
Abstract

How significant is infectious CNS disease?
Neurological disease is common in cats — accounting, for example, for approximately 10% of cases in two separate UK-based feline medicine referral clinics. 1,2 There are many different causes of central nervous system (CNS) disease in cats (see box, page 825) and about 30–45% of cases are believed to be infectious in origin. 1,3 However, a specific infectious agent cannot be identified in up to 40% of these cases; which holds true when looking at either clinical cases 4 –6 or histopathological data (Table 1). 1,3 Most of these cases are found to have histopathological changes suggestive of viral infection that is not consistent with feline infectious peritonitis (FIP) (so-called viral non-FIP encephalitides), but no causal agent can be identified. 1 –3 This group becomes even more significant if cats with particular clinical signs are considered. For example, of 30 cats investigated for recurrent seizures, all were found to have structural brain disease and 14 (47%) had non-suppurative meningoencephalitis, suggestive of a viral infection, but no infectious agent could be identified. 5
FIP and viral non-FIP encephalitides (ie, non-suppurative [meningo]encephalitides of unknown, although probable viral, cause) are the two most commonly recognised (confirmed or probable) infectious CNS disorders of cats. Toxoplasmosis is the third most commonly identified cause, while other infections such as bacterial infections, feline immunodeficiency virus (FIV), feline leukaemia virus (FeLV), feline panleukopenia virus (FPV), and fungal and parasitic infections only rarely manifest primarily as neurological conditions.
Diagnoses in 92 feline neurological cases found to have CNS histopathology consistent with inflammation and/or infection 1
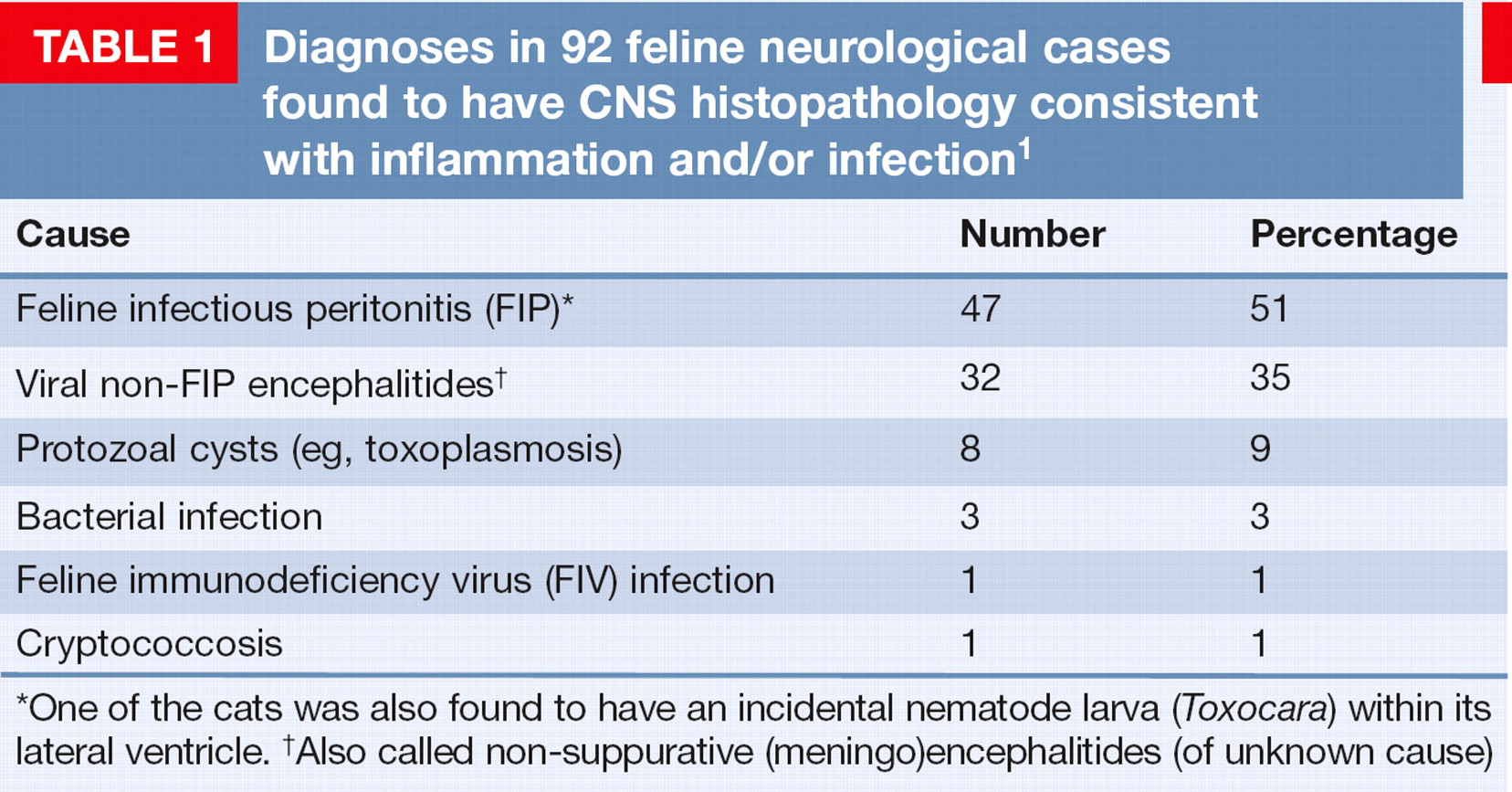
One of the cats was also found to have an incidental nematode larva (Toxocara) within its lateral ventricle.
Also called non-suppurative (meningo)encephalitides (of unknown cause)
Naturally occurring infectious causes of CNS disease in domestic cats

Diagnostic work-up
The complete diagnostic work-up comprises a careful history and clinical examination, ophthalmic, otoscopic and neurological examinations, haematology, serum biochemistry, tests for specific infectious agents, advanced imaging (magnetic resonance imaging [MRI] or computed tomography [CT]) and cerebrospinal fluid (CSF) analysis (Tables 2 and 3). 7,8 Unfortunately, the lack of pathognomonic clinical signs and the limited availability of many diagnostic tests, including CT/MRI and tests to detect specific infectious agents (see box, page 827), means that it is impossible to confirm the cause in many cases of infectious CNS disease.
Signalment and history
As with all clinical investigations, the cat's age, gender, breed and history may help to suggest a diagnosis. For example, cerebellar hypoplasia secondary to in utero FPV infection is seen in young kittens; FIP is seen most commonly in pedigree cats of under 4 years of age that have often come from a large breeding colony; viral non-FIP encephalitides occur most commonly in young to middle-aged cats; toxoplasmosis is seen most commonly in adult cats that hunt (although it can also be seen as a congenital infection in young cats); FIV and FeLV are seen most commonly in older cats that fight; and a cat that is known to have had a chronic suppurative middle ear infection may suffer from its extension into the CNS. In practical terms, however, as most infectious CNS disease is seen in young adult cats, their age may not be that helpful in differentiating this group. 7
Clinical signs
Most infectious causes of CNS disease result in neurological signs that are acute in onset and progressive, with some cases becoming chronic. There may be a history of past or present systemic disease, particularly in the case of FIP or toxoplasmosis. The clinical signs of meningoencephalitis may help to reflect the location of the lesion. Clinical signs are usually, but not always, symmetrical, and while FIP and toxoplasmosis tend to cause signs of multifocal CNS involvement, some cats with viral non-FIP encephalitides may have focal disease. 3 Few of the infectious agents give rise to specific findings, although in the case of Aujeszky's disease REVIEW / Infectious causes of CNS disease virus (pseudorabies) there is always a history of exposure to pigs from an endemic area, and affected cats usually show intense facial pruritus.
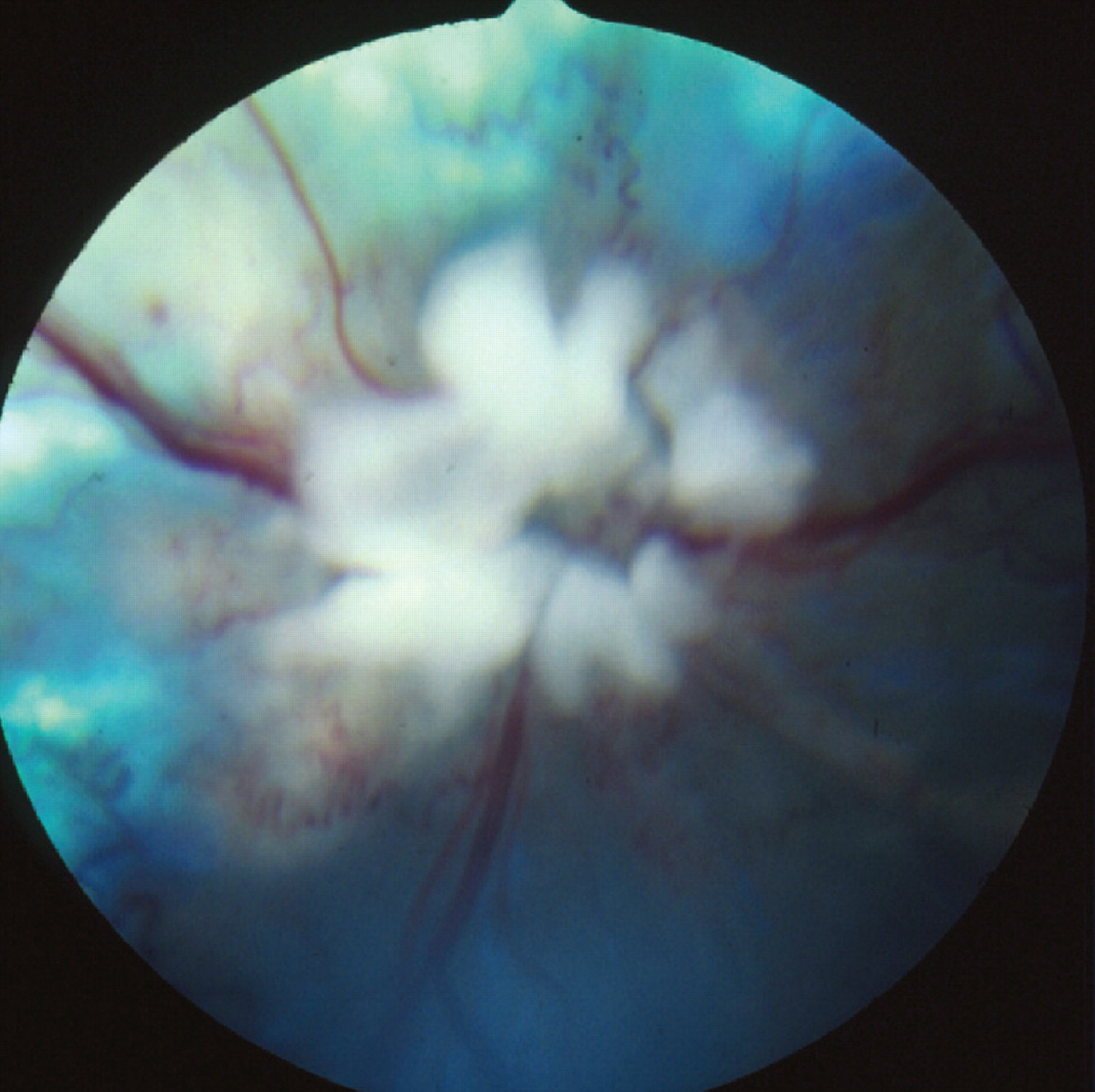
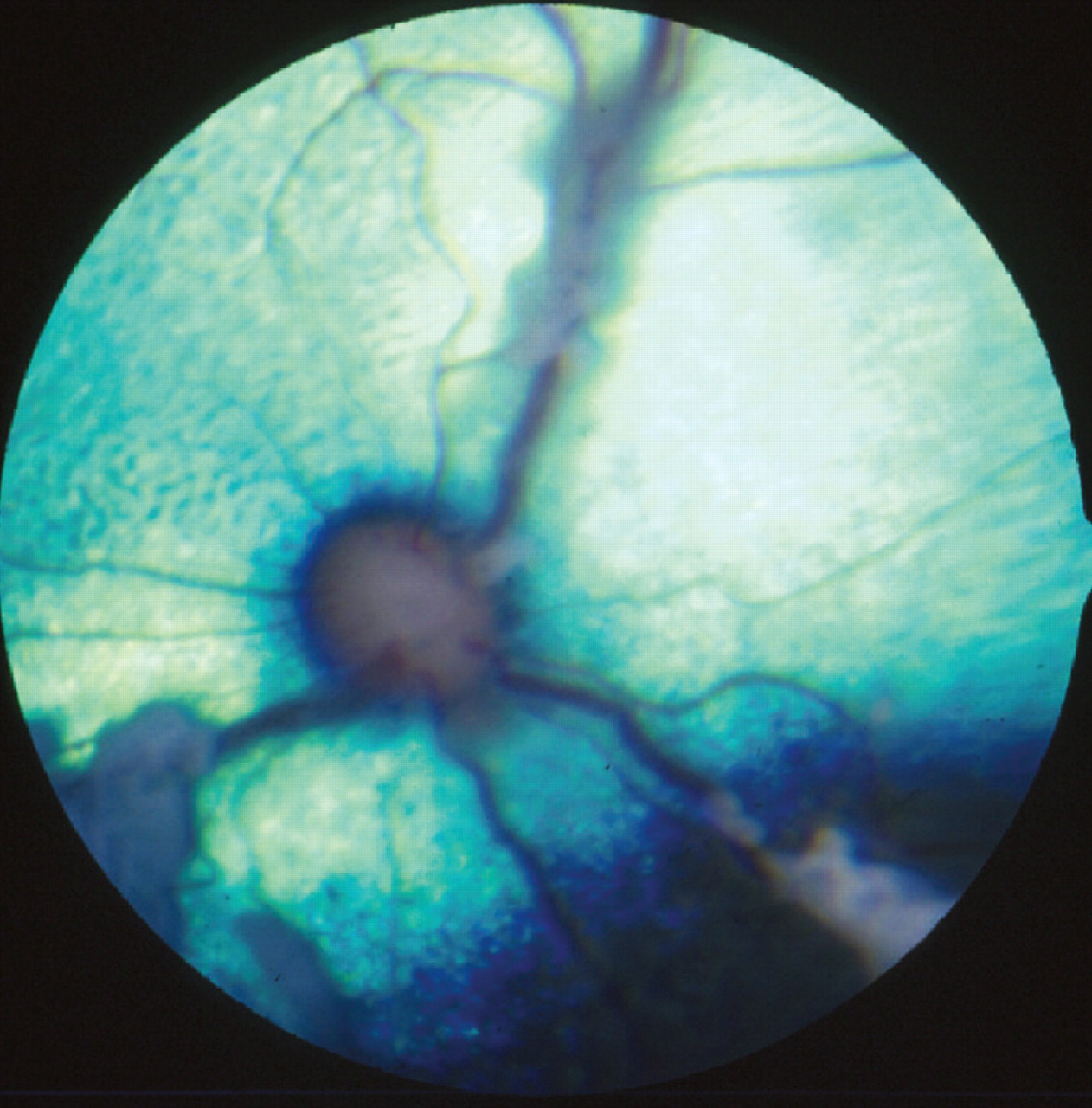
A detailed clinical examination is essential. With toxoplasmosis, FIP, FeLV and FIV, there are usually concurrent systemic signs, and cryptococcosis usually starts with upper respiratory tract signs. Local or systemic lymphadenopathy may also be present. In cats with neurological FIP, abdominal examination often reveals mesenteric lymphadenopathy, and/or irregular kidneys, liver or spleen. 9 A full ocular examination is imperative in all cases and the nature of the changes seen can often help in suggesting which infection is most likely. Inflammatory CNS disease can be associated with uveitis, and fundoscopic examination may reveal papilloedema, optic neuritis, chorioretinitis, and/or retinal haemorrhages (Figs 1—3). Otoscopic examination is needed to look for possible infectious ear disease that could have extended into the CNS. Neurological examination is essential to localise the area of CNS dysfunction, and has been well described elsewhere, 10,11 albeit is not always easy to perform in cats.
Retina of a cat with FeLV infection, showing lymphomatous infiltration of the optic disc. Courtesy of Sheila Crispin

Granulomatous tissue in the anterior chamber of an eye associated with Mycobacterium microti infection. Courtesy of Philip Hanlon

Mycobacterial granulomatous chorioretinitis. Courtesy of David Gould
Information that may be useful in the diagnosis of infectious causes of CNS disease in cats

Infectious diseases of the feline CNS with typical CSF changes
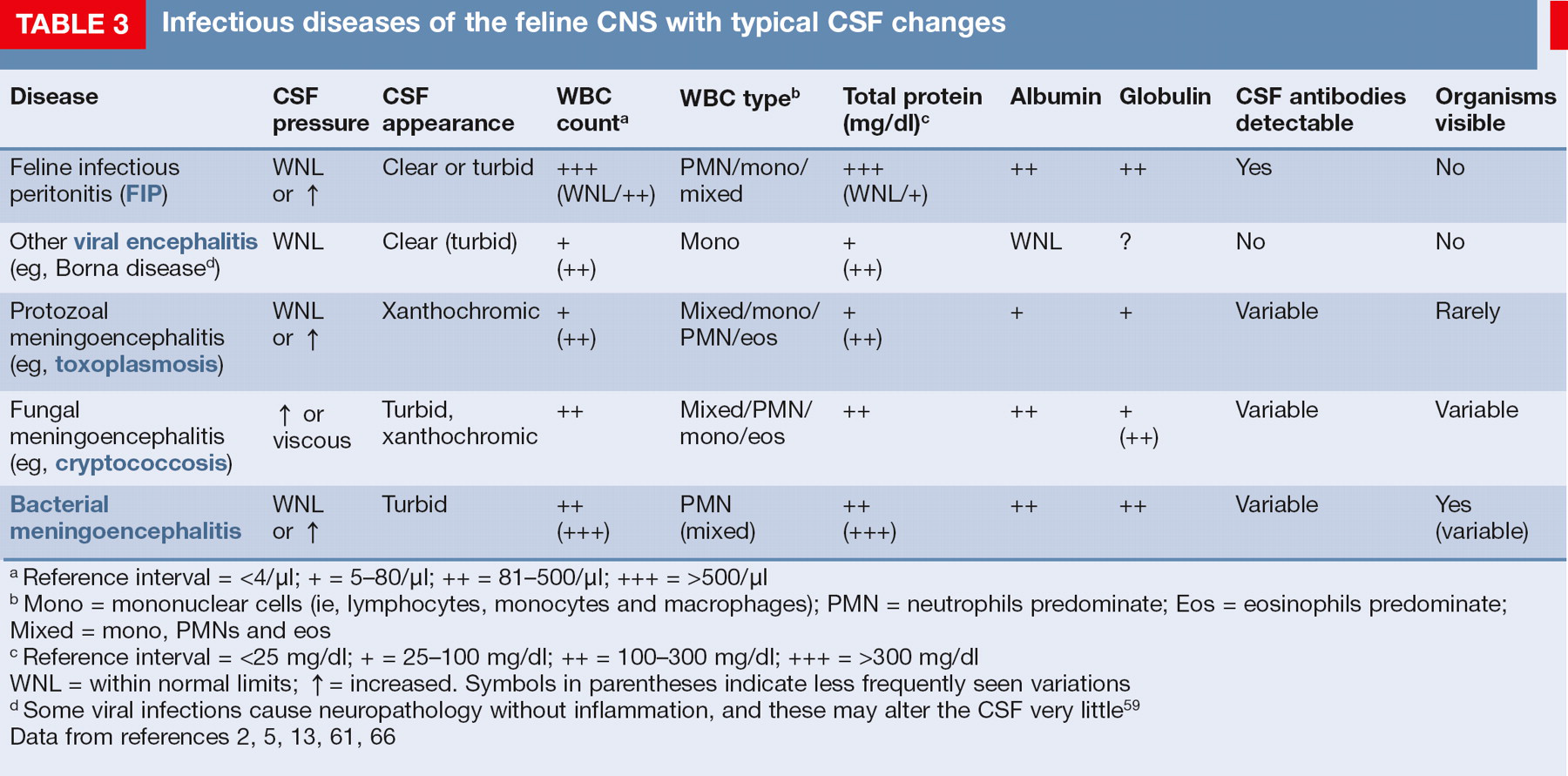
Reference interval = <4/μl; + = 5–80/μl; ++ = 81–500/μl; +++ = >500/μl
Mono = mononuclear cells (ie, lymphocytes, monocytes and macrophages); PMN = neutrophils predominate; Eos = eosinophils predominate; Mixed = mono, PMNs and eos
Reference interval = <25 mg/dl; + = 25–100 mg/dl; ++ = 100–300 mg/dl; +++ = >300 mg/dl
WNL = within normal limits; = increased. Symbols in parentheses indicate less frequently seen variations
Some viral infections cause neuropathology without inflammation, and these may alter the CSF very little 59
Data from references 2, 5, 13, 61, 66
Diagnostic tests
Biochemistry and haematology
Serum biochemistry and routine haematology may help in the diagnosis of toxoplasmosis, FIP, FeLV and FIV, but none of the changes are specific for any of these infections. All four infections can cause non-regenerative anaemia, increased numbers of neutrophils and/or monocytes, and increased serum globulins. While viral infections tend to result in lymphopenia, toxoplasmosis more commonly causes lymphocytosis. Other haematological and serum biochemical changes will vary depending on the extent of systemic involvement. When systemic changes are detected they should be investigated further. Haematology and serum biochemistry are rarely rewarding in cases of viral non-FIP encephalitides or CNS lymphoma. 7
Advanced imaging
For diseases confined to the CNS, MRI/CT (and CSF analysis — see below) are needed to enable diagnosis. MRI is considered superior to CT in the investigation of most cases of neurological disease in cats. 7 Potential MRI changes are mentioned in each of the relevant sections of the text, and discussed in detail elsewhere. 12 Unfortunately, these changes are rarely pathognomonic for a specific type of infection.
CSF analysis
CSF analysis may be non-specific, but it can be helpful in some cases (Table 3). Methods of performing this procedure have been well described elsewhere. 8,13 Standard tests performed on CSF include assessment of its gross physical appearance (colour, turbidity), quantitative analysis (red blood cell count, total nucleated cell count, protein concentration), and cytological analysis (leukocyte distribution and characterisation, in addition to the presence of other cells or infectious agents). CSF can also be assessed by further biochemical tests, microbiology (aerobic, anaerobic and fungal culture), and serological or polymerase chain reaction (PCR) testing for specific infections (see below). Unfortunately, a spinal tap is not without possible hazard as the presence of inflammatory CNS disease increases the risk of raised intracranial pressure, and thus of brain herniation. For this reason, where possible, it is best to perform MRI prior to CSF collection to try to evaluate this risk.
Serology and PCR
Before diagnosing an infectious cause of CNS disease it is necessary to identify that the cat has been infected with a specific infectious agent. Unfortunately, while tests may show that a cat is, or has previously been, infected with a particular agent, this does not necessarily mean that the infection is the cause of the current CNS signs. Antibody, antigen and/or PCR tests are readily available for a number of infectious agents in cats, including FeLV (antigen/PCR), FIV (anti-body/PCR), FIP (antibody/PCR), Toxoplasma species (IgG and IgM titres) and Cryptococcus species (latex cryptococcal antigen test). Although antibody titres reflect direct exposure to the organism, a positive titre does not confirm active infection. An elevated IgM titre reflects acute infection, whereas an elevated IgG titre may be indicative of chronic infection or previous exposure to a pathogen.
CSF antibody titres are thought to be more reliable than serum titres for diagnosing infectious disease within the CNS. To distinguish true intrathecal antibody production from contamination of the CSF with antibodies from the peripheral blood that may be present in the event of a compromised blood—brain barrier, the CSF IgG quotient (or IgG index) can be calculated; this provides a comparison between the concentrations of a specific antibody in the CSF and the same antibody in the serum. 6,14 Looking for evidence of infection within the CNS may be more helpful — for example, performing PCR assays to detect DNA or RNA from an infectious organism within the CSF. However, it should be noted that such tests may be insensitive because they require the presence of the organism in the biological sample under evaluation. Therefore, a negative PCR result does not definitively rule out active infection. Ultimately, a post-mortem examination may be required, often with PCR testing or immunohistochemical staining of sections, to confirm the presence of specific infectious agents.
Feline infectious peritonitis
FIP occurs following infection with a feline coronavirus (FCoV). In up to 10% of cats infected with FCoV, host and viral interactions allow the virus to replicate within macrophages, ultimately resulting in systemic disease manifesting as an immune-mediated vasculitis; this has been reviewed elsewhere. 15 –17
FIP is a common cause of neurological disease in cats, and the most commonly detected infectious cause. It accounts for 45–50% of all cases associated with histopathologically identified inflammatory changes, 1 which equates to 15–20% of all cases of feline neurological disease. 1,5 In young cats (less than 2 years old), it is also the most common histopathologically confirmed cause of spinal cord disease, affecting 24% (28/84) of cases. 18 It is important to realise just how common this infection is; and that, while most clinical cases are seen in young pedigree cats with obvious systemic involvement, this is not invariably the case. 15
Clinical signs of FIP may be vague, such as weight loss, anorexia or fever. The more frequent, effusive form causes systemic disease secondary to an exuberant humoral immune response, characterised by a fibrinous peritonitis and pleuritis. Affected cats may display abdominal, pleural or pericardial effusion. Neurological involvement (see below) is more common with the non-effusive (or ‘dry’) form of the disease and develops in cats with humoral immunity, but only partial cell-mediated immunity. 9,19,20 Ocular signs are common with neurological FIP, and typically comprise anterior uveitis (often with keratic precipitates), chorioretinitis, anisocoria, and retinal haemorrhage and/or detachment (Figs 4 and 5). 9,15,22

Anterior chamber haemorrhage and inflammation with marked iris vasculitis in a cat with FIP. Courtesy of Sheila Crispin
Retina showing perivascular cuffing due to FIP. Courtesy of Sheila Crispin
Neurological signs associated with FIP
Neurological signs are not pathognomonic for FIP. They are usually multifocal but occasionally appear to result from focal disease. They include altered mentation, ataxia, cranial nerve abnormalities, tetraparesis, central vestibular signs, hyperaesthesia and seizures. Seizures have been reported to occur in approximately 25% of cases of neurological FIP, and may be considered a poor prognostic sign, associated with extension of the disease to the forebrain. 21 Generalised seizures and complex focal seizures were reported to affect 64% and 28% of cases, respectively. 21
Diagnosis
Diagnosis of FIP is complex and challenging, with the gold standard being immunofluorescence or immunohistochemistry to detect FCoV antigen within macrophages in body fluids or tissue sections. 15
In practice, antemortem diagnosis is often made based on the combination of signalment (most cases occur in pedigree or rescue cats from multi-cat households that are less than 4 years of age), history (typically of a recent stressful event such as rehoming or neutering), clinical signs, albumin/globulin ratio, FCoV titre, alpha-1 acid glycoprotein level, plus or minus a positive Rivalta's test if ascitic fluid is present. CSF analysis may reveal a predominantly neutrophilic or mixed cell pleocytosis, but can be normal. CSF total protein concentration is often markedly elevated (>200 mg/dl) (Table 3). 3,19,23
Serum tests for FCoV titre are often positive but have a low specificity. Furthermore, a negative serum titre does not exclude the possibility of FIP-associated neurological disease because soluble antibodies can form immune complexes and escape detection by standard tests. There is also considerable overlap in titres in cats with and without FIP (ie, some cats with FIP have low titres, while many cats with high titres never develop FIP). Measurement of FCoV antibodies in CSF has also yielded conflicting results, 9,24 and the value of PCR on CSF has not been fully evaluated. Unfortunately, it is not uncommon for CSF to fail to flow on a spinal tap, due to increased viscosity relating to markedly elevated protein concentrations.
Cats with FIP may show no abnormalities on MRI, but, where abnormalities are detected, meningeal and ependymal lining contrast enhancement, granuloma formation and obstructive hydrocephalus (most commonly due to blockage of the fourth ventricle and subarachnoid space at the level of the foramen magnum) are commonly reported (Fig 6). 9,25
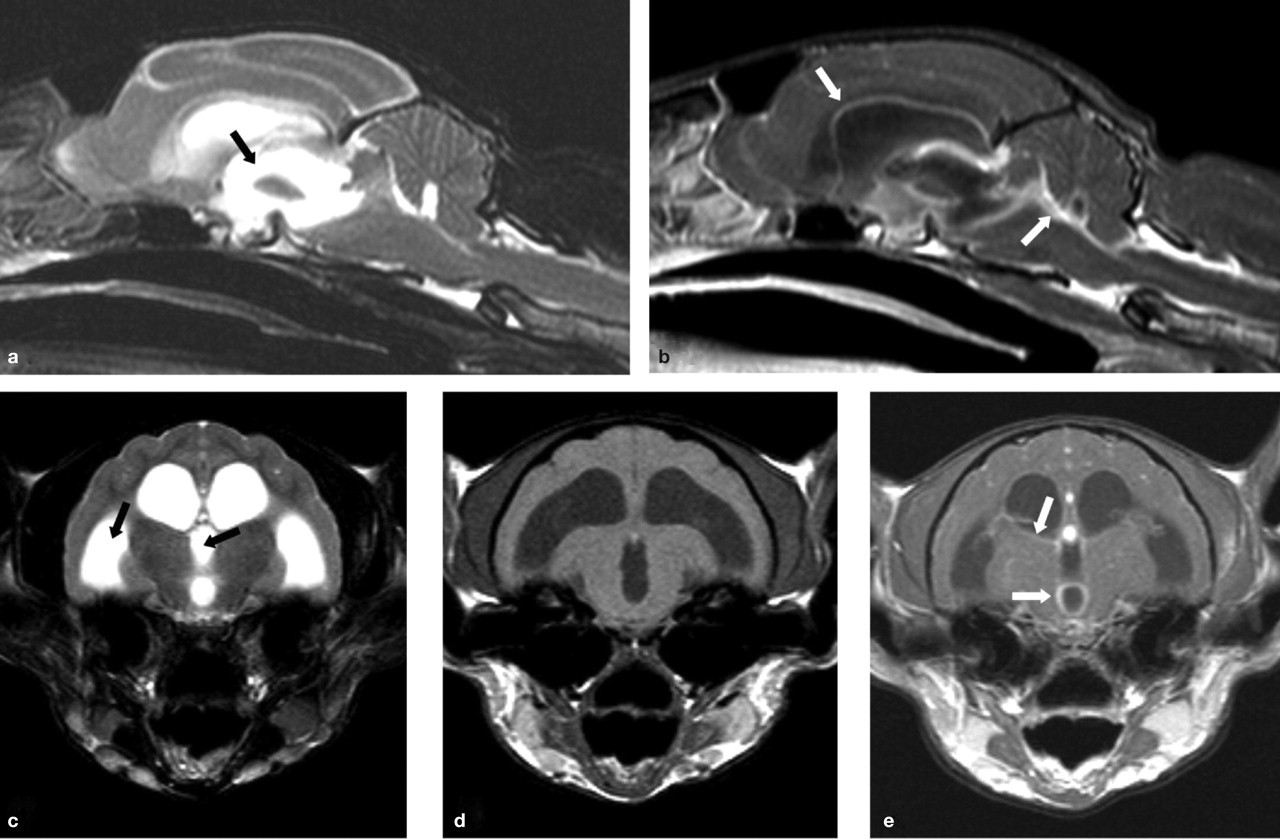
MRI scans from a cat with neurological FIP. T2-weighted midline sagittal (a) and transverse (c) images reveal obstructive hydrocephalus of the third and lateral ventricles (black arrows). T1-weighted post-contrast sagittal (b), and pre- and post-contrast transverse (d and e, respectively) images of this same region reveal enhancement around the third and lateral ventricles (white arrows) following administration of an intravenous contrast agent (gadolinium). These features are indicative of FIP in which a pyogranulomatous inflammation is seen on the surface of the brain involving the meninges. Courtesy of Mark Lowrie, Davies Veterinary Specialists
Post-mortem examination is often required for confirmation of the diagnosis, with demonstration of the presence of FCoV antigen or identification of viral genetic material using a FCoV-specific PCR assay in inflamed tissues. As with many viral infections affecting the CNS, histopathology reveals nonsuppurative meningoencephalomyelitis, with perivascular cuffing and meningeal infiltration with mononuclear cells, gliosis and variable neuronal degeneration. However, the inflammation is often pyogranulomatous, and located around the lateral ventricles, in the meninges, or affects the choroid plexus. 1,9 Ependymitis and choroiditis may also be a feature, affecting the fourth ventricle more than the lateral ventricles, and giving rise to a secondary hydrocephalus that may be detected by MRI.
Treatment and prognosis
Although various therapeutic modalities have been proposed for the treatment of FIP, at present this remains an invariably fatal disease.
Toxoplasmosis
Cats are the definitive host for Toxoplasma gondii, which is an intracellular coccidian parasite. Infection is usually the result of ingestion of prey harbouring bradyzoites, but faeces containing oocysts are another potential source of infection. Clinical reviews of feline toxoplasmosis are available. 14,17
Toxoplasmosis is typically a multisystemic disease, which may either be acute or chronic. Acute disseminated disease arises due to rapid replication of tachyzoites, often within the liver, CNS, pancreas or lungs. Chronic disease is more typically associated with vague signs, such as fever, anorexia, weight loss and diarrhoea. Dissemination of chronic disease may occur in patients that become immunosuppressed (eg, following administration of ciclosporin or infection with feline retroviruses). 26 CNS disease is most commonly seen following reactivation of latent bradyzoites within the brain, spinal cord and/or skeletal muscles. This often manifests as neurological (and ocular) signs in the absence of systemic disease. Again, this may be a sequela of immunosuppression associated with chemotherapy and/or retroviral infection.
Toxoplasmosis is the second most common definitively diagnosed infectious disease of the feline CNS. 1,23,25 Although neurological involvement is histologically present in nearly all cats with toxoplasmosis, 27 clinical signs relating to the CNS are only apparent in approximately 10% of cases. 26 Neurological signs (see right) may be seen alone or in conjunction with systemic signs such as pneumonia or diarrhoea. Concurrent clinical signs may also include lymphadenopathy, pancreatitis, hepatitis, myocardial disease and/or myositis. Ocular examination may reveal chorioretinitis and/or uveitis.
Neurological signs associated with toxoplasmosis
Neurological signs are usually multifocal and include behavioural changes, altered mentation, seizures, ataxia, blindness, anisocoria, torticollis, vestibular signs, muscle hyper aesthesia and paresis/paralysis. 17,28
Diagnosis
Diagnosis of toxoplasmosis is challenging. It commonly relies on assessing antibody titres as changes in routine haematology (typically increased neutrophils, lymphocytes and monocytes) and serum biochemistry (eg, azotaemia, changes consistent with hepatopathy, increased globulins) are not specific and depend on the extent of systemic involvement.
IgM titres are an indicator of recent or active infection. Unfortunately, false-negative results (IgM <1/64) may be seen in cats that have been infected for a sufficient length of time for the IgM to undergo a class switch to IgG. They can also arise where extremely high levels of antibody cause a so-called prozone effect (where false-negative or false-low results occur from excess antigen or antibody in a sample due to inability of the analyte to bind to receptor sites). Conversely, false-positive results may be seen in chronic infections with persistent elevation of IgM. 14 Significantly elevated IgG titres may only represent previous exposure; a fourfold rise in titre over a 2–4 week period is more useful in demonstrating recent or active infection.
Routine CSF analysis is non-specific, typically revealing mild increases in lymphocytes (and occasionally neutrophils), with elevated protein concentrations (Table 3). Detection of T gondii IgG or DNA in the CSF may be more supportive of active infection. However, both IgG and DNA have been detected in the CSF (and aqueous humour) of normal as well as clinically ill cats. T gondii-specific IgM antibodies in the CSF may prove to be diagnostic, as unpublished data 26 has suggested that this class of antibody has not been detected in the CSF of healthy cats. Additionally, immunohistochemistry and PCR can also be performed on tissue samples. The rare presence of tachyzoites in the CSF is also diagnostic.
In patients with neurological signs, MRI findings are non-specific and often reflect multifocal involvement; lesions may have indistinct margins. 25 However, solitary space-occupying lesions attributed to granulomas have also been reported, 29,30 which may make differentiation of toxoplasmosis from neoplasia (eg, meningioma or lymphoma) more difficult. 30
Histopathology typically reveals inflammation and necrosis. Demonstration of protozoal tissue cysts is strongly supportive of a diagnosis, but immunohistochemistry or PCR assay may be required to definitively prove these are due to T gondii.
Treatment of toxoplasmosis
Clindamycin (10–12 mg/kg PO, IM or IV q12h) is the treatment of choice for toxoplasmosis. 14,17 However, trimethoprim sulphonamide (15 mg/kg PO q12h) plus a folic acid supplement (0.5–1.0 mg/cat PO q24h) may also be beneficial. Azithromycin (5 mg/kg PO q12h) may be more effective at entering the CNS in some cases, although in some cats toxoplasmosis may be refractory to this drug.
Some authors recommend that low anti-inflammatory doses of corticosteroids be given at the same time as starting antibiotic therapy, as the death of the organisms can trigger more extensive CNS inflammation. While there are no studies investigating this in cats with toxoplasmosis, positive effects have been documented in humans with bacterial, tuberculous and herpes simplex encephalitis. 31
CNS signs of toxoplasmosis may take longer than other clinical signs to improve. 26
Therapy should be continued for at least 4 weeks, and is unlikely to result in complete elimination of the organism, so owners should be warned of the potential for relapse.
Cryptococcosis
Cryptococcal infections are attributed primarily to Cryptococcus neoformans, although Cryptococcus gattii may be involved in some cases. These saprophytic yeasts are typically found in soil and pigeon faeces, and infection is thought to be by inhalation. 32 In people, the infection appears to spread from the lungs to the CNS by the haematogenous route. 32 While spread via this route may also occur in cats, neurological involvement more typically arises as a result of extension from rhinitis.
Although cryptococcosis is the most common mycotic infection of cats, it is a relatively rare cause of inflammatory CNS disease, with neurological signs occurring in only 1% of cases in a UK study, 1 and 6% of cases in an Australian study. 23 Clinical signs associated with cryptococcal infection of the CNS are highlighted below. Neuroanatomical localisation may indicate focal, multifocal or diffuse disease. Concurrent systemic clinical signs usually include nasal/upper respiratory signs, and/or cutaneous disease most commonly affecting the face.
Diagnosis
Culture of Cryptococcus is required for definitive diagnosis, although finding the encapsulated yeast forms in cytological preparations (urine, nasal discharge, lymph node aspirates or cutaneous masses) is strongly suggestive. Serological tests (latex agglutination or ELISA) may be performed to identify cryptococcal capsular antigen. Although cytology, culture and antigen testing may be performed on CSF, the risks of herniation associated with increased intracranial pressure should be considered. Routine CSF analysis may reveal increased numbers of neutrophils, eosinophils and/or mononuclear cells, plus an increased protein concentration (Table 3). The encapsulated organism can be seen in cytological preparations in the majority of cases, especially if using India ink, new methylene blue or Gram stain.
Neurological signs associated with cryptococcosis
Neurological signs include altered mentation and behaviour, seizures, ataxia, circling, head pressing, vestibular signs, cranial nerve abnormalities, generalised tremors, postural reaction deficits, spinal pain and paresis, dilated unresponsive pupils, chorioretinitis and optic neuritis. 32 –36
MRI in cats with cryptococcosis tends to produce very variable findings, including normal scans, multifocal lesions and solitary lesions. 35 Non-contrast enhancing T2-weighted hyperintense lesions (which had low intensity on T1-weighted images) are compatible with gelatinous pseudocysts. Meningeal enhancement is also a frequent finding, consistent with meningitis. Damage to the cribriform plate, retrobulbar disease extension and cerebellar herniation are also reported.
Pathology is compatible with meningitis or meningoencephalitis, with or without pseudocyst formation (Fig 7). The cerebellum and cerebellothalamic region were consistently involved in one study, with the pons, medulla and mid-brain being frequently involved. 35 Cryptococcal granulomas (cryptococcomas) may form in association with a competent cell-mediated immune response. 37

Serial sections through a cat's brain, revealing numerous cryptococcal lesions (arrows). Courtesy of Richard Malik
Prognosis
Median survival time (MST) after diagnosis in one study was only 13 days (range 0–4050 days), with many cats deteriorating rapidly after diagnosis. For those cats that survived more than 3 days after diagnosis, prolonged survival times occurred in some patients. 35 Cats that had altered mentation on presentation had a poorer prognosis, and cats receiving combination therapy survived longer than those receiving single agent treatment.
Treatment of cryptococcosis
Treatment of cryptococcosis involving the CNS is optimised by using a combination of amphotericin B and flucytosine. 38 Amphotericin B can be administered intravenously as a continuous infusion (0.5 mg/kg q24h) or subcutaneously (0.5–0.8 mg/kg 2–3 times weekly). Flucytosine is given concurrently (250 mg q6–8 h PO). Treatment is required for a minimum of 6 weeks (often 12 weeks) or until the antigen titre declines to zero.
Amphotericin B is nephrotoxic so the development of azotaemia may require suspension of treatment to allow the renal damage to resolve. During suspension of amphotericin B/flucytosine therapy, the fungistatic drugs fluconazole or itraconazole may be used as an alternative. Although a beneficial effect of giving a short course of glucocorticoids at the same time as starting antifungal treatment has been demonstrated in one study, 35 their use is controversial.
Feline retroviral infections
Feline retroviral (FeLV and FIV) infections may have a permissive role in CNS disease by enabling establishment of infections such as FIP, toxoplasmosis and cryptococcosis. 39 –41 In addition, the second most common intracranial neoplasm in cats is lymphoma, which is often associated with FeLV infection. In one study, 18% of cats with intracranial lymphoma were positive for FeLV antigen. 42 Lymphoma is also the most common spinal neoplasm of cats (39% of spinal neoplasms), with many affected individuals being young and FeLV-infected, presenting with spinal pain and paresis/paralysis. 43 Chronic FeLV infection (of greater than 2 years' duration) has been reported to be associated with a chronic myelopathy that may manifest as urinary incontinence, hyperaesthesia, ataxia and paresis progressing to paralysis. 44 Histologically, white matter degeneration was detected diffusely within the spinal cord.
FIV is a neurotropic virus. Up to 20% of experimentally infected cats may develop significant neurological deficits; however, most pet cats are euthanased before these become obvious so CNS changes are only reported in 1–5% of naturally occurring cases. 45 Diagnosis may be hampered as several cases of FIV-induced neurological disease have been serum antibody negative; 46 in one report approximately 20% of cats naturally infected with FIV were antibody negative. 47 It may, therefore, be necessary to perform PCR on blood or CSF to detect the infection, or immunohistochemistry on brain sections collected post mortem. Perivascular inflammatory infiltrate and glial nodules are typical histopathological findings. 45,48
Bacterial meningoencephalitis
Bacterial, typically suppurative, meningoencephalitis may develop as a result of extension of bacterial disease — most commonly from middle ear infection or rhinitis, penetrating injury to the skull or haematogenous spread from distant sites of infection (eg, myocarditis). A wide variety of organisms may be involved, the most common being Staphylococcus species. Bacterial infection of the CNS may result in an abscess and/or, much less frequently, a collection of pus (empyema) in subdural or epidural locations. Brain abscesses are life-threatening due to systemic and local toxicity (in the early stages of cerebritis) and increased intracranial pressure (during/after capsule formation).
Clinical signs, which are largely the result of the inflammatory reaction that the bacteria provoke, are very variable (see left), and usually rapidly progressive and frequently fatal if left untreated. 8,13
Neurological signs associated with FIV infection
Typical signs include behavioural changes (decreased interaction with owners or aggression), anisocoria (Fig 8), altered sleep patterns and paresis. 45 (Note that most pet cats are euthanased before significant neurological deficits become apparent.)

Three-year-old cat with FIV and static anisocoria (‘static pupil syndrome’). Courtesy of Sheila Crispin
Neurological signs associated with bacterial meningoencephalitis
Affected animals can present with a wide variety of neurological signs of intracranial disease that reflect a focal anatomic diagnosis, suggesting a space-occupying lesion, or a multifocal syndrome associated with many small microabscesses.
Treatment of bacterial meningoencephalitis
Treatment involves antibacterial drugs, ideally selected according to CSF culture and sensitivity testing. It is best to select bactericidal drugs that cross the blood—brain barrier and achieve high CSF concentrations. 13
Prior to the culture results being known, potentiated sulphonamides are a good choice. 8 With inflammation, some drugs that would not normally gain good brain penetration can cross the blood—brain barrier (eg, clindamycin). More information about specific antibiotic choices is reviewed by Kent. 13
Antibiotic treatment should initially be given intravenously for 3–5 days, and then continued orally until at least 2 weeks beyond clinical resolution. Dying bacteria can trigger an increased inflammatory response so a number of authors recommend a short course of corticosteroids be given at anti-inflammatory doses, starting just before the antibiotics (eg, dexamethasone for 4 days). 8,13,31 Surgical decompression by craniectomy is indicated in cases of brain abscessation that do not respond to medical management. Adjunct therapy may also include analgesia, anticonvulsants and supportive care (eg, intravenous fluids).
Even in people, the mortality rate for bacterial meningoencephalitis is up to 40%, with many of the survivors having permanent neurological deficits.
Diagnosis is based on blood and/or CSF culture but false-negative results can occur and the risk of brain herniation following CSF collection is considerable. Gram staining of CSF can be helpful. Routine haematology may show neutrophilia with a left shift, but changes in haematology and serum biochemistry are not always present and are non-specific. CSF cell counts are usually markedly increased, with toxic neutrophils and intracellular bacteria (Table 3). CT or MRI may be useful to reveal the extent of disease and whether or not there is abscessation (Fig 9). 8 Histopathology plus special staining (eg, Gram or Ziehl-Neelsen) may reveal bacteria (Fig 10).

T1-weighted post-contrast transverse magnetic resonance image of the brain at the level of the tympanic bullae from a cat with otitis media/interna and secondary meningoencephalitis. Courtesy of Cristian Falzone, Davies Veterinary Specialists

Ziehl-Neelsen-stained histopathological preparation of the brain of a cat with Mycobacterium avium infection, showing inflammation and cells packed with positive-staining bacteria
Other infectious causes of neurological disease in cats
Rabies
The risk of rabies infection out with endemic countries is rare. Cats may also become infected with bat Lyssavirus, but the risk of infection is considered to be extremely low. Rabies infection in cats most typically presents as the furious form and the disease has been reviewed recently in this journal in the context of the ABCD guidelines. 49
Borna disease virus
Borna disease virus (BDV) (reviewed by Gunn-Moore, and Kamhieh and Flower), 2,50 appears to cause a sporadic, progressive polioencephalomalacia, sometimes known as ‘staggering disease’. Serological surveys and surveys looking for BDV RNA within peripheral blood samples show that BDV infection is globally distributed in many different animal (including bird) species and infection is usually asymptomatic. Non-symptomatic cats from northern and central Europe are commonly seropositive, as were 6% of cats in the UK51 and 13–22% of cats in Japan. 52,53 The prevalence of seropositivity increases steadily with the age of the cat 54,55 and appears to be higher in cats that are also retrovirus positive. 51,56,57 Antibodies against BDV and/or BDV RNA have been detected most commonly in cats with neurological signs; 13% in Germany, 58 35% in the UK, 51 and 67% in Japan. 59
Clinical signs include pyrexia, hindlimb ataxia, behavioural changes, inability to retract the claws and lumbosacral pain (Fig 11). 60 Histopathologically, BDV may result in nonsuppurative meningoencephalomyelitis, with neuronophagia, microgliosis and heavy perivascular cuffing by mononuclear cells (Figs 12 and 13). 54,61 Diagnosis is challenging due to lack of readily available tests, and the difficulty of discerning the significance of positive test results, as they may also be found in clinically normal animals. 2,62

Two-year-old cat with Borna disease virus infection; she was ataxic and unable to retract her claws. Courtesy of Anna-Lena Berg

Histopathology of the brain of a cat with BDV, showing inflammation and vacuolation (resulting from neuronal loss). H&E staining. Courtesy of Anna-Lena Berg

Immunohistochemistry (IgG) of the brain of a cat with BDV, showing perivascular cuffing. Courtesy of Anna-Lena Berg
Highly pathogenic avian influenza
Although this infection is primarily associated with respiratory signs and pyrexia, cats infected with H1N1 influenza frequently show signs attributable to encephalitis prior to death. The index of suspicion is likely to be increased if the cat has contact with birds in an endemic area. 60
Feline panleukopenia virus (FPV; feline parvovirus)
Cerebellar hypoplasia may result from in utero infection, perinatal infection or vaccination of a pregnant queen with a live FPV vaccine. Affected kittens typically have a wide-based gait with an intention tremor that is apparent as soon as they start exploring as young kittens. This is a non-progressive disorder and there are no associated inflammatory changes within the brain. Other, less commonly seen defects include forebrain lesions (which can result in seizures and/or behavioural changes) and/or retinal damage. These can occur with or without concurrent cerebellar hypoplasia.
Other naturally occurring and clinically significant CNS infections
A variety of organisms have been seen very occasionally as a cause of CNS disease in cats, including Bartonella henselae, which typically causes cat scratch disease in humans, but can also cause CNS disease in cats, 63 Mycoplasma felis, 64 feline herpesvirus (FHV-1), feline calicivirus (FCV), Aujeszky's disease virus, Aspergillus species and dematiaceous fungi (Cladophialophora bantiana), and nemotodes (eg, cuterebral larval migration, Sarcocystis neurona). A number of different arboviruses (the arthropod-borne encephalomyelitis group) have also been shown to infect cats (eg, BDV — see above), St Louis encephalitis virus, Japanese encephalitis virus, Yellow fever virus and Rift Valley fever virus, to name just a few. Many of these viruses have a very wide geographic distribution, including the USA and Europe, and some are endemically present in wild mammal populations to which free-living cats may become exposed. However, while studies show that cats are potentially at risk of becoming infected with these organisms, their role in causing significant naturally arising feline neurological disease remains to be determined (reviewed in Gunn-Moore). 2
Viral non-FIP encephalitides
Many cases of neurological disease in cats fall into the category of viral non-FIP encephalitides. While the cause(s) remain unknown, the nature of the histopathological change is highly suggestive of viral infection. These cases classically fall into two groups based on histopathology (reviewed in Gunn-Moore) 2 : group 1 — with non-suppurative encephalomyelitis, and group 2 — with polioencephalomyelitis or polioencephalitis.
Unfortunately, until the cause(s) of these conditions is understood, specific diagnostic tests are not possible and treatment is symptomatic. Some cats may recover, even though they presented with severe signs and/or cluster seizures. MRI may or may not show multifocal areas of enhancement.
KEY POINTS
Clinically significant neurological disease is common in cats.
Infectious causes of central nervous system disease are believed to account for 30–45% of cases.
The two most commonly recognised causes are feline infectious peritonitis (FIP) and viral non-FIP encephalitides (ie, non-suppurative [meningo]encephalitides of unknown, although probable viral, cause), with toxoplasmosis comprising the third most common infectious cause.
Unfortunately, a specific infectious agent cannot be identified in up to 40% of cases.
Bacterial infections, feline immunodeficiency virus, feline leukaemia virus, feline panleukopenia, and fungal and parasitic infections are seen only rarely as a cause of neurological disease.