
Abstract
An 11-month-old, 3 kg, female domestic shorthair cat was referred to evaluate cardiac structure and function. Echocardiography revealed the membrane dividing the left atrium into two chambers, a large defect in the lower part of the atrial septum, and turbulent blood flow from the distal left atrium into the right atrium. These findings suggested cor triatriatum sinister (CTS) with incomplete atrioventricular septal defect (AVSD). The cat was treated with medications for management of congestive heart failure. In the end, she died from right-sided heart failure 17 months after the initial presentation. At necropsy, a fibromuscular membrane with a round orifice in the left atrium and an ostium primum defect were confirmed, and the definitive diagnosis of CTS with incomplete AVSD was made. To our knowledge, this study presents the first case report of CTS with incomplete AVSD in a cat.
An 11-month-old, 3 kg, female domestic shorthair cat was referred to the Veterinary Teaching Hospital, Tokyo University of Agriculture and Technology for evaluation of cardiac structure and function. Although the cat was in good general condition, she was undersized in comparison with her healthy littermates. On physical examination, the cat was quiet, alert, and responsive. The apex beat was palpable in the right fifth intercostal space, and was strong and forcible. Auscultation revealed a regular rhythm and rate of 200 beats per min (bpm), and a grade 4/6 holosystolic murmur with a thrill over the left caudal parasternal area. The results of a complete blood count including white blood cell count 10.9×103/μl (reference interval (RI) 5.5–19×103/μl), red blood cell count 9.5×106/μl (RI 5–10×106/μl), haemoglobin 12.3 g/dl, haematocrit 37.5% (RI 36–60%) and platelet count 17×104/μl (RI×104/μl), and those of serum biochemical analysis including blood glucose 90 mg/dl (RI 56–153 mg/dl), blood urea nitrogen 27.7 mg/dl (RI 10–30 mg/dl), creatinine 1.0 mg/dl (RI 0.9–1.8 mg/dl), aspartate aminotransferase 28 U/l (AST; RI 1–37 U/l), alanine aminotransferase 48 U/l (ALT; RI 1–54 U/l), alkaline phosphatase 193 U/l (RI 6–102 U/l), total bilirubin 0.1 mg/dl (RI 0–0.2 mg/dl), total cholesterol 71 mg/dl (RI 63–171 mg/dl), total protein 6.2 g/dl (RI 5.4–7.3 g/dl), sodium 152 mEq/l (RI 137–162 mEq/l), potassium 3.8 mEq/l (RI 3.6–5.6 mEq/l), and chloride 119 mEq/l (RI 115–130 mEq/l) were within normal limits.
Thoracic radiography revealed severe enlargement of the cardiac silhouette and dilation of the pulmonary vessels. The rounded cardiac apex was shifted to the right of midline in dorsoventral view (Fig 1). Pulmonary oedema was not detected. Electrocardiography (Alpha8000, Fukuda ME, Japan) showed small R waves and deep S waves on standard limb lead II (Fig 2). On echocardiography (ProSound Alpha10, Aloka, Japan), a perforate membrane dividing the left atrium into a proximal and a distal chamber was visualised by using the right parasternal long-axis view (Fig 3), in addition to moderate irregular thickening of the mitral valve (MV) and marked dilation of all four chambers with wall thinning. Colour-flow Doppler showed turbulent continuous blood flow over the dividing membrane (Fig 4). The velocity of the turbulent blood flow was 5.2 m/s measured during systole by continuous wave Doppler in the left apical four-chamber view demonstrating mitral regurgitation. Turbulent diastolic flow spread from the distal left atrium (DLA) into the right atrium (RA) through a large defect in the lower part of the atrial septum. Its peak velocity measured during diastole was 2.2 m/s in the right parasternal long-axis view. These findings suggested a left-to-right shunt at the atrial level. Based on the typical findings of echocardiography, a presumptive diagnosis of cor triatriatum sinister (CTS) with incomplete atrioventricular septal defect (AVSD) was made.

Dorsoventral (A) and left lateral (B) thoracic radiographs of the cat show extreme cardiac enlargement and dilation of the pulmonary vasculature. The cardiac apex is shifted to the right of midline (arrowheads).

Small R waves (0.2 mV) and deep S waves (1.8 mV) are observed in the ECG tracing (lead II) recorded from the cat. These features are consistent with right ventricular hypertrophy (paper speed=50 mm/s; 10 mm=1 mV).

Two-dimensional echocardiography (right parasternal long-axis four-chamber view) of the cat at the initial presentation shows the membranous structure (white arrowheads) dividing the left atrium into two chambers and the defect in the lower part of the atrial septum (asterisk). PLA=proximal left atrium.
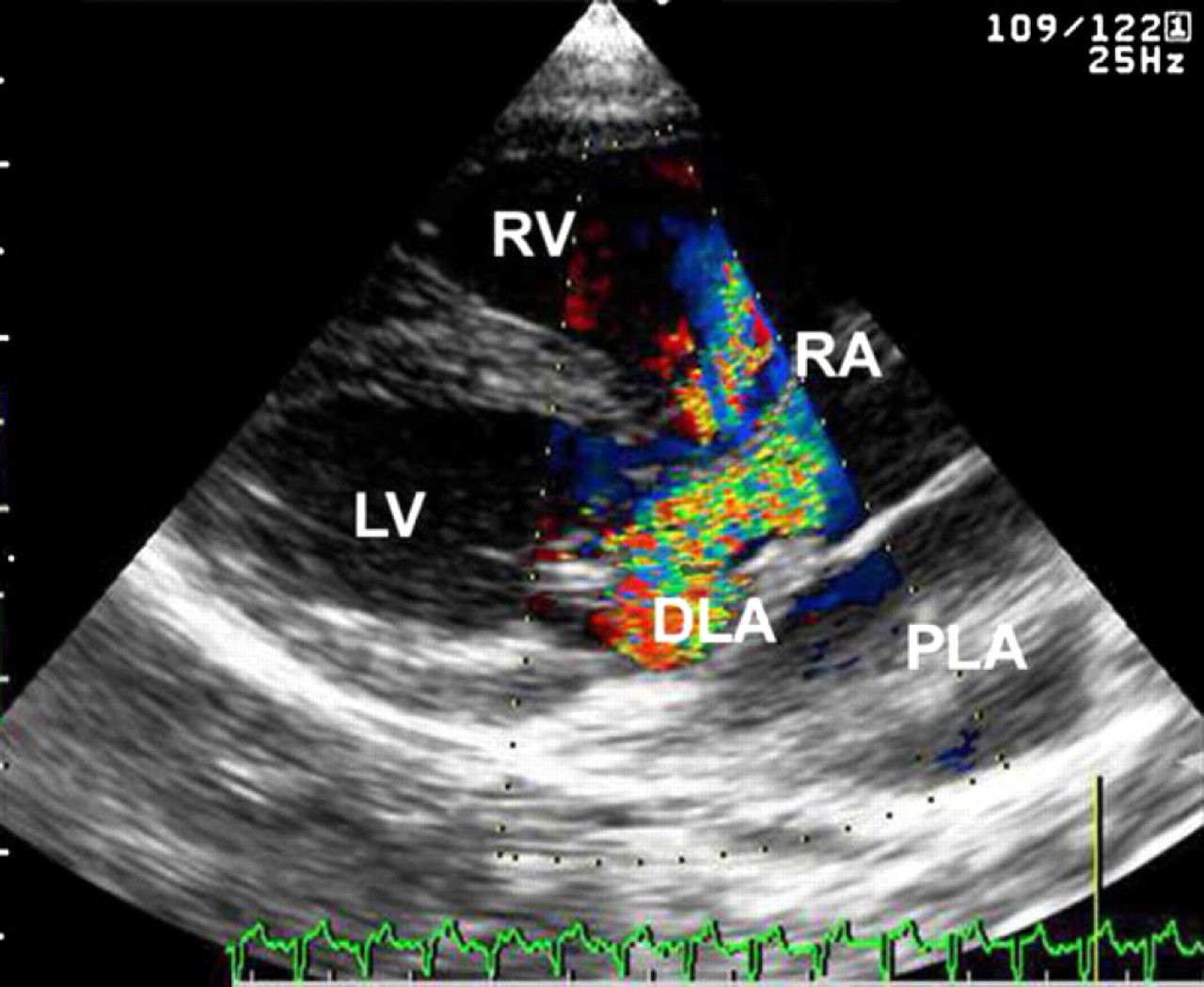
Colour-flow Doppler echocardiography (right parasternal long-axis four-chamber view) of the cat at the initial presentation shows turbulent systolic flow in the DLA and the RA. PLA=proximal left atrium.
The cat was treated with furosemide (Lasix; Sanofi-Aventis KK) 0.5 mg/kg, PO, q 12 h, digoxin (Digosin; Chugai Pharmaceuticals) 0.005 mg/kg, PO, q 12 h and metoprolol succinate (Lopresor; Novartis Pharma KK) 1.5 mg/kg, PO, q 12 h for the medical management of congestive heart failure, and with beraprost sodium (Dorner; Toray) 2.0 μg/kg, PO, q 12 h for the control of pulmonary hypertension. Spironolactone (Aldactone-A; Pfizer Japan) 1.0 mg/kg, PO, q 12 h was used because of its potential anti-remodeling effect on the left ventricle (LV). Surgical resection of the dividing membrane was not adopted because of marked volume overload and moderate pulmonary hypertension. As follow-up assessments, echocardiography, thoracic radiography, electrocardiography, and blood examination were performed every 4 weeks.
Twelve months after the initial presentation, echocardiography suggested development of eccentric cardiac hypertrophy due to the detection of more dilated chambers of the atria and the right ventricle (RV). The left auricle extended by approximately half of the LV toward the left ventricular apex. At 17 months after diagnosis, the cat developed dyspnoea, depression, anorexia, and dehydration. Echocardiography revealed marked left atrial enlargement, decreased ventricular wall motion, and a moderate to large amount of pleural, pericardial and abdominal effusion. The left auricle appeared to extend to the left ventricular apex. Thoracocentesis was performed for the improvement of dyspnoea, and 120 ml of haemorrhagic pleural effusion was removed. Additionally, the cat was medicated with an increased dose of furosemide 1.0 mg/kg, PO, q 12 h, and was given subcutaneous fluid therapy (Ringer's acetate: Solacet F; Terumo, Tokyo, Japan) 100 ml/head, SC. Although the general condition of the cat initially improved, the dyspnoea returned 3 days after the thoracocentesis. The same treatments were repeated every 3 days due to the owner's rejection to the option of euthanasia. The cat died of recurrent pleural effusion 2 weeks after the first thoracocentesis.
Post-mortem examination was limited to the heart and lungs at the owner's request. On gross examination, there was marked dilation of all cardiac chambers, which had extremely thin walls. Particularly, both atria were greatly enlarged and the thickness of their walls was paper-thin. A prominent finding was that the left atrium was divided into proximal and distal chambers by a membrane. The proximal chamber received four pulmonary veins, and the distal chamber was connected to the LV through the MV. A fibrous round orifice of 5 mm in diameter was located in the centre of the membrane (Fig 5A). Moreover, an ostium primum defect was detected between the DLA and the RA (Fig 5B and C). Based on these typical findings, a definitive diagnosis of CTS with incomplete AVSD was made. In addition, the MV leaflets were thickened and shortened with moderate dilation of the valve annulus. Although the tricuspid valve (TV) was involved to a lesser degree, marked dilation of its annulus was found. The lungs were light pink, wet, heavy and distended, and foamy fluid oozed from a cut surface. The thoracic cavity contained excess haemorrhagic fluid. On histopathological examination, the dividing membrane consisted of fibromuscular tissue. The mitral and TVs showed mild to moderate myxomatous degeneration. Focal sclerosis and interstitial fibrosis were observed in the upper part of the ventricular septum. Pulmonary oedema with varying degrees of chronic interstitial pneumonia was found throughout the lungs.

The heart of the cat at necropsy. (A) The opened left atrium shows the dividing membrane with a fibrous round orifice (arrowhead). (B) The thickened and distorted leaflets of the mitral and TVs are seen from the RA through the ostium primum defect (asterisk) (the dividing membrane removed). (C) Cross-section of the heart shows severe eccentric hypertrophy and the ostium primum defect (asterisk). PLA=proximal left atrium. Scale=1 mm.
CTS is an uncommon congenital heart disease that results from a fibromuscular membrane, dividing the left atrium into a proximal chamber and a distal chamber. 1,2 CTS occurs during the development of the pulmonary venous system, and results in the common pulmonary venous chamber being incorporated incompletely into the left atrium. 1,3,4 Incomplete AVSD is also a rare congenital abnormality, which includes an atrial septal defect in the lower part of the atrial septum. Incomplete AVSD occurs as a result of abnormal development of the endocardial cushions. 1,5
The diagnosis of CTS with incomplete AVSD was based mainly on echocardiography in the cat, and the dividing membrane in the left atrium and the large defect in the lower part of the atrial septum were detected. These findings corresponded well to the morphological features on post-mortem examination. Echocardiography is an easy, non-invasive, and valuable tool for diagnosis of cardiac malformations, such as the present case.
A few reports of CTS in cats have been published. 1,6–8 There has been only one previous report of successful surgical treatment of CTS in a kitten. 7 Incomplete AVSD is also an uncommon anomaly in cats. 5,9,11 Cats with this congenital defect generally develop severe heart failure and die at a very young age. 1 Thus, no appropriate treatment of both CTS and incomplete AVSD has yet been established. On the other hand, in humans, surgical resection of the abnormal membrane is the only treatment choice in patients with CTS in order to resolve the associated signs. However, CTS with other concurrent congenital heart conditions may be associated with a higher degree of surgical risk. 3,4,10 According to these reports, our decision not to adopt surgical resection of the dividing membrane may have kept the cat in a good general condition until the last 2 weeks. Therefore, it is uncertain whether surgery would be most effective for the treatment of malformations similar to the present case.
Some human cases of CTS are associated with a complex of congenital heart conditions. 3,11 However, to our knowledge, there has been no previous report of a cat with a complex of CTS and any other cardiac malformations. Therefore, this is the first reported feline case of CTS with incomplete AVSD.