
Abstract
Hypertrophic cardiomyopathy (HCM) was first reported as a clinical cardiac condition in cats in the 1970s. 1 Today, HCM is the most common adult-onset cardiac disease in cats, with some estimates of prevalence approaching 20%. 2,3 Sequelae of HCM range from lifelong subclinical disease to sudden death, congestive heart failure (CHF) and cardiogenic aortic thromboembolism (ATE). 4 Studies of natural history of the disease suggest a median survival in cats initially presenting with subclinical disease of approximately 4 years. This statistic cannot, however, be used to predict the disease course for any individual patient as the rate of progression, severity of disease and potential for the disease to progress are highly variable. 4,5
Despite substantial progress in diagnosis, categorization and etiology of feline HCM, 6–18 little evidence exists regarding efficacy of therapy for HCM at different stages of disease, 19–27 and no therapies for feline HCM have been critically evaluated in large randomized controlled trials.
Commonly described therapies for HCM include diuretics, angiotensin-converting enzyme inhibitors (ACEIs), calcium-channel blockers and beta-blockers. 4,25,26,28–30 However, most of these have not been rigorously evaluated in cats with HCM. One study suggested no benefit of any therapy other than furosemide, and potential harm of administering β-blockers in cats with CHF secondary to diseases with diastolic dysfunction. 31 No studies have evaluated the clinical outcomes of treating subclinical HCM in terms of disease progression or survival, although one study found no change in left ventricular wall thickness or diastolic function in Maine Coon cats with subclinical HCM over a 12-month period of ramipril administration. 19,32
Similarly, no randomized controlled studies have evaluated the outcome of prevention of ATE (either as a first event or recurrence). The Feline Aortic Thromboembolism — Clopidogrel vs Aspirin Trial (FATCAT) is currently evaluating the effect of clopidogrel or aspirin on recurrence of ATE in cats with prior ATE and HCM. 33 Some investigators have examined the ability to reduce dynamic left ventricular outflow tract (LVOT) obstructions in subclinical HCM, although the clinical implications of such interventions have not been defined or examined. 34,35
Thus, demonstrated benefit of most current therapies for HCM in cats is absent from the literature. Under a standard classification system of scientific clinical evidence, most therapy for HCM falls into the lowest category or level of evidence — benchtop science, theoretical benefits and personal observations. 36 Nevertheless, review papers, textbook chapters and continuing education presenters often suggest therapies for cats with either sub-clinical or clinical HCM, despite a lack of published evidence of efficacy or safety. 25,26,28,37–55
Our hypothesis was that cardiologists do not base their treatment of HCM on credible clinical science that examines patient-oriented outcomes, because such scientific data are lacking. This article collates the published literature evaluating therapy of feline HCM, contrasting this with self-reported treatment strategies chosen for hypothetical cases of HCM by board-certified veterinary cardiologists, cardiology residents and veterinarians with an interest in cardiology.
Materials and methods
Survey of cardiologists
A survey examining treatment strategies for HCM was conducted online in April 2006 through the Veterinary Information Network. A link to the survey was sent via email to 342 members of the American College of Veterinary Internal Medicine (ACVIM) cardiologist listserve. This listserve includes all ACVIM and European College of Veterinary Internal Medicine (ECVIM-CA) certified cardiologists, all UK diplomates in cardiology, all ACVIM and ECVIM cardiology residents and candidates, and approximately 150 veterinarians with an expressed interest in or focus on veterinary cardiology.
Respondents were asked to identify their level of cardiology training (diplomate, post-residency candidate, resident, practitioner with or without interest in feline cardiology, practice limited to cardiology [non-certified], American Board of Veterinary Practitioners [ABVP] certified in feline medicine, UK certificate in cardiology, other).
The survey provided 12 case scenarios of HCM of increasing complexity and severity. Seven scenarios were for cats with subclinical disease and five were for cats with clinical signs. Full details of each scenario are provided in Table 1. For each scenario we asked the clinician to identify therapy that they would prescribe for the ‘typical cat presenting to them with these findings’ to determine ‘standard’ therapeutic decisions.
Case scenarios for the HCM survey
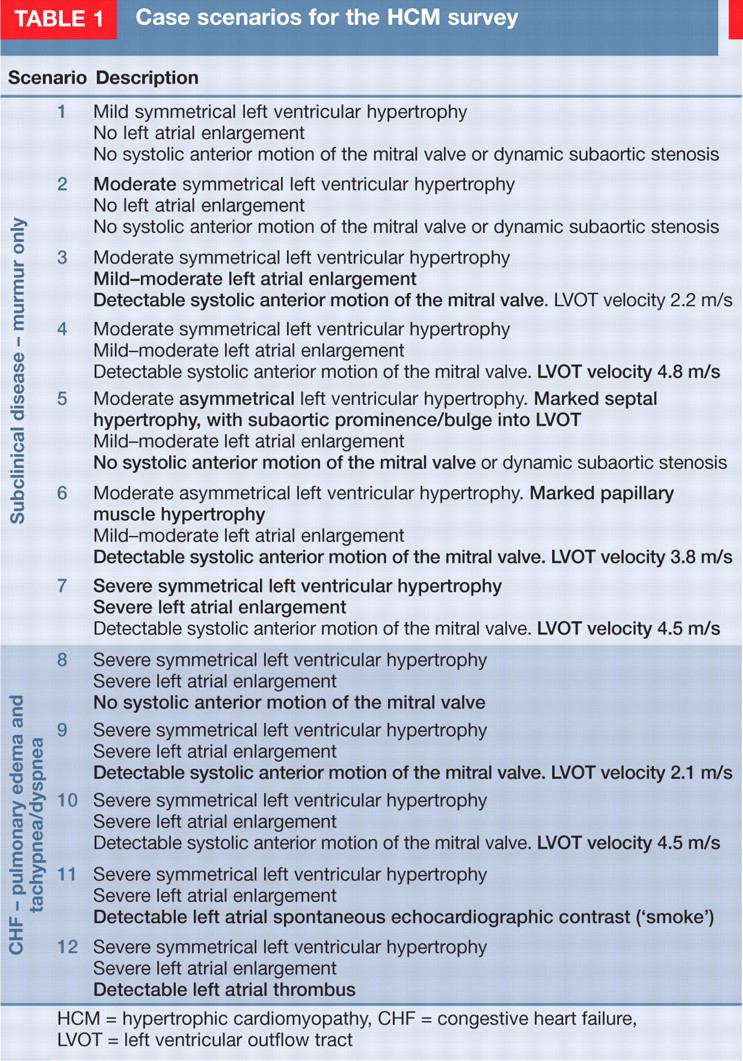
HCM = hypertrophic cardiomyopathy, CHF = congestive heart failure, LVOT = left ventricular outflow tract
Treatment options for each scenario
None
Lasix
ACEI (any kind)
Diltiazem (short- or long-acting)
β-blocker (any kind)
Aspirin
Low-molecular weight heparin
Heparin (unfractionated)
Clopidogrel
Amlodipine
Holistic/alternative
Hospitalization
The web-based survey system randomly assigned respondents to one of two groups (group A or group B) as they began taking the survey. Randomization of the survey was performed using a random-number generator that was coded into the survey system. The case scenarios (Table 1) and treatment options (see box left) provided to each group for each case scenario were identical. In addition to selecting the treatment options they would consider for each case scenario, each respondent was asked to select justification options for their chosen treatments for two of the 12 case scenarios presented (see box on page 489). Group A was asked to provide justification for their therapeutic choices for scenarios 1 and 7, and group B was asked to provide justification for their therapeutic choices for scenarios 4 and 12. We hypothesized that being asked to provide justification for treatment choices would impact the choices made. Randomizing the survey among respondents would allow an unbiased comparison of treatment choices between the two groups.
We did not directly ask whether specific therapeutic interventions were aimed at preventing disease progression or reducing the risk of ATE. However, when non-antithrombotic therapy (ie, furosemide, ACEIs, diltiazem [short or long acting], β-blockers, amlodipine) was selected for scenarios 1–7 (subclinical disease) in any combination, we assumed that this was done in order to affect disease progression (either myocardial remodeling or development of CHF); and when antithrombotic therapy (ie, clopidogrel, aspirin, low molecular weight heparin [LMWH] or unfractionated heparin) was selected for any scenario in any combination, we assumed this was done to reduce the risk of ATE.
Literature search
On March 17, 2006, shortly before releasing the survey to participants, we conducted a literature search on PubMed for published articles related to feline cardiology. We used four different search criteria. First, we compiled a list of all veterinary journals indexed on PubMed. These journal titles were included in the search term as an ‘
All veterinary journals (171)
All veterinary journals (171)
Next, we created a search string of all members of the cardiology listserve (author[AU]
Authors (377)
Authors (377)
Additionally, we examined the list for potentially excluded journals and searched those individually using CAB abstracts using the search term ‘hypertrophic cardiomyopathy’.
The search results were combined and duplicates and non-relevant citations were excluded. Excluded citations pertained to hemodynamic effects of anesthetic agents, cardiopulmonary resuscitation, or in vitro experiments utilizing feline myocardium as a model. We then identified all citations related to feline HCM or ATE. These were further classified in three ways. First, we identified the purpose or intent of the article (diagnosis, pathophysiology, anatomy or pathology, treatment or review). Next, we classified those citations addressing treatment according to evidence-based medicine criteria for levels of evidence. 36 Finally, we classified the citations as being either ‘disease-oriented outcomes’ or ‘patient-oriented outcomes’. 37
Justification options
Justification was sought for treatments selected and treatments not selected
Reasons FOR using
Favorable personal experience
Probably doesn't hurt and might help
Recommendation from specialist consultant or continuing education presenter for use
Consensus of peers for use
Clinical study in cats showing survival or disease progression benefit
Clinical study in other species (including humans) showing survival or disease progression benefit
Research showing physiological response in cats or other species (including humans)
Research suggesting theoretical benefit in cats or other species (including humans)
Textbook recommendation
Reasons FOR NOT using
Unfavorable personal experience
Recommendation from specialist consultant or continuing education presenter against use
Consensus of peers against use
Clinical research showing lack of benefit in cats or other species (including humans)
Clinical research showing adverse outcome in cats or other species (including humans)
No evidence showing benefit with regard to survival or progression in cats
Not a logical choice in this scenario
No experience with this treatment in this condition
Analysis
We performed descriptive analysis of the survey results. We compared use of β-blockers in scenarios where systolic anterior motion of the mitral valve was present versus those where it was not with a Cochran's Q test, which compares proportions for k related samples. Differences were considered significant if P < 0.05.
Results
Ninety-eight respondents (29% of listserve) completed the survey (demographics are presented in Table 2). There were no apparent differences in responses between cardiology diplomates and non-diplomates or non-cardiology diplomates. For any given question, at least 88 responses were available for analysis.
Demographics of survey respondents

UK certificate holders in cardiology or non-cardiology diplomates (eg, internal medicine)
Scenarios 1–7 described patients with sub-clinical disease (murmur but no evidence of CHF or dyspnea/tachypnea). For scenario 1 (extremely mild or equivocal disease), 84% (82/98) of respondents reported that they would not prescribe any pharmacotherapy. Of the 16% (16/98) prescribing medications, all chose ACEIs, diltiazem and/or β-blockers, with 6/16 choosing more than one drug. When presented with scenario 2 (slightly more apparent left ventricular [LV] thickening), 44% (42/96) of respondents indicated that they would prescribe ACEIs, diltiazem and/or β-blockers, and 11 of the 42 chose more than one drug. Approximately 77% (73/95) of respondents stated that they would prescribe one or more drugs by scenario 3 (some left atrial [LA] enlargement and mild dynamic LVOT obstruction): approximately 50% would prescribe β-blockers, 25% an ACEI, 10% diltiazem, and 20% would prescribe aspirin or clopidogrel. Of those prescribing pharmacotherapy at this stage, 47% (33/71) stated that they would prescribe more than one drug. In response to scenario 4 (same as scenario 3 but more severe LVOT obstruction), 90% (83/92) of respondents indicated that they would prescribe pharmacotherapy, with 94% (78/83) of these prescribing a β-blocker. By scenario 7 (severe subclinical disease, with marked LA enlargement and severe LVOT obstruction), 98% (89/91) of respondents indicated that they would administer some sort of therapy, with 84% (75/89) selecting to administer antithrombotic therapy — 66% (59/89) would administer aspirin, and 33% (29/89) would administer clopidogrel or LMWH.
Once CHF was presented as part of the scenario (scenarios 8–12), 100% of respondents stated they would routinely administer furosemide, with or without other therapeutic agents.
Overall, as the complexity of the scenario increased, there was a proportional increase in both the number of respondents stating they would administer some sort of therapy (Fig 1), and the variety of unique responses in terms of therapeutic choices. For example, with scenario 1 (the mildest subclinical scenario presented), respondents formulated seven distinct therapeutic combinations; by scenario 12, respondents formulated 48 distinct therapeutic combinations (Fig 2a). Additionally, as the severity of the disease scenario presented increased, the number of clinicians stating that they would administer three or more medications increased (Fig 2b). In scenarios with CHF, >88% of clinicians stated that they would prescribe three or more medications.

(a) Intent to alter primary disease progression or to treat congestive heart failure (CHF). Collated responses were restricted to drugs or interventions that are not obviously antithrombotic or anticoagulant. (b) Intent to reduce risk of occurrence of aortic thromboembolism (ATE). Collated responses were restricted to clopidogrel, aspirin, low molecular weight heparin (LMWH) and heparin. In (a) and (b) cardiologist respondents are represented by the pink bars, non-cardiologist respondents by the black bars. (c) Use of clopidogrel or LMWH

(a) Number of different treatment combinations adopted by respondents for each scenario. (b) Percentage of respondents prescribing three or more medications to patients with each scenario. CHF = congestive heart failure
Fig 1 shows therapeutic choices based on intervention that we interpreted as being aimed at preventing disease progression (scenarios 1–7; Fig 1a), treating CHF (scenarios 8–12; Fig 1a) or reducing the risk of ATE (all scenarios; Fig 1b). Over 82% (75/91) of respondents showed intent to reduce the risk of ATE by scenario 7, and this approached 98% (86/88) by scenario 12. Fig 1c shows the percentage of respondents selecting LMWH or clopidogrel in each scenario. Clopidogrel therapy was instituted in earlier scenarios, and cardiologists appeared to be more likely than non-cardiologists to prescribe clopidogrel. LMWH use was instituted with severe disease, and selection of LMWH increased with disease severity.
Fig 3 shows use of β-blockers. These drugs were chosen more commonly in subclinical disease when dynamic LVOT obstruction was present (scenarios 3, 4, 6 and 7) (P < 0.0001), and use increased with more severe obstruction — ie, increased use in scenarios 4 (4.8 m/s), 6 (3.8 m/s) and 7 (4.5 m/s) compared with scenario 3 (2.2 m/s) (P < 0.0001). Similarly, with onset of CHF, β-blocker use was chosen more commonly when dynamic LVOT obstruction was present (scenario 9 versus scenario 10) (P < 0.0001). However, fewer clinicians opted to use β-blockers once CHF was present, regardless of the presence or absence of dynamic LVOT obstruction (P < 0.0001).

Cardiologist respondents are represented by the pink bars, non-cardiologist respondents by the black bars. Numbers above bars represent the left ventricular outflow tract (LVOT) velocity (expressed in m/s) associated with LVOT obstruction presented in that particular scenario. CHF = congestive heart failure
Fig 4 shows use of diltiazem and ACEIs. Despite preliminary published evidence of efficacy of diltiazem in treating HCM with CHF, 25 only a maximum of 30% of respondents prescribed diltiazem in any scenario (the highest usage was with CHF; Fig 4b). Use appeared to decrease in scenarios with LVOT obstruction. By contrast, ACEI use (Fig 4a) increased steadily with disease complexity, with virtually 100% of respondents using it with CHF.

(a) Angiotensin-converting enzyme inhibitor (ACEI) use increases with increasing severity of hypertrophic cardiomyopathy (HCM). (b) Diltiazem use is substantially lower than ACEI use and is inversely correlated with β-blocker use. Cardiologist respondents are represented by the pink bars, non-cardiologist respondents by the black bars
Table 3 summarizes treatment choices for each scenario.
Distribution of responses for each scenario in the HCM survey

Scenarios 1–7 described subclinical hypertrophic cardiomyopathy (HCM) patients, scenarios 8–12 described HCM patients with congestive heart failure. See Table 1 for full scenario descriptions. Scenarios 3, 4, 6, 7, 9 and 10 had evidence of dynamic left ventricular outflow tract obstruction. ATE = aortic thromboembolism, NA = not assessed
Justification for therapeutic choices was asked for scenarios 1 and 7 for group A, and scenarios 4 and 12 for group B. Overall, treatment choices by respondents, when asked to justify their decisions, did not differ from the responses by those not asked to justify their decision for any of the scenarios.
For any scenario, the most commonly chosen reasons for not administering a particular therapy were either lack of evidence showing benefit, or that the treatment was not a logical choice in that particular scenario. Reasons chosen to support administering a particular therapy were more varied, but most commonly included research showing theoretical (unproven) benefit in cats or other species, favorable personal experience with a particular therapy, consensus among peers favoring use, or the opinion that the therapy ‘probably doesn't hurt and might help’.
The literature search yielded 540 relevant citations. Of these, 126 addressed issues associated with HCM and 37/126 dealt with therapy of HCM or ATE (20 clinical studies and 17 review articles addressing therapeutic aspects). Of the 20 clinical studies, we identified two randomized clinical trials 23,25 and three prospective case series that addressed patient-oriented outcomes. 22,56,57 We identified three randomized clinical trials addressing disease-oriented outcomes, 19,21,58 eight experimental studies examining aspects of coagulation, 59–66 and four retrospective studies (case-control or case series). 18,22,24,27 We found no published studies addressing use of β-blockers in subclinical HCM. We found no clinical studies examining patient-oriented outcomes (ie, delay of disease progression) in subclinical HCM.
Discussion
Our study highlights the variability of therapeutic approaches to feline HCM of varying severity reported by cardiologists and non-cardiologists. With most of the scenarios presented in this study, there appeared to be marked variability and lack of consensus about most specific therapies. There was general consensus on a few points: all clinicians reported using furosemide with evidence of CHF, most clinicians reported using ACEIs with evidence of CHF, and most clinicians reported using β-blockers with substantial dynamic LVOT obstruction.
With subclinical HCM, treatment choices varied, ranging from mostly no therapy with mild forms of disease, to aggressive therapy with more severe subclinical forms. We assumed in this study that such treatments were aimed at either altering disease progression or preventing ATE, when prescribed to cats with subclinical HCM. Applying this assumption, as the subclinical severity increased, some clinicians displayed a tendency to attempt to delay the onset of CHF by prescribing ACEIs or even diuretics. Similarly, in scenarios where spontaneous left atrial echocardiographic contrast ('smoke’) was present, clinicians displayed an increased tendency to institute antithrombotic therapies, presumably to prevent ATE. We assumed that treatment choices in scenarios describing earlier/milder disease were aimed at altering myocardial remodeling rather than preventing the onset of CHF. Even with the mildest disease, a small proportion of clinicians reported that they would administer some form of therapy.
Treatment decisions made by veterinary cardiologists did not appear to differ dramatically from those made by veterinarians with an interest in cardiology. Our findings show a marked disconnect between published clinical data for therapy of cats with HCM and treatment choices made by cardiologists and non-cardiologists when treating both clinical and subclinical HCM.
Despite the willingness of cardiologists to adopt treatment strategies for their feline HCM patients, we could find virtually no clinically relevant literature to support these decisions. This issue was recognized by the survey participants when asked to justify their choices — they rarely selected the justification option that a particular therapy had been demonstrated by controlled clinical trials to have a clinical benefit in the scenario in which they were prescribing the medication. Previous authors have made similar observations about the paucity of therapeutic evidence. 29,67 In most cases, clinicians prescribed medications because of theoretical benefits, extrapolations from human HCM therapy, peer consensus, or because it ‘probably doesn't hurt and might help’ (however, as was pointed out to one of the authors by a colleague, this is merely the optimist's version of ‘probably doesn't help and might hurt’!).
The reasons for this disconnect between sufficient clinical evidence for instituting therapy and self-reported treatment strategies are likely multifactorial. These include personal favorable experience (as with β-blocker use for dynamic LVOT obstruction); the desire by clinicians to ‘do something’; pressure from clients or referring veterinarians to provide a service beyond diagnosis (to offset the feeling of futility or frustration in the client or clinician); and belief that their intervention is, at worst, doing nothing and, at best, altering disease outcome.
In other cases, the treatment alters a measurable physiological variable, such as LVOT obstruction. Clinicians likely used this as a surrogate marker of clinical outcomes, despite a lack of evidence demonstrating such relationships. Additionally, clinicians commonly justified their use of certain drugs by extrapolating from data in other species. This was most apparent for β-blocker therapy of LVOT obstruction (where treatment of humans provides symptomatic relief and improves exercise tolerance) and use of anticoagulants (LMWH and clopidogrel). However, the problems with such approaches (personal experience, interspecies extrapolation) are highlighted by one investigator, who, in a review of β-blockade in HCM in 1991, suggested that clinical experience and extrapolation from other species would support the use of β-blockers in cats with CHF secondary to HCM. 26 This same investigator subsequently failed to demonstrate this benefit in a clinical study, and showed potential harm of such therapy. 31
Of note is the reported common practice of prescribing medications for treating subclinical HCM. We assumed this practice was based on the hypothesis that early intervention would result in slowed disease progression. Almost 50% of clinicians adopted this strategy with mild disease, and almost all adopted this strategy with severe subclinical disease, despite the lack of evidence demonstrating any benefit of therapy in subclinical HCM in cats. Our findings also demonstrated that as the complexity of the disease increased, the tendency to prescribe three or more drugs increased, with 88% of clinicians prescribing three or more drugs at the onset of CHF. This observation raises several points for consideration (see box below):
Recently, investigators examined factors that impacted quality of life decisions for owners of cats with heart failure and found that owner stress of administering medications increased with the number and frequency of medications. 72 Thus, clinicians should consider the potential negative implications of their treatment strategies when committing a client and patient to potentially prolonged therapy that often requires more-than-once-daily administration of multiple medications.
We were surprised by the infrequent use of diltiazem in feline HCM. When asked to justify their choice for not using diltiazem in the four scenarios requesting justification, approximately 50% of respondents stated that they did not use it because there was ‘no evidence showing benefit with regard to survival or progression in cats’. Thus, it appears that a preliminary study suggesting benefit in cats with HCM and CHF has not translated, for most clinicians, into experience of clinical benefit. 25 There appeared to be an inverse relationship between β-blocker use and diltiazem use for individual scenarios. In the cases with dynamic LVOT obstruction, diltiazem use decreased, presumably because of the concerns of using β-blockers and diltiazem together.
Treatment of subclinical HCM: considerations
Given the unpredictable nature of HCM in most cats, with no clear means of distinguishing early progressive disease from mild, non-progressive disease, it is highly likely that many feline patients are subjected to unnecessary medical therapy, because the disease in these patients would never progress, regardless of intervention.
Given the lack of evidence for benefit, medicating may subject many patients and clients to years of unnecessary inconvenience and stress.
Given that clients might not observe a benefit (as the cat has subclinical disease) and/or experience difficulty medicating their cat, especially when administering three or more medications, non-compliance rate might be substantially higher than specialist clinicians suspect. This can lead to an over-estimation of benefits of therapy. Additionally, clients not willing to admit to non-compliance might elect not to present their patients for follow-up visits or elect to follow-up with other clinicians to avoid embarrassment or conflict with the prescribing veterinarian. This could result in suboptimal management of cases or a presumption by the clinician that ‘all is well’ with the patient and that their therapy was of benefit.
Given that no data exist about clinically relevant outcomes of the therapies commonly employed with subclinical HCM (as reported in this study), there is an unfounded assumption that therapy is either helping, or doing no harm. It is, however, quite possible, as previous landmark studies in human medicine have demonstrated, that perceived and commonly acknowledged ‘benefits’ of therapies can indeed be harmful, when critically evaluated. 68–71
Limitations
This study has a number of limitations. Several clinicians alluded to the fact that they tailor therapy to the specific individual. However, we were interested in ‘average’ treatment choices in each scenario — what a clinician was likely to do given a set of observations in a cat with HCM.
Additionally, we presented somewhat loose definitions of severity based on left atrial size and wall thickness, which we labelled as ‘mild’, ‘moderate’ and ‘severe’. Respondents could interpret these classifications differently, or use the various criteria differently (eg, left atrial enlargement versus wall thickness) to determine treatment choices. How this would affect the survey results is unclear.
We did not specifically ask for the clinicians' intent as to their therapeutic choices, but made assumptions about intent based on the known pharmacology of the drugs chosen and standard therapeutic strategies adopted with these drugs. Therefore, it is possible that, in some cases, our assumptions were incorrect and that respondents were prescribing medications for reasons other than those which we ascribed.
Our literature search was possibly not exhaustive. However, we believe that we identified all the literature pertinent to treatment of feline HCM that had been published during the specified period. Subsequent to the original search, a few additional studies have been published detailing aspects of treatment and pathophysiology of HCM, but we do not believe that they have impacted the therapeutic decisions of cardiologists (as evidenced in a recent unpublished survey of veterinary cardiologists). 20,73,74
Footnotes
Acknowledgements
We would like to thank Cornell reference librarian Susanne Whitaker for help with the literature search. The data in this article were first presented as an abstract at the ECVIM-CA Congress, Amsterdam, September 14–16, 2006.