
Abstract


Ovarian remnant syndrome
Ovarian remnant syndrome (ORS) is the presence of functional ovarian tissue with signs of estrus after ovariohysterectomy or ovariectomy. Signs of estrus may occur weeks to many years after surgery and include lordosis, vocalizing, rolling on the ground and receptivity to intact males. 1 The cause of ORS is failure to remove all or part of an ovary at surgery, or revascularization of ovarian tissue inadvertently dropped into the abdomen during ovariohysterectomy/ovariectomy. 2,3 Neoplasia in ovarian remnants, such as granulosa cell tumor, is a rare cause of ORS. Age at the time of surgery and the breed of cat do not appear to influence the risk of ORS, although one report did not find any cases in queens spayed before 4 months of age. 1
Diagnostic methods
Diagnosis is most commonly made by observing signs of estrus in a spayed cat with coincident vaginal cytology (Fig 1) consistent with estrus (cornified epithelial cells, absence of red/white blood cells, clear background).

Taking a sample for vaginal cytology. The swabbed sample should be spread across the slide for examination
Documentation of serum estradiol levels >20 pg/ml (>73.4 pmol/l) while signs of estrus are occurring is also consistent with ORS, although the diagnosis cannot be ruled out if estradiol levels are low.
Another method involves inducing ovulation of mature ovarian follicles during estrus with gonadotropin-releasing hormone (GnRH) (Cystorelin; Merial, 25 μg IM) and documenting elevated serum progesterone (>2 ng/ml [6.4 mmol/l]) 2 weeks later.
Detection of ovarian activity when a queen is not in estrus has been described by administering the GnRH analogue buserelin (Receptal; Intervet/Schering-Plough Animal Health, 0.4 μg/kg IM), with measurement of serum estradiol 2 h later. 4 Serum estradiol concentrations >3 pg/ml (>11 pmol/l) were consistent with the presence of ovarian tissue. No adverse effects from administration of buserelin were noted.
Surgical treatment
Once ORS is confirmed, the ovarian tissue should be surgically removed. Queens with ovarian remnants may be at increased risk of mammary and ovarian neoplasia. Moreover, many owners will not be tolerant of the estrous behavior. Exploratory laparotomy is required to remove the ovarian remnant. A thorough search of the peritoneal cavity is necessary, starting at the most common location for remnants, the ovarian pedicles. Other common sites for ovarian remnants are the omentum and the peritoneal walls. Remnants may be unilateral or bilateral. Surgery is most rewarding if performed when the cat is in diestrus or has been induced to ovulate. The corpora lutea are visible as yellow—orange structures against the red background of ovarian tissue. Excised tissue should be submitted for histopathology to confirm ovarian tissue has been removed.
In some cases, queens have undergone more than one laparotomy in an attempt to resolve ORS; failed attempts to locate ovarian remnants are a common reason for referral to a board-certified surgeon.
Mammary fibroadenomatous hyperplasia
Approximately 80% of feline mammary masses are neoplastic, most commonly adenocarcinomas. The remaining 20% are benign and are predominantly mammary fibroadenomatous hyperplasia (MFH; also called fibroepithelial hyperplasia). MFH is most commonly seen in young cycling queens, but may also be seen in pregnant queens, and in male or female cats treated with progestins (eg, megestrol acetate, medroxyprogesterone acetate). 6,7 Typically most or all of the glands are affected. The hyperplasia can be severe, leading to tissue necrosis, ulceration and infection (Fig 2).

(a) Mammary hyperplasia in a young late-gestation pregnant queen. A litter of kittens was born 12 days later. The queen was treated with cabergoline, broad-spectrum antibiotics and analgesics. The kittens were hand-raised. (b) The same queen approximately 2 months later, after ovariohysterectomy. Courtesy of Dr Shelagh Morrison
Etiology and diagnosis
MFH is often mistaken for neoplasia on gross appearance. Histologically, the lesions consist of benign, unencapsulated, fibroglandular proliferation. Progesterone receptors have been commonly found in MFH samples, while estrogen receptors have been found in only 50% of cases. 8 The etiology is suspected to be an exaggerated response to natural progesterone or synthetic progestins, but the disease is also occasionally reported in sterilized male or female cats with no history of progestin therapy. In spayed queens, ORS may be the initiating cause.
A diagnosis of MFH is suspected on the basis of clinical signs, patient signalment and history. Biopsy of affected tissue and histopathology is confirmatory. However, surgical biopsy of markedly swollen mammary glands may create incisions that heal poorly due to wound tension.
Treatment approaches
Treatment varies with the underlying cause. Intact queens should be spayed, and a flank approach is most appropriate (Fig 3). If the cat is being treated with progestins, treatment should be stopped. The drug of choice for treatment of MFH is the progesterone receptor blocker aglepristone (Alizin; Virbac, 10–15 mg/kg/day SC, days 1, 2 and 7). 9,10 One study monitored 14 queens with MFH for 12 months following treatment with aglepristone. 11 Remission of clinical signs occurred in an average of 4 weeks. Cats that had been treated with long-acting medroxyprogesterone acetate required treatment for 5 weeks. Six of the queens were subsequently bred and four delivered normal litters. Aglepristone may not be available or licensed for cats in every country.

The flank approach to ovariohysterectomy is useful in cases of mammary hyperplasia
Anecdotal information suggests other treatment choices include dopamine agonists that reduce prolactin levels, such as cabergoline (5 μg/kg/day PO, 5–7 days) or bromocriptine (0.25 mg/cat/day PO, 5–7 days). Prolactin appears to be necessary for the maintenance of the corpora lutea, which produce progesterone. For cats that have not received exogenous progestins, dopamine agonists may be useful to reduce endogenous progesterone levels. In most countries, these drugs are not licensed in the cat and must be obtained from a compounding pharmacy. Infections should be treated with broad-spectrum antibiotics.
Occasionally, MFH will resolve spontaneously, but it typically takes several weeks to several months to resolve, even with treatment.
Spayed or intact?
It may be difficult to determine if an adult queen with unknown history has been previously spayed. Traditional methods to determine reproductive status include observing for signs of estrus and examining the ventral abdomen (or flank) for a surgical scar that may be due to ovariohysterectomy/ovariectomy. Surgical scars will not be evident on all cats — and, if a scar is found, there is no guarantee it is from surgical sterilization.
Serum LH can be used to determine reproductive status. LH is released from the anterior pituitary gland in response to copulation. LH stimulates ovulation and luteinisation of mature ovarian follicles. In intact queens, serum LH is maintained at basal levels through the negative feedback provided by ovarian estradiol secretion. Following ovariohysterectomy/ovariectomy, this negative feed-back is lost and serum LH levels elevate persistently.
A rapid, semi-quantitative colorimetric assay is available that shows a positive result when serum LH level is >1 ng/ml (Witness-LH; Synbiotics Corporation). The test was developed for timing of canine ovulation and has been validated in the queen — test sensitivity and specificity for determination of reproductive status were determined to be 100% and 92%, respectively. 5 A single negative test is highly likely to indicate a sexually intact queen. A single positive test suggests a spayed queen, although false-positives may occur if an episodic LH surge is sampled or the queen is in estrus. The manufacturer recommends that positive tests be confirmed with a second sample taken 2 h later. Anecdotally, equivocal test results have been reported in some spayed cats. Some commercial laboratories offer LH testing to veterinarians, but these assays may not have been validated for the dog or cat, so investigation to determine validity is recommended.
Pregnancy diagnosis
Clinical signs
Failure of a queen to come back into heat after breeding is one of the most obvious signs of pregnancy, but pseudopregnancy will produce the same effect. However, queens experiencing a pseudo-pregnancy will usually return to heat within 50–60 days of the last estrus. One of the first physical indications of pregnancy is ‘pinking’ of the nipples, which occurs around days 15–18 after ovulation. This change in the nipples, which become noticeably pinker and easier to see as they increase in size and the hair around them recedes somewhat, is most obvious in maiden queens. It can be recognised with experience in queens that have had several litters as well.
Palpation
The developing fetuses can be palpated in the abdomen as early as 14–15 days after breeding, but most easily at about 21–25 days. They remain distinctly palpable up to about 35 days, at which point the fetuses and placentas are sufficiently large that they cannot easily be distinguished individually. Towards the end of pregnancy, the heads of fetuses may be very easy to palpate.
Hormonal assay
Traditionally, there has been no blood test available in the cat to detect pregnancy. Cats do not produce a placental hormone similar to human chorionic gonadotropin (hCG), which is the basis for some human pregnancy tests. However, the hormone relaxin is produced primarily by the placenta and is, therefore, a useful marker for pregnancy. Relaxin levels increase in pregnancy but not in pseudopregnancy. An in-clinic test kit (Witness Relaxin; Synbiotics) has been developed as a rapid means of pregnancy detection in cats and dogs. The test requires a small volume of plasma and results are available in about 10 mins.
In a study designed to evaluate the commercially available relax-in test kit, 11 queens were mated and monitored for pregnancy. 12 All queens were confirmed pregnant and delivered kittens. An additional 13 pregnant queens undergoing ovariohysterectomy were also tested. A group of 23 non-pregnant cats were tested as controls. The kit was able to detect pregnancy between days 20–25 of gestation. All pregnant queens tested negative within 5 days post-partum. In the control group, two cats tested false-positive, both of which had large ovarian cysts. This suggests another possible source of relaxin production in some queens. The test was estimated to have 100% sensitivity and 91% specificity in cats after day 25 of gestation, with a positive predictive value of 93%.
Radiography
Radiography may be used to detect pregnancy once fetal bones begin to mineralize, as early as 25–29 days before parturition. 13 Until this time, only uterine enlargement may be detected. It is not possible to distinguish pregnancy from uterine disease (eg, pyometra) at this point. There is a predictable sequence of radiographic bone mineralization in the cat, similar to that of the dog, but beginning about 1 week earlier in gestation. 13 In one study, prediction of date of parturition within 3 days was possible for 75% of 32 cats (and within 7 days in all cats) using references for bone mineralization. 13 Not all structures were reliable for prediction of parturition, however. Mineralization of the humerus and femur occurs over the narrowest range, while the ulna, fibula and pelvic bones have more variable mineralization times. The fibula, calcaneus and phalanges may not become visibly mineralized before parturition. Another use of radiography is in determining the number of fetuses, simply by counting the number of skulls present.
A pregnant queen at term. Radiography is useful for determining the number of fetuses, simply by counting the number of skulls present

Ultrasonography
Ultrasound is a more sensitive test for pregnancy than radiography. The gestational sac, a spherical anechoic structure slightly compressed at the pole, can be detected at 11–14 days, and the embryo at 15–17 days post-breeding. 14 From day 30, it is possible to identify fetal organs. Details on the time of ultrasound appearance of various fetal and extra-fetal structures in the cat have been published. 15,16 A benefit of ultrasound is the ability to determine fetal viability through detection of a beating heart (about 16 days) and fetal movement (about 32 days). Fetal heart rate in the cat averages about 230 beats per min (range 193–263 beats per min) and remains constant throughout gestation, unlike the dog. 17 Gender determination is even possible, at about days 38–43 post-breeding. 18
Early fetal death is also identifiable — ultrasound exams performed on consecutive days will show that the gestational sacs decrease in size. However, ultrasound may not be as good as radiography for determining the number of fetuses present. The ultrasound exam views each fetus individually and movement of the queen or the uterus makes identification of individual fetuses confusing. Ultrasound pregnancy diagnosis is 99% accurate at 28 days.
Gestational age and due date
Prediction of gestational age (GA) and date of parturition is possible using fetal ultrasound measurements of head (HD) or body diameter (BD). 19
GA (days) = 25 x HD + 3 or 11 × BD + 21
Days before parturition = 61 — GA
Using these formulae, the due date can be estimated ± 2 days about 75% of the time. Ideally, the measurements should be taken 23–28 days post-breeding.
Many sonographers prefer that the hair coat is clipped as this gives the best image quality. If the hair coat is not going to be clipped, alcohol or another wetting agent can be used in addition to acoustic coupling gel to decrease the amount of air between the transducer and the skin, and thereby improve image quality. However, it is still possible to get a false-negative pregnancy diagnosis early in pregnancy if the hair coat is not clipped. Ideally, the queen should have a full bladder to move the bowel out of the way and also to move the uterine body out of the pelvic canal so it is more readily imaged. It also helps to fast the queen for 12 h before the ultrasound examination so that intestinal gas is less likely to obscure the views, especially in early pregnancy.
Congenital anomalies in the reproductive tract of the queen
Congenital anomalies of the queen's reproductive tract are not common and are poorly described in the literature. Segmental aplasia/hypoplasia/agenesis of the uterine horn, often called uterus unicornis, may be encountered occasionally and can present difficulties for veterinarians when found incidentally during ovariohysterectomy/ovariectomy (Fig 4). Anecdotally, this condition appears to be more common in Ragdoll cats than in other breeds or non-pedigree cats. One uterine horn may be missing or reduced to a thread-like remnant, and the ipsilateral kidney is often absent. 20–24 However, both ovaries are typically present and the surgeon must ensure the ipsilateral ovary is found and removed during neutering surgery. Failure to remove the ipsilateral ovary is likely to result in ORS and necessitate an exploratory laparotomy at a later date.
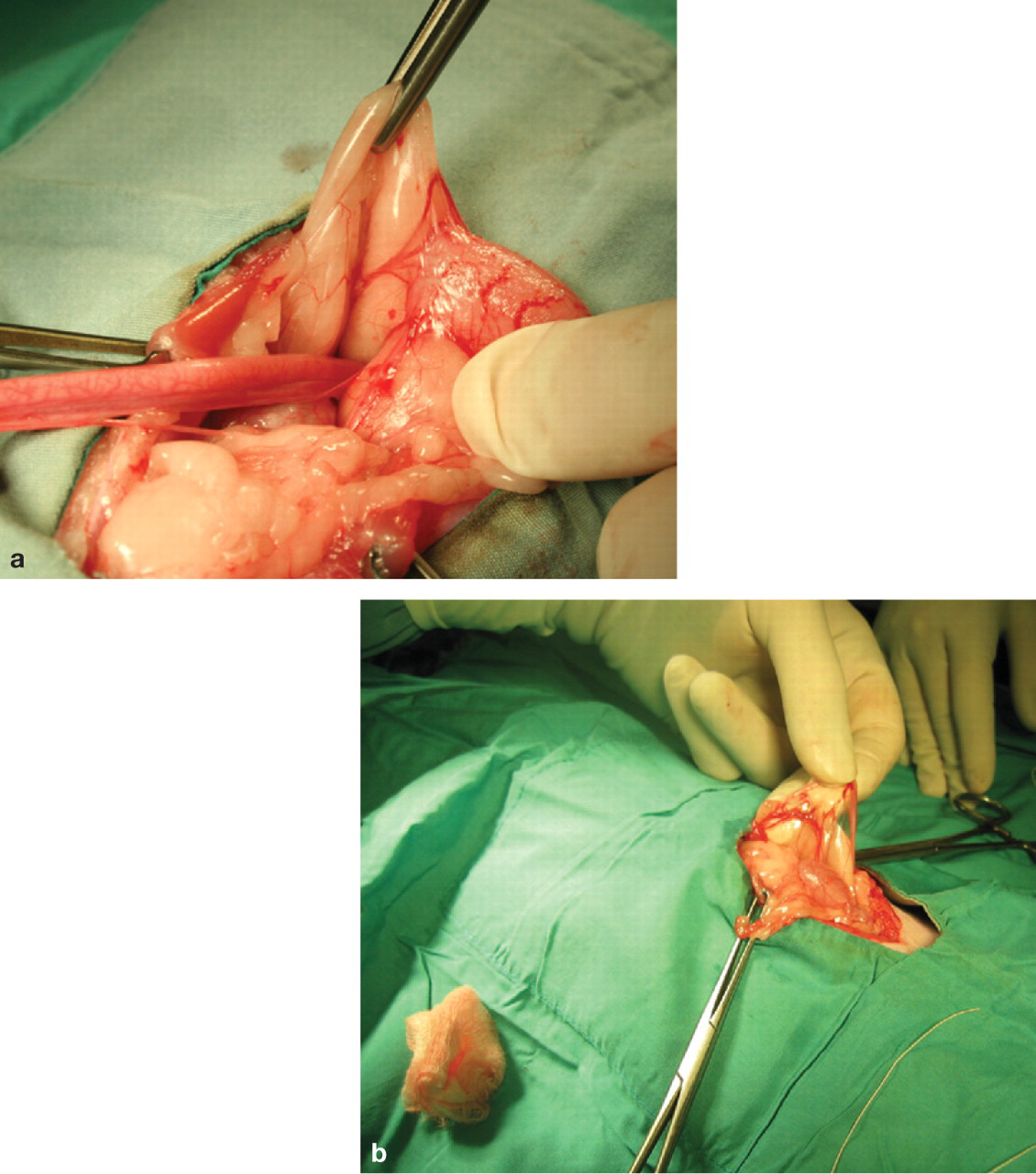
(a) Uterus unicornis discovered in a young queen at ovariohysterectomy. (b) Although one uterine horn may be hypoplastic or missing, the ipsilateral ovary is almost always present. Courtesy of Dr Jim Sweetman
When one normal uterine horn and ovary are present, the queen may have normal estrous cycles and may become pregnant. However, segmental aplasia may cause failure to conceive associated with fluid accumulation in the uterine lumen, depending on the location of lumen occlusion. 20,25
Ultrasonography may be a useful tool for diagnosis of uterine abnormalities in some infertile queens.
Cryptorchidism
The testes are normally descended into the scrotum by birth or shortly afterwards. The testes may move freely up and down in the inguinal canal prior to puberty, however. Cryptorchidism is failure of one or both testes to descend into the scrotum and remain there by 7–8 months of age. It is uncertain if cryptorchidism is linked to other congenital defects in cats.
The prevalence of cryptorchidism in cats has been reported as 1.3–3.8%, which is generally lower than the prevalence in dogs. 26–28 In one study of over 100,000 feral cats admitted to trap—neuter—return programs, 1.3% of male cats were cryptorchid. 29 In another study of over 5000 free-roaming cats admitted to a trap—neuter—return program, 1.9% of the males were cryptorchid. 30 In the author's practice, records of 4140 cats presented for castration over a 10-year period were reviewed. Seventy-two cats (1.7%) were identified as cryptorchid. Of the cats presented for castration, 10.5% were of a pedigree breed, with a total of 22 breeds represented. Among the pedigree cats, 6.2% were identified as cryptorchid. The highest incidence was in the Ragdoll breed (>18%).
Terminology
Cryptorchidism is the most common congenital defect of the feline urogenital system. The term ‘monorchid’ refers to total absence of one testis. Monorchidism is very uncommon in cats. Unilateral testicular agenesis has been reported, with the finding of a rudimentary spermatic cord and no associated testis. 26 The term ‘anorchid’ refers to the total absence of both testes, and is an exceedingly rare event.
Cryptorchid configuration
Most cryptorchids are unilateral (78–90%), with left and right sides equally affected. In one study where the location of the retained testis was recorded, 49% were inguinal, 33% were abdominal and 14% were within the inguinal ring. 26 In the author's practice, 87% of 72 cats had unilateral cryptorchidism and the most common configuration was the unilateral inguinal cryptorchid (51.6% of cases). Bilateral cryptorchids are likely to have abdominally retained testes. If one testis is in the scrotum, it may be difficult to determine if it is on the left or right side. Pushing the scrotal testis dorsally and cranially toward the inguinal canal can help determine its location. 31 It may be difficult to palpate an inguinal testis if the cat has large inguinal fat pads, unless the testis is located caudal to the fat pad. The inguinal lymph node and fat pad are commonly confused with inguinal testes on palpation.
Abdominally retained testes have been examined histologically and typically no sperm are found. The higher temperature inside the body suppresses development of sperm. Cats with retained testes located outside the abdomen, however, may be fertile. These testes produce testosterone so that affected cats have the typical male phenotype (thick skin on neck/shoulders, broad face) and behaviors (libido, aggression, urine marking, etc).
Confirmation of cryptorchidism
In one study, only 22% of cat owners were aware their pet was cryptorchid. 28 All male cats should be examined for cryptorchidism during wellness visits. If a retained testis is suspected, there are two ways to confirm the condition. The simplest is to check for testosterone-dependent penile spines (Fig 5). Penile spines will atrophy by 6 weeks following complete castration. Gonadotropin stimulation testing has also been used to detect retained testes. Testosterone levels fluctuate in the cat, so resting samples are not very informative and provocative testing must be used. Various protocols have been described, two examples of which are shown above right. Resting testosterone levels in intact male cats are <3.0 ng/ml. Provocative testing will induce a marked elevation of serum testosterone in the intact male.

Glans of the penis of (a) an intact tom cat with penile spines and (b) a castrated cat without penile spines
The mode of inheritance is suggested to be recessive and polygenic, and cryptorchid males should not be used for breeding. 26 Cryptorchidism is an example of a sex-limited trait: the trait is physically expressed only in the male even though it can be carried by females. Both the sire and dam of an affected cat should be considered to be carriers. Some full siblings of an affected cat will also be carriers. A reduction in the number of cryptorchid cats in a breeding program can be achieved by removing affected males and carrier parents from breeding. If the problem is widespread in a family line, full siblings of an affected cat should also be eliminated from the breeding program.
Protocols for provocative testosterone testing
Obtain baseline serum testosterone sample; administer 25 μg GnRH IM (Cystorelin; Merial); obtain second sample for testosterone concentration 1 h later
Obtain baseline serum testosterone sample; administer 250 IU hCG IM; obtain second sample for testosterone concentration 4 h later 32
Cryptorchidectomy
Testes that are palpable in the inguinal subcutaneous tissue can be removed via a simple incision. In other cases, a caudal midline incision and dissection deep to the inguinal fat pad is required. The external inguinal ring should be examined but care should be taken not to damage structures in the femoral triangle. For abdominally retained testes, laparotomy via a midline approach is required, although laparoscopic-assisted cryptorchidectomy has also been described. 33–35 Advantages of a laparoscopic technique over laparotomy include minimal invasiveness, reduced tissue trauma and, potentially, reduced postoperative pain and fewer complications. The principal disadvantage is the need for specialized equipment, with the associated costs and expertise required. Initially, the laparoscopic approach may take longer to perform than a traditional laparotomy until the practitioner gains experience with the technique.
Poor libido
Poor libido in the breeding tom cat is a common complaint and may be associated with a variety of factors. Successful breeding tom cats must be physically, socially and sexually mature. Ideally, a young inexperienced tom should be paired with a calm, mature and experienced queen. In some late-maturing breeds, libido cannot be assessed properly until 2–3 years of age.
Poor libido is often caused by management problems or underlying medical conditions. Investigation requires a thorough physical examination, a medical history and collection of a minimum database (complete blood count, serum chemistry, urinalysis and feline leukemia virus and feline immunodeficiency virus testing). Non-reproductive disease, such as dental disease or degenerative joint disease, may influence willingness or ability to mate. Chronic illness, such as upper respiratory tract infection or diarrhea, may lead to poor body condition and diminished libido.
Information should also be obtained on the cat's housing, diet (including nutritional supplements) and medications (both prescription and non-prescription). The tom cat's environment is very important for breeding success. It is preferable to bring the queen to the tom, as many toms will not breed successfully when outside their own territory. In pedigree catteries, tom cats may be housed separately in cages or enclosures because of urine marking behavior and to control reproduction. Tom cats often dislike changes to their territory, even changes in odor such as when scented cleaners are used. The enclosure for a breeding tom cat must provide enough space to allow for normal exercise. Cats value vertical space, so provision of areas to climb, or shelving, is very important. It also provides a way for the tom to retreat from the post-coital reaction of the queen to avoid being swatted. Inadequate housing may inhibit the breeding behavior of normal tom cats.
Measurement of baseline testosterone in tom cats with poor libido is not informative; provocative testing must be used (see discussion on diagnosis of cryptorchidism). Administration of supplemental testosterone in an attempt to correct poor libido is inappropriate. Exogenous testosterone may suppress release of GnRH and LH, thereby interrupting testosterone synthesis by the interstitial cells of the testes.
Surgical techniques for removal of abdominal testes have been described elsewhere. 31 Use of a spay hook to retrieve the vas deferens is not recommended because of the risk of damage to the ureters. 26 Abdominal testes are often located near the bladder (Fig 6), but can be present in the internal inguinal ring or in the inguinal canal. The best procedure is to find the vas deferens and follow it caudally to the testis. Applying gentle traction to the vas deferens may facilitate location of the testis by detecting its movement. While it can be frustrating trying to locate the retained testis in some cases, it is not appropriate simply to ligate the vas deferens and testicular vessels in the hope the testis will atrophy. It is possible for the blood supply to re-establish and the testis to remain functional.

The retained testis in cats with abdominal cryptorchidism is often found near the bladder