
Abstract
This report describes a cat that suffered pelvic urethral rupture associated with multiple pelvic fractures. A vaginourethroplasty was performed as a salvage procedure, via intrapelvic anastomosis of the proximal urethra to the caudal vagina, following failure of a primary urethral anastomosis. Urinary diversion was achieved via tube cystostomy and a vagino-urethral catheter was maintained for 3 days postoperatively. Anterograde cystourethrography was performed at 7 days and 14 days postoperatively. Absence of contrast leakage from the vagino-urethral anastomosis was documented at 14 days postoperatively and the tube cystostomy was removed. An Escherichia coli urinary tract infection was treated following removal of the tube cystostomy and subsequent urine culture revealed no evidence of urinary tract infection. The cat retained normal urinary continence and elimination behaviour during the 7-month follow-up period. Vaginourethroplasty could be considered as a salvage option for management of traumatic pelvic urethral rupture in the neutered female cat.
Urethral rupture may occur following vehicular trauma, bite wounds, penetrating injuries, urethral calculi or iatrogenic injury during urethral catheterisation or surgery.1–4 Management of urethral rupture requires patient stabilisation, correction of metabolic disturbances and provision of urinary diversion. There are three options for the management of urethral rupture: temporary urinary diversion via a tube cystostomy or urethral catheter and second intention healing of the urethra, permanent urinary diversion via a urethrostomy or primary urethral repair. 5 Second intention healing of the urethra is only appropriate when the urethral defect is small. 4 Primary urethral repair is challenging due to the small size of the feline urethra and is associated with complications of urethral dehiscence and stricture.5,6 Permanent urethrostomy may provide a satisfactory outcome, however, the rate of complications can be greater following urethrostomy at more cranial sites. Prepubic and transpubic urethrostomy achieve permanent bypass of urethral lesions of the pelvic urethra, however, a relatively high rate of complications, including urinary incontinence and peristomal skin irritation and necrosis, are documented. 7
This case report describes the use of an end-to-end vagino-urethral anastomosis (‘vaginourethroplasty’) to achieve permanent urinary diversion in a cat following traumatic urethral rupture and failure of primary urethral anastomosis.
A 9-year-old female neutered domestic shorthair cat (3 kg) was referred for management of pelvic fractures, following a road traffic accident. Plain and contrast radiography revealed a right iliac shaft fracture, multiple pubic and ischial fractures and rupture of the pelvic urethra (Fig 1).A tube cystostomy was placed to achieve urinary diversion on the day of presentation using a standard technique. 8 Surgical exploration of the pelvic urethra on the fourth day, documented complete urethral transection, 3 cm from the bladder neck, and a primary urethral anastomosis was performed. The right iliac shaft fracture was stabilised using a 2.0/2.7 mm lateral veterinary cuttable plate (Synthes, Welwyn Garden City, UK) on the sixth day following presentation. Anterograde cystourethrography performed 20 days following urethral anastomosis revealed a stricture and persistent contrast leakage at the anastomosis site (Fig 2), necessitating surgical revision.

Retrograde vaginourethrocystogram performed on the day of presentation. This demonstrates contrast leakage from the pelvic urethra, consistent with urethral rupture.

Anterograde cystourethrogram performed via the tube cystostomy 20 days following primary repair of the complete pelvic urethral rupture. This demonstrates leakage of contrast material and the presence of a stricture at the anastomosis site.
Under general anaesthesia the cat was prepared for a vaginourethroplasty surgery via a ventral midline laparotomy and pubic symphysiotomy, including antiseptic lavage of the vulva which was draped within the sterile field. An 8 Fr nylon catheter was passed normograde, via a stab incision in the urinary bladder, through the proximal urethra allowing improved visualisation of the site of urethral stricture. A 5 Fr Foley catheter was inserted in a retrograde fashion per vagina. The vagina was then transected and spatulated at the level adjacent to the previous urethral anastomosis, allowing the tip of the Foley catheter to exit the distal vagina at this point. The cervical remnant and proximal portion of the vagina were resected. A 5 mm portion of urethra, at the site of previous anastomosis, was resected and the distal urethra was ligated using an encircling ligature of 3–0 polydioxanone. The proximal urethra and distal vagina were then apposed by advancing the Foley catheter into the distal opening of the proximal urethra (Fig 3). The anastomosis was sutured using a simple interrupted pattern of 5–0 polydioxanone on a round bodied needle circumferentially; eight sutures were placed and surgical Loupes (3.5x) were used for magnification. The vaginourethral anastomosis site was omentalised prior to routine abdominal closure.
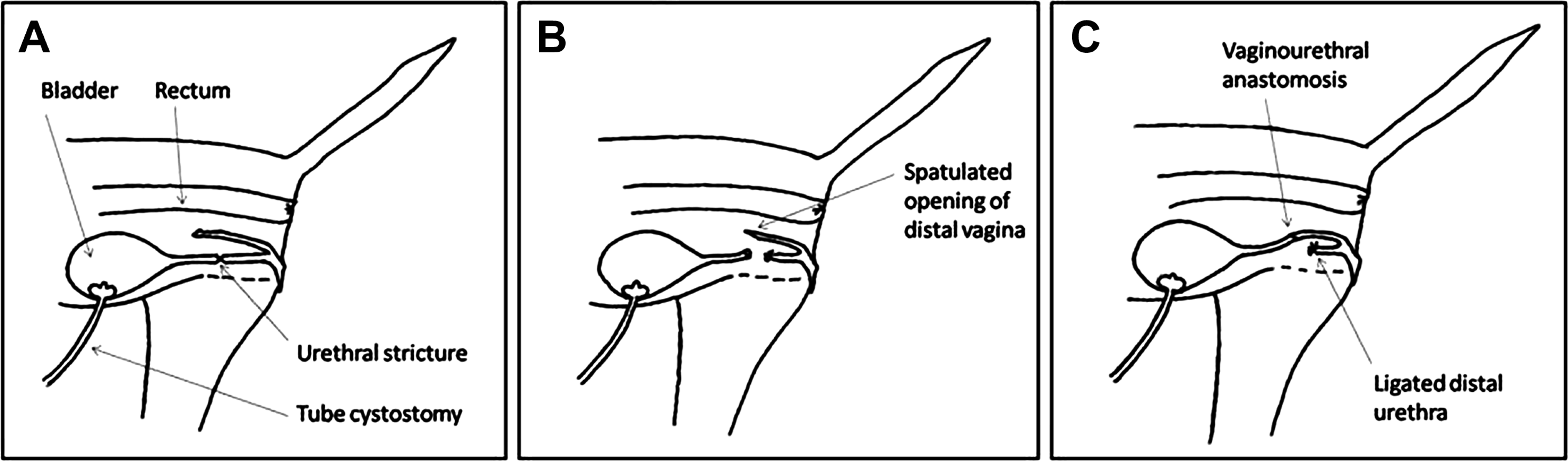
A schematic diagram of the caudal abdomen and pelvis of the cat demonstrating the stages of the vagino-urethral anastomosis procedure to create the vaginourethroplasty.
Continued urinary diversion was provided via the tube cystostomy and the vagino-urethral Foley catheter was closed and left in situ for 3 days postoperatively. Anterograde cystourethrography was performed under general anaesthesia at 7 days and 14 days postoperatively by injection of a 2 ml/kg bolus of iohexol (Omnipaque; GE Healthcare AS, Oslo, Norway, 300 mg I/ml) diluted in a 1:1 ratio with sterile saline via the tube cystostomy. Leakage of contrast agent was documented from the vagino-urethral anastomosis site at 7 days postoperatively but was not present by 14 days (Fig 4) and the tube cystostomy was, therefore, removed. Urinalysis and culture at this time revealed an active urine sediment and a profuse growth of Escherichia coli. A 4-week course of enrofloxacin (5 mg/kg po q 24 h) was prescribed on the basis of sensitivity testing.

Anterograde cystourethrogram 15 days following vaginourethroplasty demonstrating the healed anastomosis between the cranial vagina and distal portion of urethra. There is slight narrowing at the anastomosis site but no evidence of contrast leakage.
The cat was re-examined 4 and 16 weeks postoperatively. The owners observed that she urinated normally with no evidence of dysuria and that she retained normal urinary continence. There was no evidence of perineal urine scald or vulval inflammation. A urine sample was obtained via cystocentesis 1 week following cessation of antibiotic treatment and the urine sediment was unremarkable and culture yielded no bacterial growth. The cat was represented at 24 weeks postoperatively following a 2-week history of vomiting. Abdominal ultrasonography revealed a grossly thickened gastric wall with complete loss of layering. The owners declined further investigations and the cat was euthanased 1 month later due to progression of her disease; post-mortem examination was not performed.
The majority of published literature regarding management of feline urethral rupture describes the condition in the male cat.1–5 Literature regarding urethral rupture in the female cat is very limited.1,9 Extrapolating from the canine literature, the optimal management of transection of the pelvic urethra is primary urethral anastomosis over a urethral stent with concurrent urinary diversion.5,10,11 Following failure of this technique, revision of the urethral anastomosis was considered unfeasible due to the risk of tension at the anastomosis site following excision of the stricture. Vaginourethroplasty was performed as an alternative salvage option to prepubic, 7 subpubic 12 or transpelvic 13 urethrostomy, to maintain greater urethral length and normal elimination behaviour.
The vaginourethroplasty technique employed in this cat was modified from that previously described for management of urethral neoplasia in the bitch14,15 to account for anatomical species differences. In the bitch, the luminal disparity between the vagina and urethra necessitates resection of the ventral vaginal wall and closure over a catheter to create a narrow ‘vaginourethra’ 15 however, in contrast, the narrow lumen of the feline vagina allowed a direct anastomosis of the proximal urethra to the distal vaginal. In fact, the end of the distal vagina was spatulated in this cat to increase the luminal diameter of the vagina. The small size of the feline urethra and vagina presents a technical challenge during both primary urethral anastomosis and vaginourethroplasty; however, magnification was used to ameliorate this problem. Whilst the primary urethral anastomosis failed, successful healing of the vagino-urethral anastomosis was achieved. This is likely to be due to improved urethral tissue characteristics following a delay posttrauma, in addition to use of the non-traumatised distal vagina which provided a tension free site for anastomosis.
Following the vaginourethroplasty procedure, continued urinary diversion was employed via the tube cystostomy and an indwelling closed vagino-urethral catheter was left in place as a stent for 72 h. Urinary diversion to bypass the anastomotic site is associated with improved urethral healing and reduced incidence of dehiscence and stricture.16,17 The period for which a catheter was used for vagino-urethral stenting was similar to the previous canine case series in which the catheter was retained for 48 h. 15 The rationale for use of a catheter as a vagino-urethral stent is based upon a canine experimental study in which minimal urethral stricture was demonstrated following suturing of a urethral anastomosis over a catheter compared to other non-sutured anastomoses, or those without an indwelling catheter. 10 It has been demonstrated in experimental dogs that urothelial regeneration occurs rapidly across urethral defects if some mucosal continuity is present, 16 however, it is unclear how mucosal healing would occur at the vaginourethral interface.
A urinary tract infection was documented in this cat, however, resolution occurred following antibiotic treatment and it is recognised that the use of a tube cystostomy 18 and indwelling urethral catheter 19 predispose to urinary tract infection. There was no indication that the cat was predisposed to urinary tract infection during the follow-up period; however, longer term follow-up of this technique in additional cats is required.
This report describes the modification of an existing technique of vaginourethroplasty for permanent urinary diversion in a female neutered cat with a traumatic pelvic urethral rupture associated with pelvic fractures. The technique allowed retained continence and elimination behaviour and was not associated with any complications. This report highlights an alternative salvage option to urethrostomies in neutered female cats for management of urethral trauma.