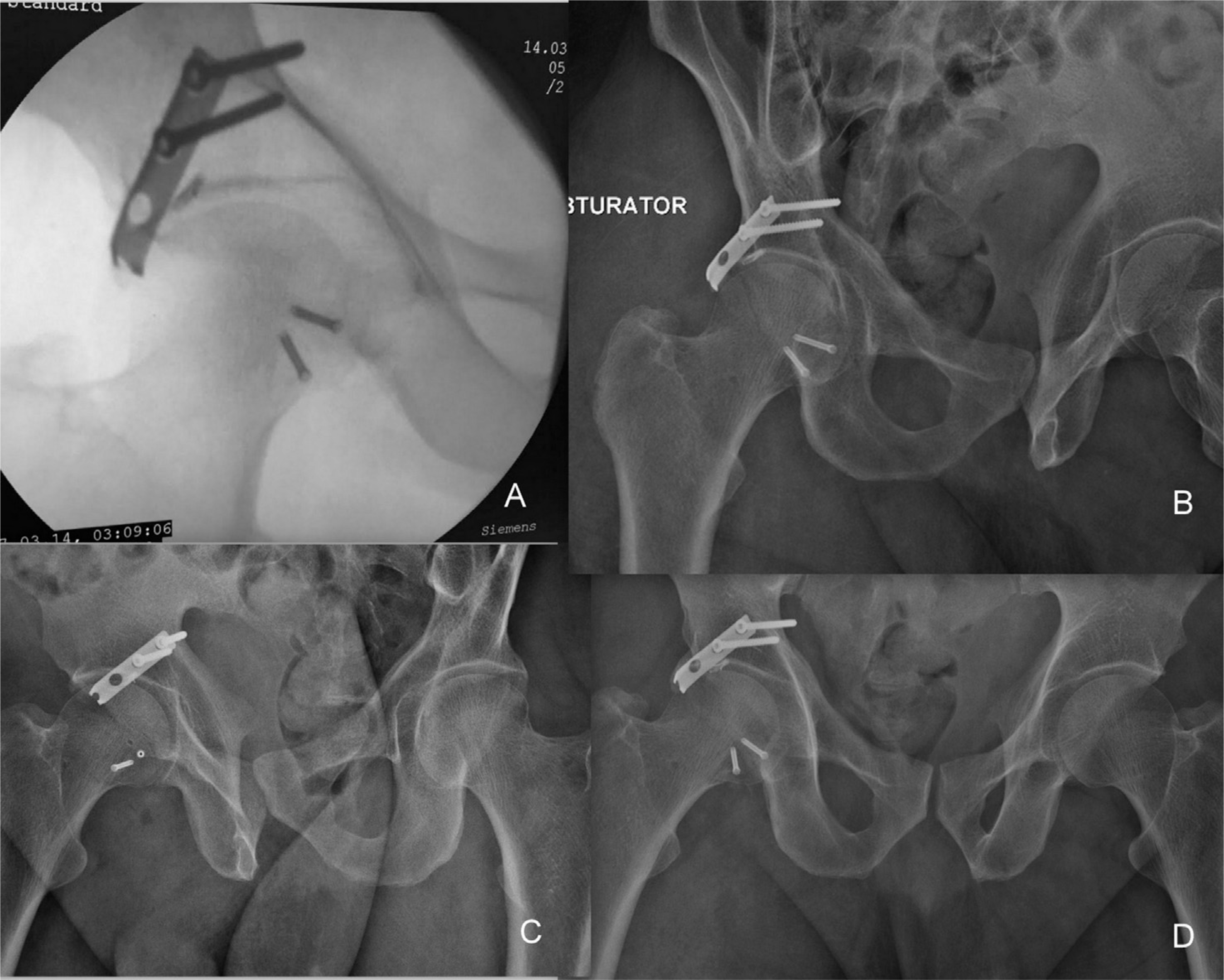
(A) Intraoperative fluoroscopy image showing congruent hip joint; (B) postoperative obturator oblique radiographs of pelvis showing satisfactory reduction and fixation; (C) iliac oblique radiographs of pelvis showing satisfactory reduction and fixation; (D) AP radiographs of pelvis showing satisfactory reduction and fixation.
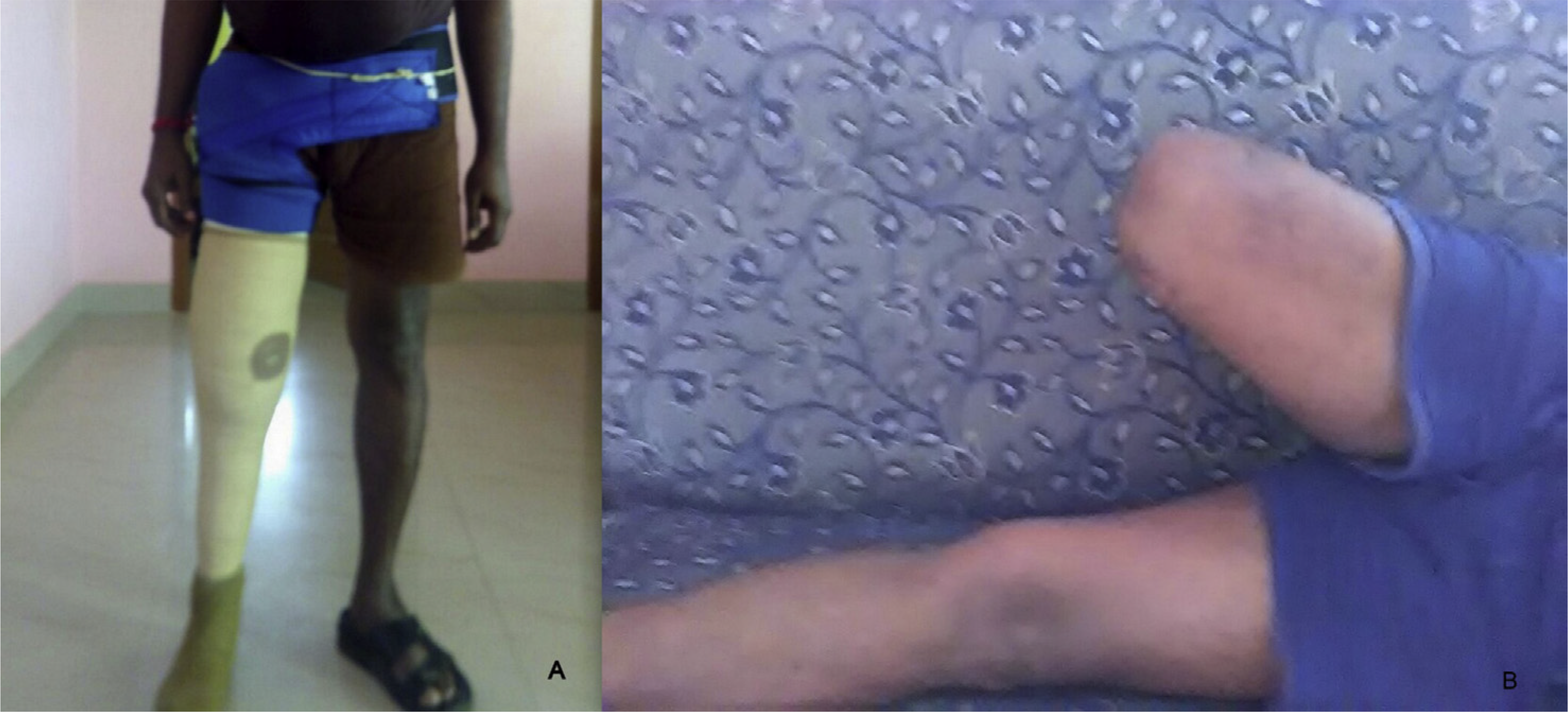
(A) One year follow-up clinical images demonstrating standing with prosthesis; (B) hip abduction.
One year follow-up AP radiograph of pelvis showing no evidence of avascular necrosis.
Discussion
Posterior hip dislocations constitute 80–90% of all hip dislocations. 2 Seventy percent of these injuries are associated with fractures of the acetabulum, and 25% are associated with knee injuries.2 Simultaneous ipsilateral hip and knee dislocations with popliteal artery involvement are rare with only few cases reported in the literature. 3 This is the second case report of gluteus medius avulsion associated with posterior hip fracture dislocation. 1
Knee dislocations are associated with popliteal artery injuries in 22–32% of cases. 4 The tethering of the popliteal artery at the adductor hiatus and soleal arch makes it vulnerable to injury. Delay in diagnosis and prolonged warm ischaemia time results in irreversible injury warranting an above knee amputation. Green and Allen reported an amputation rate of 11% if revascularisation was done within 6-8 hours and amputation rate of 86% if done after 8 hours. 4 The lower extremity assessment project (LEAP) study demonstrated an average warm ischaemia time of 7.25 hours for patients with amputation following knee dislocation and 4.7 hours for those not requiring amputation. 5 In this case the warm ischaemia time was 8 hours; however, in view of patients worsening general condition and darkening of foot following arterial repair, we proceeded with above knee amputation.
In our case, the unstable hip dislocation can be attributed to (1) posterior wall rim fracture, (2) femoral head fracture and (3) gluteus medius and capsulolabral avulsion. We first addressed the femoral head fracture via Kocher–Langenback approach for easier access. Femoral head being a large fragment was fixed with two Herbert screws. Secondly, the hip joint was relocated and acetabular rim fracture was reduced with K wires. As it was a rim fragment, we used a semitubular plate which was cut at one of the holes and bent. This was applied as a spring plate, and fragment was also secured with a suture anchor. Finally, we addressed the abductor tendon and capsulolabral avulsion with transosseus ethibond sutures.
A prospective study by Laorr et al on early magnetic resonance imaging findings in 18 cases of hip dislocations revealed femoral head contusions, fractures, osteochondral defects, labral tears, loose bodies, ligamentum teres entrapment, iliofemoral ligament injury and gluteus muscle injury. There were no documented abductor tendon avulsions. 6 A similar study by Tannast et al showed posterior wall fractures associated with obturator internus, gemelli and gluteus minimus avulsions. 7 Some authors have advocated magnetic resonance imaging in acute hip dislocation with stable posterior wall fractures for evaluating the aforementioned injuries. 8
Gluteus medius avulsion in a patient with grade IIIA open pelvic ring disruption and left posterior hip fracture dislocation has been reported by Urchak et al. 1 They proceeded with open reduction and internal fixation (ORIF) of pelvic ring disruption, and since the posterior wall fracture was comminuted, simple debridement and loose body removal was done. Avulsed gluteus medius was repaired with ethibond sutures through bony tunnels. Gluteus medius and minimus are referred to as the rotator cuffs of hip joint. Many authors have addressed degenerative and acute tears with transosseus sutures, suture anchors and endoscopic repair. 9 We used transosseus ethibond sutures for repair.
Fixation of the acetabular fracture in our case required Schanz pins to be placed in the femur for providing traction in view of previous amputation. This technique has been reported previously by few authors for bipolar hemiarthroplasties in above knee amputees. As the posterior wall fragment was a small rim fracture, a semitubular plate which was cut at one end and bent to create hooks was used as a spring plate as described by Ebraheim et al. 10
Conclusion
Ipsilateral concomitant hip and knee dislocation must be treated as a surgical emergency. Gluteus medius avulsion in posterior hip fracture dislocation is a rare finding, and this is the second reported case of such an injury. Though femoral head fracture and posterior wall rim fracture were the main causes of instability, intraoperative recognition of this injury yields better functional outcome.
Footnotes
Conflict of interest
The authors have no conflicts of interest relevant to this article.