
Abstract
Monteggia fractures are uncommon injuries, despite a high incidence of upper limb fractures in teenage children. We describe a case of a type 2 Monteggia variant in an adolescent. This injury pattern consisted of ulnohumeral dislocation in combination with type 2 Monteggia lesion. We discuss the possible injury mechanisms of this rare injury and review available literature.
Introduction
Elbow injuries are common in children and young adults, forming around 10-40% of total injuries; but monteggia fracture is relatively rare, affecting about 1.5-2% of this population. [1] The eponymous monteggia lesion was described in 1814 by Giovanni Batiata Monteggia as fracture of the proximal ulna with subluxation or dislocation of the proximal radius. Even the first patient described by him had a poor outcome due to persistence of radial head dislocation. [2].
Bado described the term true Monteggia and classified the fracture into four types based on direction of radial head dislocation. He also described Monteggia equivalents due to similarity of the pattern of injury to true monteggia. His equivalents were exclusively type 1 injuries. [1].
But since then many case reports have described equivalents in other Bado types. [3 –7].
We report a rare injury which has not yet been reported in the adolescent population. It could be included in the type 2 equivalent based on the mechanism and biomechanics of the injury.
Case report
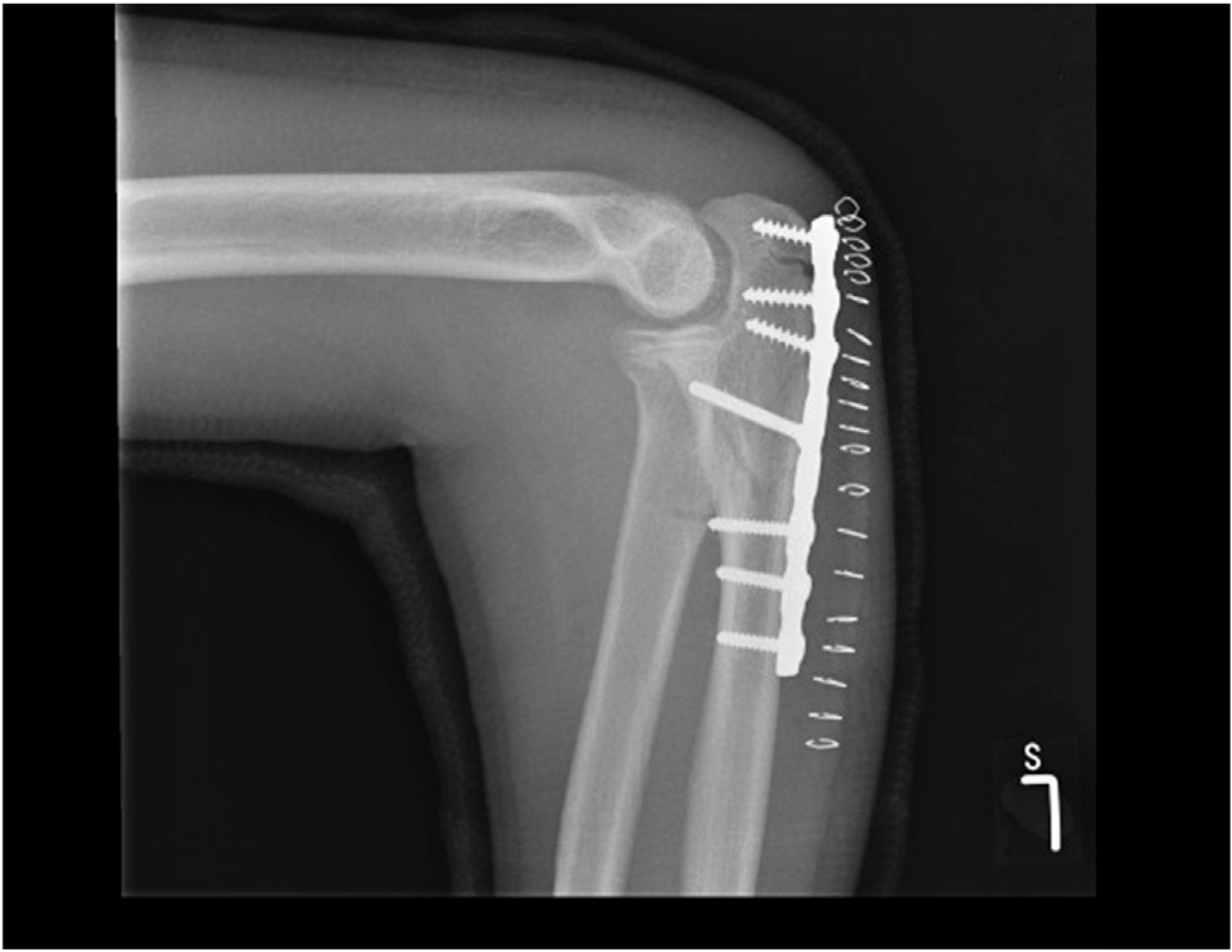
We describe a case of a 14 year old boy who sustained this injury. He sustained a fall from a climbing frame about 6-7 feet high. He claimed to have lost balance and fell on to his outstretched hand. He presented to accident and emergency department within 6 hours of the trauma. He had a swollen painful elbow with bruising on the posterior aspect of the elbow and forearm. There was flexion deformity at the elbow. Neuro-vascular status of the upper limb was normal. There was no other injury and the boy was systemically well. Radiographs revealed a fracture of the proximal ulna with apex posterior angulation of twenty degrees. The radial head was dislocated posterior. The ulnohumeral joint was also dislocated posterior (Figures 1 and 2). After initial treatment in a plaster of Paris back slab, the child was prepared for surgery. The ulnohumeral dislocation was reduced by manipulation; proximal ulna was anatomically and rigidly fixed using an interfragmentary screw along with a reconstruction plate for neutralization (Figure 3). The radial head reduced satisfactorily after ulna fixation and was stable. The ulnohumeral joint was also found to be stable in complete range of movement of the elbow. The elbow was subsequently immobilized in an above elbow plaster cast for 3 weeks followed by gentle assisted mobilization with a supportive sling for further 3 weeks. The patient had excellent functional outcome with no restriction to elbow range of movement. The fracture had united, both clinical and radiological, at 6 month review (Figure 4).
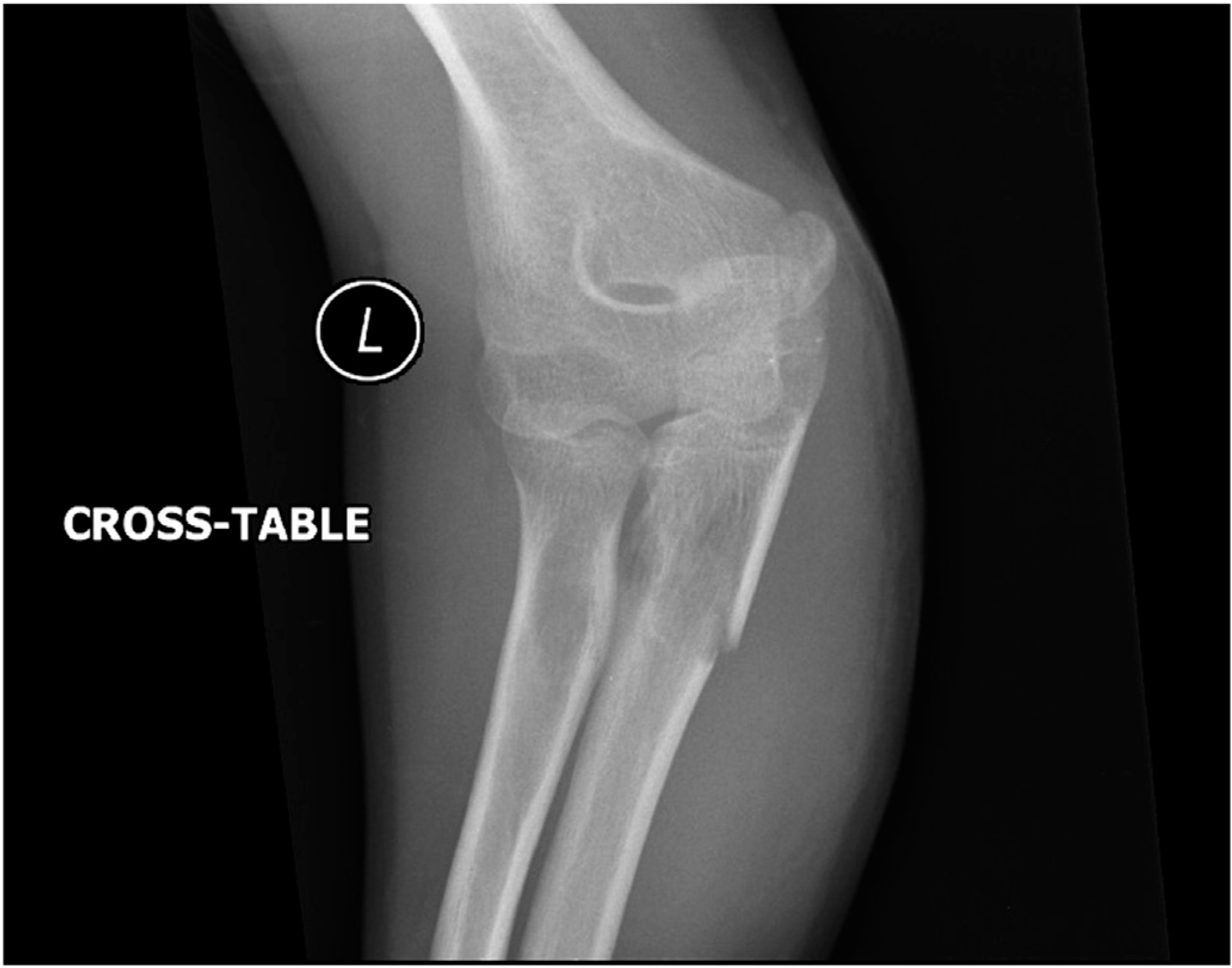
Injury radiographs of the described Monteggia variant.

Injury radiographs of the described Monteggia variant.

Postfixation radiographs of the injured elbow.
Elbow radiograph at six-month follow-up.
An informed consent was obtained from the patient and his parents for the treatment of the injury and publication of radiographic materials without any personal identification.
Discussion
Monteggia fracture can have significant functional loss if maltreated. Prompt diagnosis and treatment is essential. Bado classified it into 4 types, on the basis of direction of radial head displacement.
Type 1: anterior dislocation of radial head with apex anterior angulation of ulna fracture. Type 2: posterior dislocation of the radial head with apex posterior angulation of ulna fracture. Type 3: lateral or anterolateral radial head dislocation with apex lateral angulation of ulna fracture. Type 4: anterior dislocation of radial head with fracture of the radius shaft at or distal to the level of ulna fracture.
Bado supplemented his classifications with certain equivalents which shared a similar pattern of injury mechanism. All were type I equivalents and these included [1].
Isolated radial head dislocation (with plastic deformation of ulna). Fracture of proximal ulna with fracture of the radial neck and Both-bone proximal third fractures with the radial fracture more proximal than the ulnar fracture [8].
Over a period of time various other equivalents of type I Monteggia have been described which included pulled elbow syndrome, isolated radial neck fracture, fracture of ulnar diaphysis with anterior dislocation of radial head and an olecranon fracture [3 –7, 9]. These variants were predominantly seen in young children.
Though Bado stated that there were no equivalents of type II, III, IV Monteggia, but various investigators have described other equivalents on the basis of fracture characteristics, biomechanics and the mode of injury. [1, 8, 9] Considering the mechanism of injury as defined by Penrose [10] in type II Monteggia lesion, a posterior elbow dislocation could be considered as type II equivalent. According to Penrose for a type 2 Monteggia lesion to occur the forearm is in neutral rotation and slight flexion. The force is transmitted distal to proximal. He postulated that posterior elbow dislocation can result if the ligamentous support around the elbow prove to be weaker than the proximal ulna.
It is usually very difficult to determine the exact mechanism of injury in young adults, who are usually unable to provide precise details of the sequence of events [11]. However, the position of the forearm when the patient is first seen, the position of the distal radius on roentgenograms, the direction of dislocation of radial head, and the direction of angulation of ulnar fracture, all provide indirect clues about the mechanism of injury [12]. One of the most widely accepted theories is that isolated Monteggia fracture– dislocation is caused by hyperpronation as described by Evans [13]. However, Tompkins postulated that hyperextension of the elbow plays significant role in causing this injury [14].
There is sparse literature available on biomechanical cadaveric studies for causation of type 2 monteggia injuries. Tan et al conducted a finite element analysis on two cadaveric specimens and found that the radial head dislocation is due to a traction force rather than a transverse force. They also identified that the force transmission occurs through the annular ligament forcing the radial head out of the ligament. Both ulnar fracture angulation and traction force on the proximal radius contribute to the Monteggia lesion. [15]. Another study on 6 cadavers confirms the pivotal role of ulnar angulation as a basis for radial head subluxation. Sandman et al introduce a concept of proximal ulna dorsal angulation, which is a normal sagital bow in the proximal ulna. The extent and direction of malalignment of this angulation, along with the annular ligament tear determines the magnitude of radio capitellar instability. [16]. But an exact biomechanical explanation of the our reported injury was not available.
In our case there was not only a fracture of the proximal ulna but also a dislocation of the ulnohumeral joint. We hence theorize that this was made possible due to either of the two mechanisms.
Ulna fracture and ulnohumeral dislocation happened sequentially: The boy landed on the outstretched arm with elbow in neutral rotation and slight flexion. The force impacted distal to proximal with force concentration in the proximal ulna causing a fracture. After the fracture of proximal ulna, the boy further landed on the proximal forearm thereby causing a direct force on the already fractured proximal ulna. This resulted into a posterior dislocation of the ulnohumeral articulation. Ulna fracture and Ulnohumeral dislocation happened simultaneously: This injury may have occurred due to a fall on the outstretched hand with the elbow in flexion. The combination of normal ulnar bowing and flexion in the elbow at the time of impact, created a force couple with vector transmission in two directions. One directed axially and proximally causing the ulnohumeral dislocation and second directed dorsally and outward, causing the proximal ulna fracture with apex posterior angulation.
Concomitant ulnohumeral dislocation with posterior monteggia fracture is a very rare pattern of injury. There is a case series of a similar fracture pattern described in adults. This series has relatively high energy mechanisms with multifragmented fractures. [17] Our case report is quite unique as we have not identified similar injury reported in adolescents. We recommend this injury pattern to be included as a type 2 variant. We also recommend that all type 2 monteggia fractures in children should be assessed for ulnohumeral instability at the time of fixation/manipulation of the proximal ulna fracture.
Footnotes
Conflicts of interest
The author has no conflicts of interest relevant to this article.