
Abstract
Feline parotid salivary duct sialocele is an uncommon disorder that has been previously reported in association with traumatic rupture of the duct in only two cats. Both cases were successfully treated by proximal duct ligation. We describe the successful surgical treatment of a parotid duct sialocele, secondary to spontaneous salivary duct stenosis, in an adult domestic shorthair cat. The cat was referred for assessment of a recurrent fluid-filled swelling on the left side of the face. Cytology of the aspirated fluid was consistent with serous saliva. The anatomical localisation of the lesion and the nature of the fluid were indicative of parotid gland/duct involvement. Retrograde sialography by parotid duct cannulation was unsuccessful because the left parotid duct opening was stenosed and obstructed by scar tissue. Surgical exploration revealed a parotid salivary duct sialocele, which was completely removed along with the parotid gland without complications.
A 5-year-old, indoor, spayed female domestic shorthair cat was referred to the National Veterinary School of Alfort (France) for a recurrent fluid-filled swelling on the left side of the face. The onset of the lesion was observed 2 months previously.
Antibiotic treatments and three consecutive needle drainages were performed without resolution of the swelling. No history of facial trauma or dysphagia was reported.
Clinical examination revealed the cat to be bright and alert with a 3 cm soft, fluctuant and non-painful subcutaneous swelling on the left side of the face. Ophthalmological evaluation and the examination of the oropharynx revealed no abnormalities and the remainder of the clinical examination was unremarkable.
Differential diagnosis included soft tissue abscess, tooth abscess, neoplasia and parotid or zygomatic salivary mucocele.
Fine-needle aspiration of the swelling was performed. The sampled liquid was translucent and microscopic examination revealed non-mucinous fluid containing a low number of large phagocytic cells with small round nuclei and abundant foamy cytoplasm (Fig 1A and B). This cytological appearance was consistent with serous saliva. Dorsoventral and lateral radiographs of the skull were performed under general anesthesia. Radiographic images showed focal thickening of soft tissues in the left mandibular area, adjacent to the ramus of the mandible and the zygomatic arch (Fig 2). Boney lesions were not observed. The anatomical localisation of the lesion and the nature of the fluid were indicative of parotid gland/duct involvement. A retrograde sialography was attempted; however, the left parotid duct could not be cannulated. A20F vein catheter and a 2/0 or 3/0 USP monofilament nylon suture were used for these trials. On gross examination, the papilla stoma appeared to be non-patent because of obstructive scar tissue. A tentative diagnosis of parotid salivary duct sialocele associated with parotid duct stenosis was made and a surgical exploration was performed. The cat was anaesthetised and positioned in right lateral recumbency. The left side of face was clipped and aseptically prepared. A 4 cm horizontal skin incision was made over the swelling. The cystic lesion appeared to be a dilated portion of the parotid glandular duct, continuous with the parotid gland. The dissection was continued and excision of duct sialocele and parotid gland were performed. The surgical site was closed routinely. No sialoliths were found in the excised tissue.

(A) Numerous vacuolated phagocytic cells in the sialocele aspirate (Giemsa stain). (B) High magnification of vacuolated phagocytic cells (Giemsa stain).

Dorsoventral skull radiograph showing focal thickening of soft tissues in the left mandibular area (white arrows), not associated with bone lesions.
The specimen was fixed in 10% buffered formalin and processed routinely.
Histopathological analysis revealed a cystic structure continuous with the parotid duct, consisting of dense connective tissue, thick wall, and not delineated by an epithelium. This tissue was highly vascularised and comprised numerous fibroblasts and collagen fibres. A mononuclear inflammatory reaction was present around many vessels. The salivary gland appeared oedematous with a sclerotic interstitium (Fig 3).
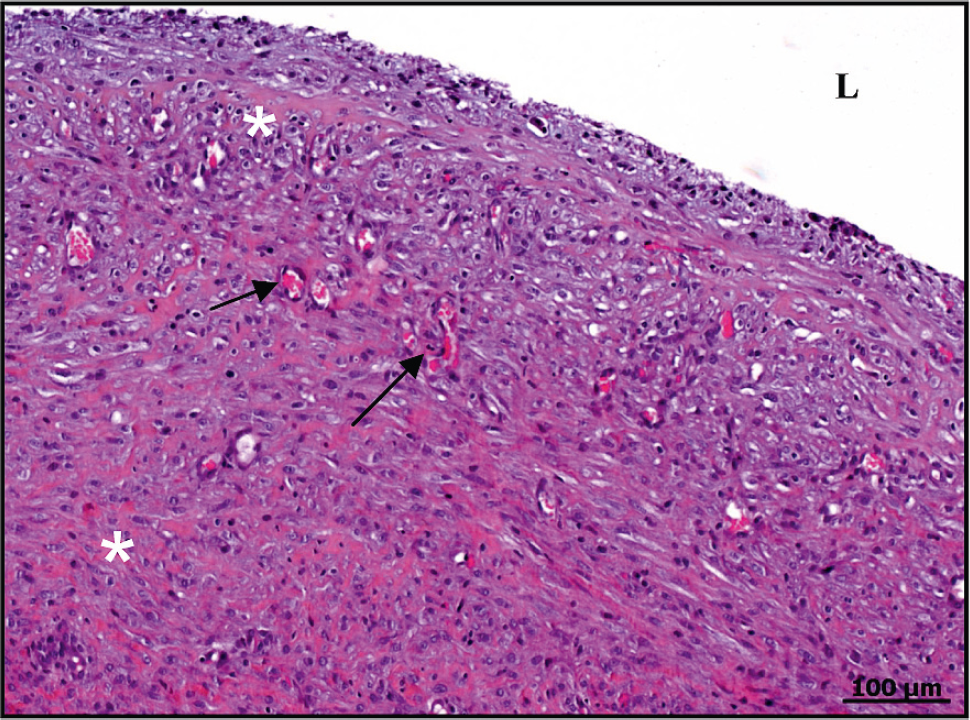
The cyst wall consisting of a heavy and highly vascularised (vessels: black arrows) connective tissue (orange stained, collagen fibres: white asterisk); L = cyst lumen. Haematoxylin eosin saffron stain.
Histological examination confirmed a parotid salivary duct sialocele.
Sutureswere removed 15 days after surgery with complete resolution of the swelling. Clinical examinations were performed at 3 and 6 months postoperatively. No-recurrence of the lesion was reported during the 1-year telephonic follow-up period.
Salivary glands diseases are infrequently diagnosed in cats; neoplasia is the most commonly reported pathological condition.1,2 Feline salivary mucoceles are in general uncommon and a limited number of cases have been reported. The sublingual salivary gland is the most often affected3–7 whereas parotid8,9 and zygomatic 10 gland involvement is rare.
Salivary mucoceles are single or multiloculated cavities with an inflammatory connective tissue lining, contiguous to a salivary gland or duct.11,12 Salivary mucoceles or sialoceles occur when the saliva leaks from a damaged salivary gland or duct into the subcutaneous tissue. The superficial location of the parotid gland and its glandular duct makes them susceptible to injury. Bite wounds, blunt or concussive trauma, tooth abscesses and foreign bodies are potential causes of parotid salivary gland lesions. 13 Effects are usually self-limiting: wounds heal rapidly because of an abundant local vascular supply. However, the underlying aetiology for the formation of sialoceles remains unknown, 11 and the pathogenesis of this pathological condition has not been firmly established.
Parotid salivary sialoceles have been reported in only two cats, associated with traumatic duct rupture (bite wound 8 or iatrogenic surgical procedure 9 ) and salivary fistula recurrence.8,9 In these two reported cases, sialography confirmed the diagnosis and the sialoceles were surgically treated by proximal duct ligation. This surgical procedure was reported to be simple, quick and effective.8,9 The ligation of ducts causes back pressure which results in glandular atrophy. 14 This theory is supported by experimental studies in rodents: duct ligation of salivary glands produces glandular atrophy without mucocele occurrence. 15 Nevertheless, experimental studies in cats suggest that the complete ductal obstruction may be a possible aetiological factor in mucocele formation.4,16 Harrison and Garrett demonstrated in cats that extravasated saliva induced the migration of macrophages and a fibroblastic reaction. 16 It was hypothesised that if the quantity of extravasated saliva could not be contained by the resultant reaction then sialocele formation would occur. In our case, we postulate that the spontaneously occurring stenosis, and subsequent obstruction of saliva flow, may be a possible cause of salivary duct sialocele or extravasation of saliva and subsequent sialocele formation, although the causes of duct stenosis have not been identified. No history of facial, or oral cavity, trauma or diseases were reported. Sialoliths were not found during the surgery and neoplasia was not seen at the histological examination.
The identification of the affected salivary gland is essential to plan the surgical management. Within large areas of saliva collection, the affected salivary gland/duct cannot easily be identified. In these cases, the sialography facilitates diagnosis and can be useful. 17 Nevertheless, plain radiography and fine-needle aspiration may be sufficient to make up a preliminary diagnosis, 10 as in our case. Diagnosis of parotid salivary duct sialocele was based on the anatomical lesion location, palpation (non-painful, fluctuant) and presence of serous fluid filling the lesion. The cytological appearance of the analysed fluid ruled out mixed seromucinous salivary glands involvement. 13
Stenosis of the parotid glandular duct may be considered as a possible cause of parotid salivary sialocele. Preoperative diagnosis may be facilitated by macroscopic aspect and cytological examination of the fluid to distinguish parotid from other salivary glands. In our case, parotid gland/duct sialocele removal was effective in treating this lesion, without early and long-term complications.