
Abstract

TRAUMATIC BRAIN INJURY
The second part of this two-part article, addressing the diagnosis and management of traumatic brain injury, appears on pages 815–823 of this issue of J Feline Med Surg and at: doi:10.1016/j.jfms.2011.09.003
Head Injury in Context
Trauma is common in cats and can result in significant morbidity and mortality. 1 Due to their small size it is common for cats to receive injuries to more than one body system and frequently this will include the head. Literature on this topic, referring specifically to trauma of the head and not including brain injury, is limited in the veterinary field, particularly with reference to cats. This is despite the fact that the head is the second most frequently injured body region in cats (the extremities being the most commonly injured region). 2
Injury to the head commonly includes damage to the soft tissues (including the skin and eyes) and bones of the skull, often in association with some degree of brain injury. Mandibular and maxillary fractures account for 15–23% of all fractures in cats. 3,4 These injuries are usually a result of a road traffic accident or unknown blunt injury, 5 but high-rise syndrome is also commonly associated with head injury. 6,7
Initial assessment
While it is easy to focus attention on the more obvious injuries, it is vitally important that a thorough major body systems assessment is carried out on all trauma patients. Cats should be assessed for abnormalities in their cardiovascular, respiratory and neurological systems, and management for these abnormalities should be initiated prior to completion of the physical examination and before any further diagnostics into their obvious injuries are carried out. Oxygen should be provided to all traumatised cats on initial presentation where their status is unknown.
Cardiovascular assessment
Patients should be assessed for the presence of hypovolaemia through evaluation of heart rate, pulse quality, mucous membrane colour and capillary refill time. This can be challenging as cats seem to compensate well for loss of small volumes of blood but tend to decompensate earlier than dogs with larger fluid losses. Tachycardia with weak pulses, pale mucous membranes and a prolonged capillary refill time (>2 s) should be taken as signs of severe hypovolaemia in a cat and prompt immediate therapy. Note that as the severity of hypoperfusion increases, cats tend to become increasingly bradycardic (rather than tachycardic) and hypothermic, resulting in severe decreases in peripheral perfusion. 8,9 Blood pressure monitoring, if available, is useful. A systolic blood pressure of less than 80–90 mmHg should prompt aggressive and immediate resuscitation in order to maintain adequate cerebral perfusion, 10 particularly in the presence of suspected brain injury.
Respiratory assessment
Facial trauma is frequently associated with trauma to the upper airway, which in some cases can significantly impact on respiratory function. The cat should be assessed for epistaxis and the head and neck gently palpated for emphysema, which may indicate more severe trauma to the nasal bones or trachea. If epistaxis has been severe, gentle attempts to clean the nares may result in easing of respiration. Feline trauma cases will also frequently have sustained injury to the thorax. Respiratory assessment should concentrate on identifying pulmonary contusions or pleural space disease (typically pneumothorax). Diaphragmatic rupture is seen less frequently than pulmonary contusion or pneumothorax, although the effects on the respiratory system can be dramatic.
Neurological assessment
Neurological assessment should initially focus on the mental status of the cat. Severe depression in the presence of normal cardiovascular and respiratory parameters should alert the clinician to the possibility of traumatic brain injury (TBI). Many cats with facial trauma will have a degree of TBI, although this has not been evaluated in the veterinary literature. While in many cases TBI is relatively minor and self-limiting, manifesting as mild, subtle behavioural changes, at the opposite end of the spectrum there can be life-threatening injury and death (often secondary to severe brainstem involvement).
A full neurological assessment should only be conducted in patients that are cardiovascularly stable (see later).
Stabilisation — the priorities
Initial stabilisation should be aimed at maintaining adequate oxygen delivery to all tissues. Prolonged hypoperfusion is associated with organ dysfunction, and increased morbidity and mortality. 11 –13
The two factors that have the most significant impact on the perpetuation of secondary injury (particularly in brain injury) and which should be avoided are hypoxia and hypotension. 10 Thus treatment for these patients revolves around maintaining oxygenation and blood pressure to ensure adequate tissue oxygen delivery. All cats should receive oxygen supplementation initially.
Stabilisation
Fluid resuscitation
Mortality in cases of hypovolaemic shock is related to the duration of the ischaemic insult. 14 Early replacement of circulating volume is key to successful patient management.
Stabilisation of the cardiovascular system centres on replacement of lost circulating volume using intravenous fluid therapy. Fluid resuscitation remains a controversial subject, and it seems that there are many ways to achieve similar end-points. 15 As cats have a small blood volume, even proportionately large volumes of blood loss can be rapidly replaced through the use of isotonic crystalloid fluids (eg, Hartmann's solution).
Hypotonic fluids such as 0.18% saline with 4% glucose, 0.45% saline and 5% dextrose encourage extravasation of water from the vessels into the extravascular space. They are, therefore, inefficient volume expanders and encourage the formation of oedema. The use of these fluids is to be avoided in all forms of hypoperfusion, but particularly when TBI is suspected. 10
The volume of fluid given is based on the severity of hypoperfusion. Aliquots of the ‘shock dose’ (45–60 ml/kg) of isotonic crystalloids are administered over a short period of time (15–20 mins) and the cat is reassessed. The end-point of resuscitation should be normalisation of cardiovascular parameters, heart rate, mucous membrane colour, and capillary refill time and pulse quality. The cat's response to therapy will ultimately determine the total volume to be given. Isotonic crystalloids are effective in the majority of cases; however, if there is a poor response to fluid resuscitation the use of other fluid types should be considered and the patient evaluated for ongoing haemorrhage. Cats that are hypothermic and hypoperfused should be re-warmed slowly and only after fluid resuscitation has been initiated to prevent excessive vasodilation and subsequent vascular collapse.
Hypertonic crystalloids
Hypertonic fluids are associated with less tissue oedema than isotonic fluids, and thus may provide a theoretical benefit. 16 In humans with severe TBI (Glasgow coma score <8) and hypovolaemic shock, use of hypertonic fluids has been shown to produce a better outcome compared with isotonic fluids. 17 In patients without evidence of hypoperfusion, hypertonic saline is not associated with an improved outcome. 18 This is likely due to the promotion of intracranial oedema that occurs when large volumes of isotonic crystalloids are used for resuscitation in the face of injured brain tissue. 10 Hypertonic fluids are not associated with intracellular fluid accumulation, and therefore reduce this risk, and low volumes of isotonic fluids are not likely to cause significant oedema.
There is ongoing discussion about whether hypertonic crystalloids may confer a benefit for volume resuscitation where there is evidence of TBI (see above). Currently, however, there is no clinical evidence to suggest that hypertonic fluids result in better outcomes than isotonic fluids in animals.
Cats that have had multisystem trauma and suffered haemorrhage requiring large volumes of fluid for resuscitation will become anaemic. Should signs of hypoperfusion persist, whole blood transfusion or haemoglobin (Oxyglobin; OPK Biotech) infusion should be considered.
Oxygen therapy and airway management
All dyspnoeic patients will benefit from oxygen therapy. As mentioned, cats that have suffered head trauma often have a degree of respiratory compromise as a result of their facial injuries, and possibly also related to thoracic injuries (Fig 1). Oxygenation can be difficult to assess in these patients, so any dyspnoeic or severely hypoperfused patient should initially be provided with oxygen. This should be delivered in a stress-free manner, ideally using flow-by oxygen.

Lateral chest radiograph of a cat with pneumothorax following a road traffic accident
Specific problems that are treatable, such as pneumothorax, should be addressed. In some patients with severe upper airway trauma it may be necessary to perform a temporary tracheostomy. This is always best conducted in a controlled manner under general anaesthesia. Airway management techniques such as the use of a tracheally placed dog urinary catheter to provide oxygen may be useful as a temporary measure if it is not possible to place an endotracheal tube. In the majority of these patients the larynx is visible with a laryngoscope. Tracheostomies in cats are commonly associated with complications and therefore appropriate facilities for 24 h monitoring should be available. 19
Limiting secondary brain injury
Damage to the central nervous system in TBI typically occurs in two phases. The first, known as the primary neurological injury, occurs at the time of trauma and is mechanical in nature. The brain is subjected to laceration or shearing forces, resulting in bleeding or tearing of the neurovascular tissue. Secondary neurological injury refers to the subsequent cascade of events that results in progressive neuronal damage, both at the site of the initial injury and potentially extending globally to the brain as a whole. The brain is particularly sensitive to impaired oxygen and glucose delivery. Impaired cerebral ATP production leads to a failure of neuronal cell membrane pumps and excitotoxicity. 11
Minimising secondary brain injury is the primary goal when treating TBI in cats and this is discussed in more detail in the second part of the article.
Analgesia
All cats that have sustained trauma should receive analgesia. In the majority of cases this should initially take the form of an opioid agent. If there is concern about side effects, the cat should be monitored carefully — analgesia must not be withheld in these patients. Aside from the welfare implications, ongoing pain will be associated with central sensitisation, which may lead to the development of chronic pain states that are difficult to treat. Patients with TBI may be more sensitive to the sedative effects of these drugs, and therefore lower doses should be used and the drugs titrated to effect. Analgesia, and to some extent sedation, play a role in reducing cerebral metabolic rate and cerebral blood flow, and thereby intracranial pressure; thus, they may be of additional benefit in these cases. 20
Non-steroidal anti-inflammatory drugs (NSAIDs) should be avoided in the initial stages of case management due to the side effects that are associated with their use in the presence of hypoperfusion. Pure opioid agonists (eg, pethidine or methadone) can be reversed if problems are encountered and are, therefore, preferred. It should be stressed that side effects are rare if the drugs are used carefully and dosed to effect. Buprenorphine is an effective analgesic agent in cats and can be used for management of pain associated with trauma. It is suited to these patients as it is uncommonly associated with dysphoria or vomiting. 21
Once the cat is stable NSAID therapy can be used to provide longer term analgesia as required.
Ocular injuries
When ocular injury is present the first priority should always be the major body systems. Definitive management of the ocular injury must be delayed until such a time that anaesthesia is safe.
Enucleation — when to perform
If there is evidence of ocular rupture, rupture of the extraocular muscles, no visible pupil or hyphaema, the prognosis for vision is considered to be grave 23 and enucleation should be performed. There is also thought to be an association between globe trauma and the occurrence of primary ocular sarcomas. In one study five out of 13 cats with primary ocular sarcomas had a previous history of trauma to the globe. 24 For this reason many authors recommend enucleation of hydrophthalmic or phthisical eyes. 25,26

This cat with severe facial injuries requires enucleation of the proptosed globe as soon as is practically possible. Careful attention to appropriate analgesia and stabilisation prior to anaesthesia is essential. It is also important to prevent drying of or damage to the corneal surface of the other eye
Imaging
All cats that have sustained craniofacial trauma should undergo radiographic imaging of the thorax. In addition, radiographs of the skull may be useful in revealing fractures and luxations not easily identified on physical examination. Interpretation of skull radiographs can be challenging and it is useful to have normal cat skull radiographs and a skull to hand for comparison. Radiographs of the skull are best taken under general anaesthesia, which will ensure that the head is straight. Laterolateral and ventrodorsal/ dorsoventral radiographs should be performed initially. Other views may be necessary — in particular, oblique radiographs can be useful for assessment of orbital structures.
Computed tomography is a more sensitive method of assessment for most types of skull fractures 27 and may be helpful for planning surgical repairs in complex cases. It has limited availability and is most useful where there are the skills for management of complicated fractures.
Whichever modality is chosen, it is important to ensure that the images are optimal to prevent misdiagnosis.
Jaw injuries
Jaw injuries tend to occur in conjunction with ocular and other craniofacial injuries and, in many cases, can be managed easily in practice. More complicated mandibular and maxillary fractures may require referral to a specialist surgeon or dentist.
Cats with jaw injuries tend to hold their mouth open, salivate and will be generally painful around the mouth. Direct palpation is normally resented and therefore the precise nature of the injury may not be apparent on initial conscious examination. General anaesthesia is recommended to allow manipulation of the jaw to assess the extent of the injuries.
As discussed for ocular injuries, full stabilisation and treatment of more serious injuries should be achieved prior to further investigation and treatment of jaw injuries.
Mandibular fractures
Mandibular fractures are typically fairly obvious on physical examination. Separation of the mandibular symphysis is commonly seen (Fig 3) and cats should also be assessed for luxation of the temporomandibular joints, damage to the teeth and fractures of the maxilla.

Intraoral radiographs showing (a) mandibular symphyseal separation and (b) appropriate apposition following wiring
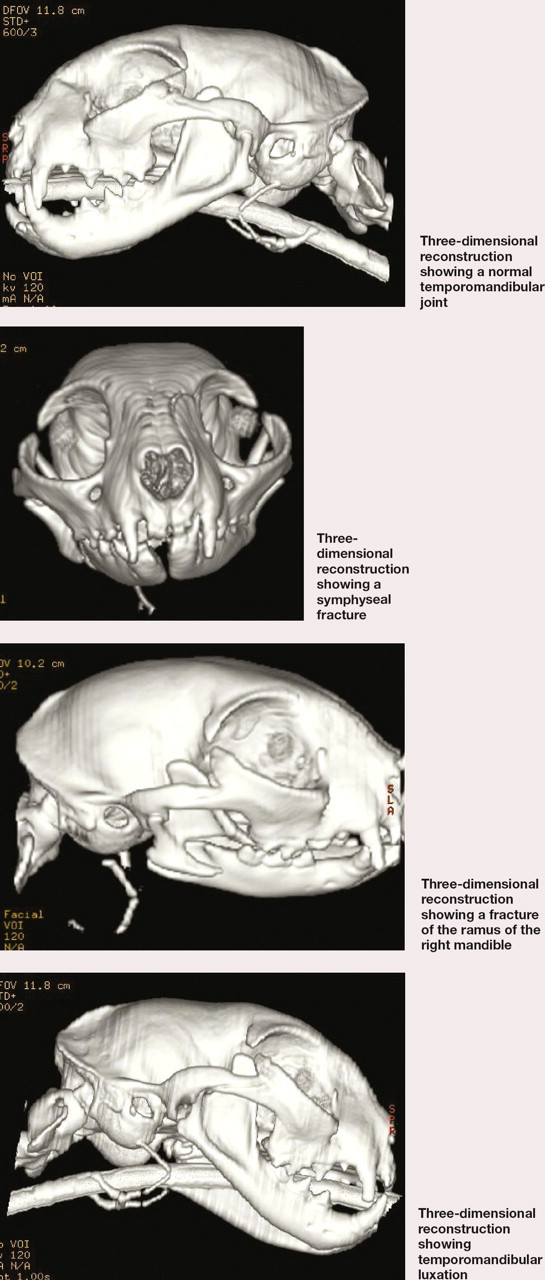
Radiography is very useful, particularly for more caudal fractures, which may not be apparent on oral examination. Laterolateral, dorsoventral, oblique and intraoral radiographs should be obtained as necessary. Computed tomography (CT) can be invaluable in providing additional information, particularly for complicated fractures and those involving the temporomandibular joint (see box, left). Radiographs and CT scans are also essential to allow accurate treatment planning for fractures to be managed surgically.
Computed tomography of the mandible and temporomandibular joint
Surgery or conservative management?
Detailed discussion of the management of mandibular and maxillary fractures is beyond the scope of this article. Stable, non-displaced fractures may be managed conservatively. (Note that the use of tape muzzles as a method of repair is not appropriate in cats.) 28 If there is severe malocclusion, marked instability of larger fragments and/or obstruction of the nasal cavity, then surgical repair of the fracture is indicated.
Generally when managing jaw fractures it is more important to consider dental occlusion than fracture reduction and this should be assessed under anaesthesia prior to waking the cat. It may be necessary to place the endotracheal tube via a pharyngostomy incision to allow full assessment of dental occlusion during surgical repair.
Mandibular symphyseal (and also hard palate) fractures can be wired using the canines as support to stabilise the fracture (see page 812). Uncomplicated mandibular symphyseal fractures typically heal quickly with a low risk of complications. Once these fractures have been stabilised most cats are comfortable to eat (unless there are concurrent mandibular body or ramus fractures) and so feeding tubes are generally not required. The wires should be removed once union has occurred, which is at approximately 6 weeks in cats.
Fractures of the mandibular body can be more challenging to manage. Intramedullary pinning is not a suitable method of repair, and a plate and screws should be used with care as they may result in tooth root damage. 29 Interarcade canine acrylic bonding is a useful technique for the management of many mandibular body fractures. For more information, readers should consult an appropriate orthopaedics textbook.
Open oral fractures should be treated similarly to other open fractures, with lavage, debridement, surgical stabilisation and antibiosis.
Maxillary fractures
Maxillary fractures can be more difficult to diagnose than mandibular fractures and surgical treatment can be challenging. Advice from a specialist should be sought if there is any doubt as to whether conservative or surgical therapy should be pursued.
Step - by - step repair of a symphyseal fracture

Post-trauma management
Cats that have suffered severe head or jaw trauma are often reluctant to eat in the recovery period. Force-feeding is not appropriate in cats and appetite stimulants rarely, if ever, encourage sufficient intake to ensure the patient's full nutritional requirements are met. It is much more appropriate to place a feeding tube (Fig 4) at an early stage, and remove it if it is not required, than to not feed a recovering cat. The use of oesophageal feeding tubes is preferred as long as there is no vomiting. These tubes are extremely well tolerated in cats and associated with few complications. 30 They are also easy for owners to use and maintain, enabling patients to be managed at home. 31 They are available in wide bores allowing the feeding of semi-liquid or patty-like diets. Nutritional management should be commenced as soon as the patient is cardiovascularly stable, with a third to a half of the resting energy requirements (RER) provided in up to six meals daily.

An oesophageal feeding tube provides an effective method of nutritional management in head trauma patients
RER in cats = 30 × BW (kg) + 70
NB. There is no need to apply illness requirements to this equation in hospitalised patients.
KEY POINTS
Management of cats with craniofacial trauma can be frustrating at times and recovery periods in the severely traumatised patient can be prolonged.
With careful stabilisation of the cat and patience, successful management is possible in many cases.
Diligent assessment for pain and appropriate management of nutrition is vital in cats with severe facial trauma due to the longer convalescence period associated with multiple injuries.