
Abstract


Onset — chronic and insidious
Road traffic accidents and falls are frequent causes of a variety of bone fractures, with the pelvic limb being commonly affected. 1,2 However, some feline fractures are not caused by traumatic incidents, and have a more chronic and insidious onset. Although fractures of the femoral head and neck can be caused by trauma, this review will focus primarily on spontaneous capital physeal fractures (also known as feline slipped capital physis or feline physeal dysplasia syndrome), and pathological fractures of the femoral neck secondary to metaphyseal osteopathy. These conditions have many features in common — not least that they affect young, male neutered, obese cats — and a clear differentiation between the two may be difficult.
Anatomy of the proximal femur
The proximal femur contains two growth plates: the capital physis and the growth plate of the greater trochanter. The former is responsible for approximately 30–40% of the longitudinal growth of the femur in small animals, while the latter contributes to normal development of the shape of the proximal femur but not to the length of the bone. 3 The capital epiphysis has a semicircular shape, and it articulates with the acetabulum to form the coxofemoral joint. The capital physis in the immature cat (and dog) has an L-shape contour that facilitates surgical reduction and stabilisation of capital physeal fractures and separations. This growth plate usually closes at 30–40 weeks of age in intact cats. 4
Blood supply to the femoral head in small animals depends on vessels forming an intra-articular subsynovial arterial plexus near the edge of the articular cartilage around the femoral head. This vascular ring is nourished principally by the lateral and medial femoral circumflex arteries, and to a much lesser degree by the caudal gluteal artery and iliolumbar artery. 5–7 This vascular network crosses the peripheral border of the physis to supply the capital epiphysis. 3 In cats under 7 months of age, a substantial blood supply to the femoral head epiphysis is provided by a vessel in the round ligament. 6
The growth plate
Histologically, the growth plate of normal immature cats contains several zones: 8,9
Image courtesy of Dr Andrew Pitsillides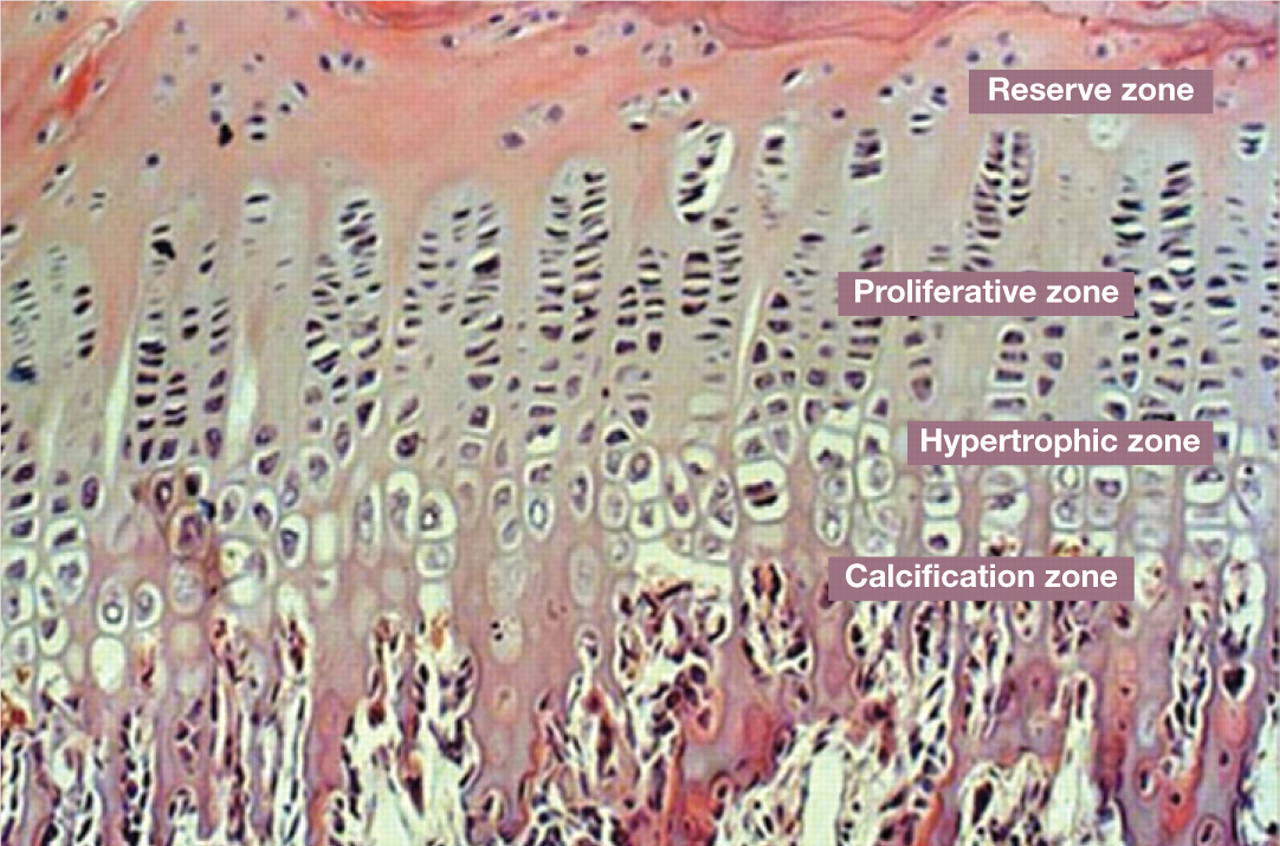
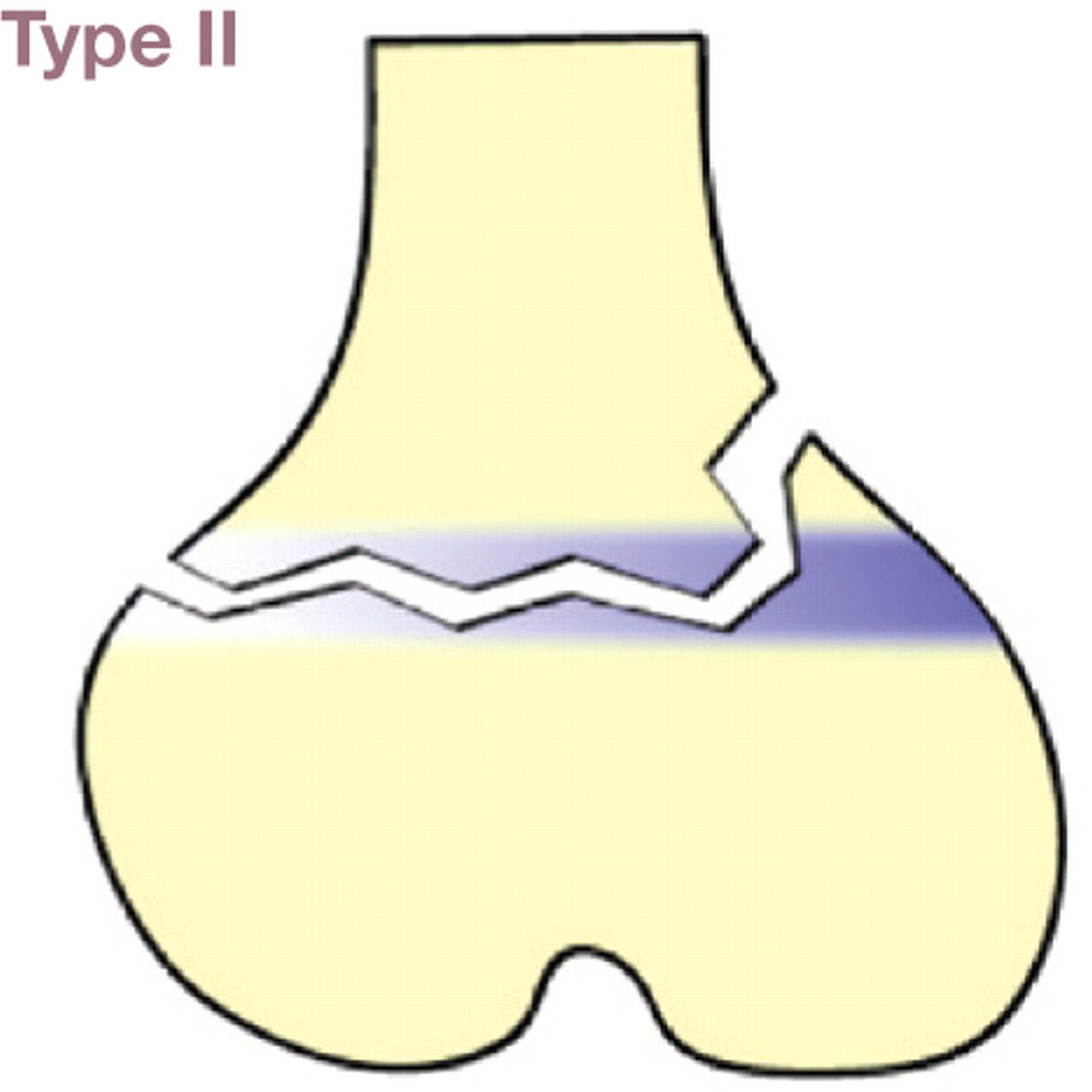
Salter-Harris classification of physeal fractures 9
Type I fractures involve separation of the epiphysis from the metaphysis at the growth plate, and frequently occur through the hypertrophic zone. These fractures are most common in the proximal humerus, and proximal and distal femur

Type II fractures occur through the growth plate and a corner of metaphyseal bone. A common presentation is in the proximal tibia
Type III fractures occur through the epiphysis and part of the growth plate, but the metaphysis is not affected. This type of fracture is an articular fracture and frequently affects the distal humerus

Type IV fractures run from the epiphysis through the growth plate and into the metaphysis. These are also articular fractures and occur in the distal humerus and femur

Type V fractures involve compression of the growth plate with end of growth potential. The distal ulna is the most common location for this fracture

Images by Dr Frank Gaillard (http://www.frankgaillard.com)
Non-traumatic conditions of the femoral head and neck
Spontaneous femoral capital physeal fractures
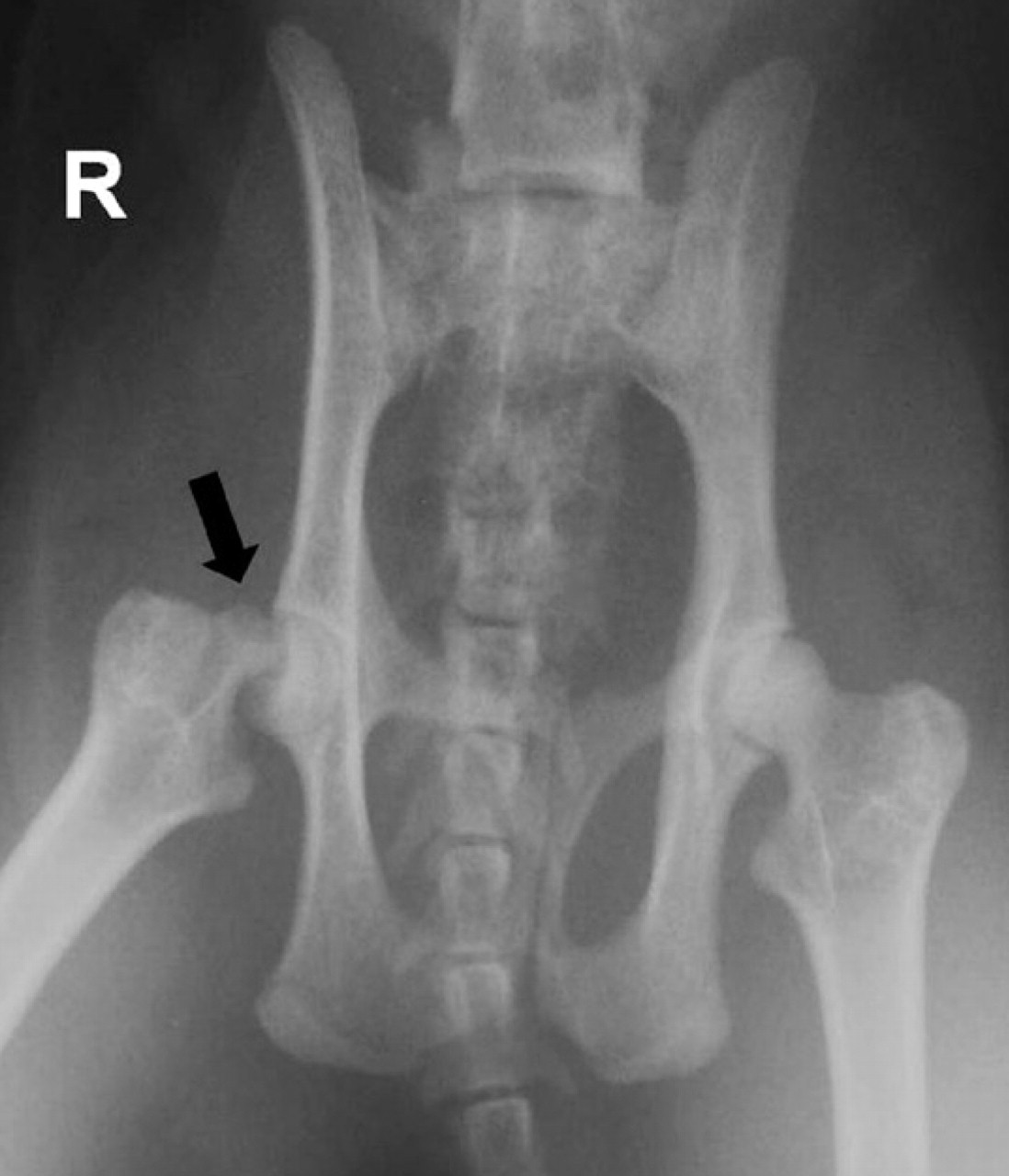
In the absence of a traumatic event (see box), fractures through the capital physis of the femur usually affect cats that are male neutered, obese and younger than 2 years of age, and they may be bilateral (Fig 1). 3,12–14 These cats generally present with acute or chronic hindlimb lameness and, of course, no history of trauma. The patient is usually reluctant to jump, and pain, decreased range of motion and crepitus can be observed on manipulation of the coxofemoral joint. While both hindlimbs may be affected simultaneously, a spontaneous fracture may develop in the contralateral limb later on. Radiographic study of the affected coxofemoral joint reveals displacement of the femoral epiphysis in relation to the metaphysis. This incongruency is best visualised when radiographs are taken with the limbs in a ‘frog-legged’ position, as the joint capsule is not tightened and thus the fracture is not reduced into position.

Ventrodorsal radiograph of the pelvis of a young cat with bilateral spontaneous capital physeal fractures (arrows). Courtesy of Dr Silke Stein
McNicholas and coworkers identified four risk factors in the development of spontaneous femoral capital physeal fractures: 14
Traumatic fractures
As with any other bone fracture, feline femoral neck fractures may be sustained during a traumatic incident. Young (between 7 months and 2 years of age) male cats and non-pedigree cats are at particular risk of being involved in road traffic accidents. 10 The growth plate is a weak area through which fractures may occur in growing animals. Interestingly, however, it has been reported that cats under 6 months of age suffer fractures of the femoral neck more frequently than fractures through the physis. 11 The authors of that study hypothesised that growth plates in these young cats could be stronger than immature bone.
Ventrodorsal radiograph of the pelvis of a 12-month-old cat, revealing a traumatic fracture of the neck of the femur and avulsion of the greater trochanter

The case history generally includes a traumatic event, so a complete general physical examination is required to evaluate if the patient is stable. These cats usually present with unilateral hindlimb lameness, pain and crepitus on manipulation of the affected coxofemoral joint. Radiographic evaluation of the joint reveals a fracture through the capital physis or femoral neck, depending on the age of the cat. 11
It has been reported that neutering causes a delay in growth plate closure not only at the femoral capital physis, but also in other locations. 15,16 Other physes have indeed been found to remain open in cats with slipped capital physis. 7 Testosterone and oestrogen facilitate cartilage maturation in the growth plate, so a reduction in the levels of these hormones leads to a delay in physeal cartilage-maturation and closure. 15 However, the age at which neutering is performed does not seem to influence the degree of growth plate closure, as no difference was found between cats neutered at 7 weeks and 7 months of age. 16
Open growth plates are areas susceptible to fracture. When the growth plate of cats with slipped capital physis was evaluated histologically, it was observed that the physis was almost double the size of a normal growth plate, and that the chondrocytes were irregularly distributed in clusters; necrosis was also present. 12,13 Some authors have reported this pathology in the growth plates of pigs, as a form of osteochondrosis. However, the feline presentation is different as it diffusely affects the entire physis and the chondrocytes lack the normal columnar distribution typical of growth plates. 12
Feline capital physeal fracture is similar to the pathology suffered by obese, human male adolescents with spontaneous slipped femoral capital physis.
Metaphyseal osteopathy
Metaphyseal osteopathy affects young, male neutered, obese cats, and the history and clinical signs are similar to those associated with spontaneous capital physeal fracture. Radiographically severe bone lysis and remodelling are observed in the femoral neck. Pathological fractures through the capital physis can frequently be seen.
Histopathological evaluation of the femoral heads and necks of cats diagnosed with feline metaphyseal osteopathy has shown focal irregularity with thickening and splitting of the articular cartilage. The aetiopathogenesis is not completely understood, as either an increase or decrease in vascularisation in the metaphysis could lead to necrosis, collapse and fracture of the femoral neck (the latter scenario similar to Legg-Calvé-Perthes disease of the femoral head in dogs). 17 Radiographically, loss of definition and areas of radiolucency can be observed in the femoral neck (Fig 2). 17

Ventrodorsal radiograph of the pelvis of a 2-year-old male neutered cat. There are areas of radiolucency in the proximal metaphysis of both femurs and separation of both femoral capital epiphyses. Reproduced from Queen J, Bennett D, Carmichael S, et al, Veterinary Record, Vol 142, pp 159–62, with permission from BMJ Publishing Group Ltd
It is unclear whether metaphyseal osteopathy is a pathology in itself, or a consequence of primary fracture and subsequent bone remodelling. Queen et al 17 reported 17 cats with radiographic changes consistent with metaphyseal osteopathy. These animals presented a subtle lameness that progressed to an acute worsening in the clinical signs several weeks later. The authors discussed the possibility that the radiographic changes observed could be associated with secondary bone remodelling after femoral neck fracture, avascular necrosis similar to Legg-Calvé-Perthes disease in dogs, or metaphyseal osteomyelitis. However, the age of the cats (most were older than 1 year old) and clinical presentation (chronic and then acute worsening, possibly due to fracture of the bone) led them to conclude that this was a primary disease of the feline metaphysis giving way to a secondary fracture of the femoral neck, rather than vice versa. In contrast to Legg-Calvé-Perthes disease in dogs, the epiphysis is not affected in cats, which might be explained by the increased blood supply to that area through the round ligament in cats, compared with dogs.
As Pérez-Aparicio and Fjeld reported in 1993, 11 some femoral neck fractures can heal spontaneously with conservative treatment. However, they also observed that some femoral neck fractures and all capital physeal fractures did not heal and developed hypertrophic pseudoarthrosis with time. Similarly, McNicholas et al, 14 in a report of 26 cats with spontaneous capital physeal fractures unrelated to trauma, observed radiographic changes in the femoral neck (osteolysis and sclerosis) secondary to the femoral fracture. The fact that the severity of these changes increased with increased duration of the clinical signs, suggested to them that the femoral neck osteolysis and sclerosis were secondary changes.
Therefore, it remains unclear whether the changes seen in the femoral neck are primary or secondary in nature.
Diagnosis
The clinician needs to include fractures of the femoral head and neck among the differential diagnoses for any young feline patient with hindlimb lameness/weakness, whether or not associated with a traumatic event. Following complete orthopaedic examination to rule out other processes, such as cruciate ligament rupture, which are not as obvious as traumatic bone fractures, careful manipulation of the hip is necessary to determine the origin of the pain. Crepitus, pain and decreased range of motion can be elicited during manipulation of the affected hip; if there is chronicity, muscle atrophy may also be evident.
Radiographs of the pelvis and coxofemoral joint are essential in the diagnosis of these pathologies. A minimum of a lateral view and a ventrodorsal projection with the limbs in extension (Fig 3) should be obtained. However, sometimes the extended ventrodorsal radiograph of the hips in cats with spontaneous capital physeal fractures may not show any obvious abnormalities. As mentioned earlier, the collagen fibres of the joint capsule become tightened during extension of the limb, which reduces the fracture and prevents its visualisation. To avoid this problem and facilitate observation of the fracture, a frog-legged view should be taken (Fig 4). 18 Positioning the patient in dorsal recumbency and allowing the limbs to abduct freely obtains this projection. A clear displacement of the femoral capital epiphysis can be seen in some cases; in others, only a minimal step between the epiphysis and metaphysis is observed.
Ventrodorsal radiograph of the pelvis of an 18-month-old cat. A capital physeal fracture is seen in the right femur (arrow)

Postoperative ventrodorsal frog-legged radiographic view of the pelvis of a cat with left capital physeal fracture and avulsion of the greater trochanter. K-wires have been placed to stabilise the capital physeal fracture and a tension band (K-wires and cerclage wire) has been used to stabilise the avulsion fracture of the greater trochanter. This projection helps to visualise the level of penetration of the K-wires in the epiphysis
Treatment approaches
While treatment of proximal femoral fractures can potentially be achieved by conservative (see box) as well as surgical methods, surgical treatment is recommended in the majority of cases to avoid the risk of non-union and dysfunction. In most cases of capital physeal fracture treated conservatively, hypertrophic pseudoarthrosis and osteophytosis ensue, which may lead to dysfunction. In cats younger than 3 months of age with femoral neck fractures, spontaneous healing may, however, occur. 11
Conservative treatment
This modality relies on natural body mechanisms to heal the fracture, so might potentially be appropriate for young cats with acute fractures of the femoral neck that present with no bone lysis or remodelling. If metaphyseal osteopathy is suspected radiographically, conservative treatment is unlikely to resolve the clinical signs.
Conservative treatment includes exercise restriction and analgesia. Ideally, cats should be confined to a crate or small room for at least 4 weeks, to allow healing of the fracture. Several daily supervised walks outside the crate are recommended to prevent muscle atrophy in the affected limb. Analgesia can be provided in the form of non-steroidal anti-inflammatory drugs (NSAIDs; eg, meloxicam) or opioid derivatives (eg, tramadol). Clinical evaluation of the patient and radiographs of the hip joint should be performed 4 weeks after the start of treatment to assess patient progress and fracture healing, and determine if normal activities can be progressively resumed or, conversely, whether surgical excision of the femoral head and neck would be more beneficial.
Surgical stabilisation with K-wires
The objective of surgical stabilisation with K-wires is to preserve the normal anatomy and function of the coxofemoral joint. This prevents side effects associated with salvage procedures: namely, muscle atrophy, decreased range of motion (especially in extension) and shortening of the limb. 6 However, due to the intra-articular nature of this type of fracture, osteoarthritis, and, therefore, secondary chronic pain and decreased range of motion, could develop with time.
Reduction and stabilisation of femoral head and neck fractures can be attempted if the fracture is acute and there are no signs of bone remodelling. Surgery should be carried out as soon as possible to minimise any impact on growth potential and changes in the femoral neck that could compromise fracture stability and healing. 3 This technique is not recommended in cats diagnosed with metaphyseal osteopathy.
Technique 3,18–21
It is important to aseptically prepare the entire affected limb to allow manipulation of the leg during surgery. The limb is clipped from the dorsal midline to the tarsus, and scrubbed for 5 mins with an antiseptic such as clorhexidine. Likewise, the complete limb is draped to allow intraoperative manipulation of the leg, which is essential for adequate visualisation of the fracture during surgery.
Craniolateral approach
A craniolateral approach to the hip is performed with the cat in lateral recumbency. 21 The joint capsule is incised in a T-shape and elevated from the femoral neck. Partial tenotomy of the deep gluteal and vastus lateralis muscles is helpful in exposing the femoral head and neck.
The capital physis has an L-shape that provides good stability following reduction. However, the capitus is usually rotated in relation to the neck and retained in the acetabulum by the round ligament (Fig 5). Reduction of the fracture might be accomplished by application of medial pressure from the femur through the fractured physis, while flexing and extending the hip. This will usually cause the epiphysis to de-rotate and lock in place. The L-shape of the fractured physis will help in achieving a correct reduction and prevent reluxation if pressure is applied through it. Alternatively, the tip of a small diameter K-wire may be used to de-rotate the epiphysis by walking it along the articular cartilage, taking care to avoid any damage. Once the fracture has been reduced in the correct position, pressure is applied from lateral to medial. The K-wires used to stabilise the fracture can be placed in a normograde or retrograde fashion. It is helpful to measure the depth of the epiphysis in preoperative radiographs to determine the distance the wires need to be drilled in, to avoid damage to the articular cartilage.

Intraoperative view of a capital physeal fracture (arrow), with separation of the epiphysis from the metaphysis. Courtesy of Dr Silke Stein
DECISION-MAKING: Surgical stabilisation
Open reduction and stabilisation of a capital physeal fracture with K-wires needs to be undertaken as soon as possible (in the first 3–4 days) to minimise alterations in vascularisation of the epiphysis and remodelling of the metaphysis. Chronic fractures, in which bone remodelling can already be visualised radiographically or intraoperatively, are best managed with femoral head and neck excision.
It has been reported that parallel K-wires are biomechanically superior to divergent wires, 22 so an effort must be made to place the pins parallel to each other and to the femoral neck. Specially designed drilling guides to allow parallel drilling are available (Fig 6).

Drill guide that facilitates parallel placement of K-wires from the base of the third trochanter into the epiphysis of the femoral head
Once the fracture has been reduced and stabilised, the joint is manipulated to check stability and any potential impingement of the implants. The joint capsule is closed with absorbable suture (eg, 3/0 PDS [polydioxanone]) in a cruciate pattern. The tenotomised muscles are repaired with absorbable suture (eg, 3/0 PDS) in a cruciate or mattress pattern. Closure of the rest of the soft tissues is routine.
Ventromedial approach
A ventromedial approach to the hip and stabilisation with two K-wires has also been described. 23 This approach requires dissection between the iliopsoas and adductor longus muscles and subtotal pectinectomy. Once the fracture has been reduced by distal distraction of the femur site, the K-wires are placed from the articular cartilage through the physis into the femoral neck.
A ventral approach to the hip permits better visualisation of the articular surface of the epiphysis, due to the presence of a ventral notch that interrupts the acetabular rim. A K-wire is placed in the fovea capitis femoris and drilled towards the third trochanter. A second K-wire is inserted cranial to the first one and directed caudally to cross the first wire. The K-wires are retracted, cut short and countersunk below the level of the articular cartilage, which is essential to preserve joint function. According to the authors who described this approach, its advantages are that it minimises soft tissue and vascular damage, and allows direct visualisation of the fracture. 23 However, the ventral approach to the coxofemoral joint is not frequently used and it can be challenging for a surgeon unfamiliar with it.
Irrespective of the surgical approach, radiographs should be taken postoperatively to assess adequate placement of the K-wires and penetration of the epiphysis without protrusion into the joint. A frog-legged view is best for evaluating this (Fig 4). If suboptimal placement of the K-wires is suspected (intra-articular, not deep enough in the epiphysis, protruding from the femoral neck, etc), additional views, including fluoroscopy, can be performed to try to determine the exact position of the implants and decide whether further action is needed. If only one wire is adequately engaging the epiphysis, for example, a second wire should be inserted to prevent rotation and instability of the fragment.
Postoperative care
The patient should be kept hospitalised with injectable analgesia to cover the first 24–48 h postoperatively. Opioids (buprenorphine: 0.03 mg/kg IV q6–8h) and NSAIDs (meloxicam: 0.2 mg/kg SC first dose, then 0.05 mg/kg PO q24h) make a good analgesic combination. Once the patient is discharged, the low dose of meloxicam can be administered at home for 4 days.
Physiotherapy is important during the postoperative period if the cat tolerates it. Cold packs applied over the operated hip for the first 48 h after surgery help reduce inflammation and pain. After this period, the owner can apply warm packs and perform gentle passive range of motion exercises several times daily until the cat is consistently using the operated limb. Bandages, such as Ehmer or 90 degree bandages, are not well tolerated by cats; furthermore, they would not allow physiotherapy, which is essential to recover joint range of motion and muscle volume. They are not needed if adequate exercise restriction is instituted.
The patient's activity level is restricted for 4–6 weeks postoperatively, either by confining the cat to a big crate or to a small room from which any furniture the cat might be tempted to jump onto/from has been removed. If using a crate, several short daily supervised walks outside the crate are recommended to prevent muscle atrophy of the operated limb. The activity level can be progressively increased, provided the cat is progressing adequately and the recheck radiographs (usually taken 4 weeks after surgery) show good bone healing and stable implants.
Femoral head and neck excision
Femoral head and neck excision allows the formation of a pseudoarthrosis (fibrous false joint) in the hip. By avoiding bony contact between the femur and the pelvis, pain is eliminated. However, limb shortening and a decreased range of motion is to be expected, so some degree of gait abnormality may persist after this surgery. 3,20 Mild muscle atrophy is also to be expected, especially in chronic cases. Femoral head and neck excision is a salvage procedure and irreversible — ideally, the joint should be preserved if at all possible.
DECISION-MAKING Femoral head and neck excision
Although performing a salvage procedure of the femoral head and neck (femoral head and neck excision) is a quick and easy approach, which usually leads to adequate limb function in the patient, preserving the coxofemoral joint should be attempted when no bone lysis/remodelling is seen.
Technique 3,20,21
Aseptically prepare the entire affected limb, as it will need to be manipulated during surgery to enable an adequate ostectomy in the femoral neck. A craniolateral approach to the hip is performed with the cat in lateral recumbency. The joint capsule is incised in a T-shape and elevated from the femoral neck. Partial tenotomies of the deep gluteal and vastus lateralis muscles are helpful in exposing the femoral neck. A periosteal elevator may be used to help elevate the vastus lateralis muscle from the neck of the femur. Placement of a Gelpi retractor greatly improves visualisation of the joint.
The round ligament is cut and the femoral epiphysis removed with forceps. The landmarks to perform an adequate ostectomy in the femoral neck are the medial aspect of the greater trochanter laterally, and the lesser trochanter medially (Fig 7). In cats, the lesser trochanter may be difficult to palpate during surgery given its small size, but having radiographs of the extended pelvis to hand might be helpful in determining the approximate location of this structure. Complete removal of the lesser trochanter should be avoided whenever possible, as it is the insertion of the iliopsoas muscle, an important flexor of the hip.

Postoperative ventrodorsal radiograph of the pelvis after femoral head and neck excision. The ostectomy is performed between the medial aspect of the greater trochanter (white arrowhead) and lesser trochanter (black arrow), without removing either trochanter
In a transverse plane, the ostectomy should not be performed perpendicularly to the femoral neck, as this would create a spike in the caudal aspect of the femur that could be a cause of discomfort for the patient. Rather, the limb is externally rotated so that the patella is oriented towards the ceiling and the cut is performed perpendicularly to the operating table. It is useful to mark the cutting line in the bone with electrocautery, between the landmarks described above, to help guide the ostectomy (Fig 8).

Intraoperative view showing the line of an ostectomy. The limb is externally rotated 90° to make the cut. The patella (circled) should be pointing at the ceiling and the ostectomy performed between the medial aspect of the greater and lesser trochanters (dashed line). No irregularities or spikes should be felt on the surface of the cut
Once the ostectomy has been performed and the head and neck of the femur removed, it is important to check for any irregularities in the surface of the cut and eliminate them with rongeurs or files. The limb is then moved into a normal position and the joint manipulated to check for any impingement or rubbing of bone on bone. Although this manipulation should be in all directions, flexion and extension are the normal movements during walking, and lack of impingement in this plane is the most relevant for a successful outcome.
The joint is lavaged prior to closure in order to remove debris. Closure of the joint capsule is important to add stability to the false joint just created. Absorbable suture (3/0 PDS) is used in a simple interrupted or cruciate pattern. The tenotomised muscles are repaired with absorbable suture (3/0 PDS) in a cruciate or mattress pattern. The rest of the soft tissues are closed in a routine manner.
Radiographs should be taken postoperatively to ensure an adequate ostectomy, with complete removal of the femoral head and neck. Positioning the hip in extension allows better evaluation of the cut (Fig 7).
Postoperative care
Analgesia, especially for the first 48 h after surgery, is essential to encourage early use of the operated limb. The same analgesic protocol as described for surgical stabilisation of a physeal fracture can be used (opioids and NSAIDs). Once the patient is discharged, the low dose of meloxicam can be administered at home for 4 days.
Physiotherapy is important during the postoperative period if the cat tolerates it. Cold packs applied over the operated hip for the first 48 h after surgery help reduce inflammation and pain. After this period, the owner can apply warm packs and perform gentle passive range of motion exercises several times a day until the cat is consistently using the operated limb. Bandages should not be applied after this type of surgery. Exercise is controlled by restricting the cat to a small room for 2 weeks; thereafter progressive access to the rest of the house is allowed to encourage use of the operated limb and improve joint range of motion.
Early detection of pain is essential to prevent a vicious cycle leading to limb disuse and muscle atrophy.
Total hip replacement
Total hip replacement (THR) is widely performed in large-breed dogs with end-stage coxofemoral osteoarthritis that is non-responsive to medical treatment. It has also been described as a treatment for cats with capital physeal fractures, as a micro-THR system has been developed for use in small dogs and cats. 24 The recovery of the cats included in this report after THR was excellent, based on clinical parameters such as muscle mass, coxofemoral range of motion, gait and the owner's subjective assessment. The surgery, however, is technically demanding, requires advanced training and considerable financial investment. A description of the technique can be found in the above-mentioned report. 24
Outcome
Cats undergoing open reduction and stabilisation of femoral head and neck fractures with K-wires have a good to excellent prognosis. 3,18–20,25 Surgery preserves the anatomy and function of the coxofemoral hip, avoiding complications derived from more aggressive techniques. However, on occasion, an ‘apple core’ appearance of the femoral neck is observed radiographically during postoperative rechecks. This is an indication of changes in vascularisation and osseous remodelling. Removal of the implants when the fracture has healed resolves these changes. 3,25 As capital physeal fractures are intra-articular fractures, osteoarthritis may develop in the operated joint. Depending on the degree of degenerative changes, patients may show clinical signs secondary to this pathology later in life.
A good to excellent outcome has been reported in most studies of cats after femoral head and neck excision. 26 However, mild lameness, shortening of the limb, decreased range of motion or pain on manipulation of the hip occur in some cases. An unsatisfactory outcome is usually due to incomplete removal of the femoral neck, which causes painful rubbing against the acetabulum (Fig 9). It has been reported that the duration of clinical signs before surgery influences outcome, with animals exhibiting clinical signs for longer than 6 months having a poorer outcome. 27

Ventrodorsal radiograph of the pelvis in a cat that had previously undergone incomplete excision of the femoral head and neck. Orthopaedic examination revealed pain, crepitus and severe muscle atrophy. The recommended line of the ostectomy is revealed by the dashes
Case notes

Answers and discussion
Radiographic diagnosis There is a fracture in the neck of the left femur (radiograph a).
Radiolucency, remodelling and narrowing of the left femoral neck can also be observed. (These changes are suggestive of underlying metaphyseal osteopathy or bone remodelling secondary to the neck fracture.) Muscle atrophy of the left hindlimb is visible.
MULTIMEDIA
Two video recordings of the cat, one at presentation and one post-surgery, are included in the online version of this article at
KEY POINTS
Footnotes
Acknowledgements
The author would like to thank Dr Silke Stein for providing some of the images.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.