
Abstract
A 7-year-old, entire female, domestic shorthair cat presented with recurrent upper respiratory tract problems. Infectious otitis media caused expansion of the middle ear which ultimately resulted in complete obstruction of the nasopharynx. A ventral bulla osteotomy was successful in relieving the clinical signs.
A 7-year-old, entire female, domestic shorthair cat was referred to North Downs Specialist Referrals with an 18-month history of gradually worsening upper respiratory tract noise. Over the 2 months prior to referral the cat had started to sneeze. There had been some clear, mucoid discharge from both nostrils, which improved on antimicrobial therapy given by the referring veterinary surgeon. The owner also reported the cat to occasionally shake her head and scratch her ears.
On physical examination the cat was bright and alert and in good body condition. A grade II/VI systolic cardiac murmur with point of maximum intensity over the caudal sternum was detected as an intermittent gallop rhythm. Femoral pulse quality and capillary refill time were within normal limits. Survey thoracic radiographs submitted by the referring veterinary surgeon showed the cardiac shape and pulmonary vasculature to be within the normal limits. There was increased respiratory noise from the nasal/nasopharyngeal area without any evidence of nasal or palatal deformity or nasal discharge. There was detectable airflow through both nostrils. No further abnormalities were noted.
Initial blood work including a full biochemical profile, electrolytes, complete blood cell count and feline leukaemia virus/feline immunodeficiency virus serology (Speed FeLV and FIV; Virbac) were within normal limits. Urinalysis was within normal limits.
The cat was anaesthetised and a computed tomography (CT) scan (GE HighSpeed Dual, GE Healthcare, No 2 North Yong Chang Street, Beijing 100176, PR China) of the skull was performed (see Fig 1a). There was expansion of the left tympanic bulla with bony proliferation ventrally, measuring up to 6 mm in size. The remainder of the bulla was irregular in outline. The majority of the septum dividing the bulla into two compartments was eroded. The tympanic cavity was filled with soft tissue attenuating material. The expansile bulla caused compression of the nasopharynx, narrowing it down to 1 mm (Fig 1a). The right tympanic bulla showed a small amount of soft tissue attenuating material, which was interspersed with gas bubbles. The nose and frontal sinuses appeared within the normal limits. These findings were compatible with bilateral otitis media with secondary bony changes and expansion of the left tympanic bulla. Neoplasia was considered as a differential diagnosis, but was thought to be less likely because the lesion was not destructive enough, the soft tissue attenuating material was confined to the tympanic bulla and solid appearing new bone formation was present. A congenital malformation of the tympanic bulla with a secondary infectious process was also considered, but thought to be unlikely in view of the age of the cat when the clinical signs were first noted, the changes in both bullae and to the authors knowledge unilateral congenital enlargement of the tympanic bulla has not been reported in the literature. Cholesteatoma has been reported in dogs and can present with a similar CT-images. 1 The subsequent histopathology findings were not consistent with a cholesteatoma.
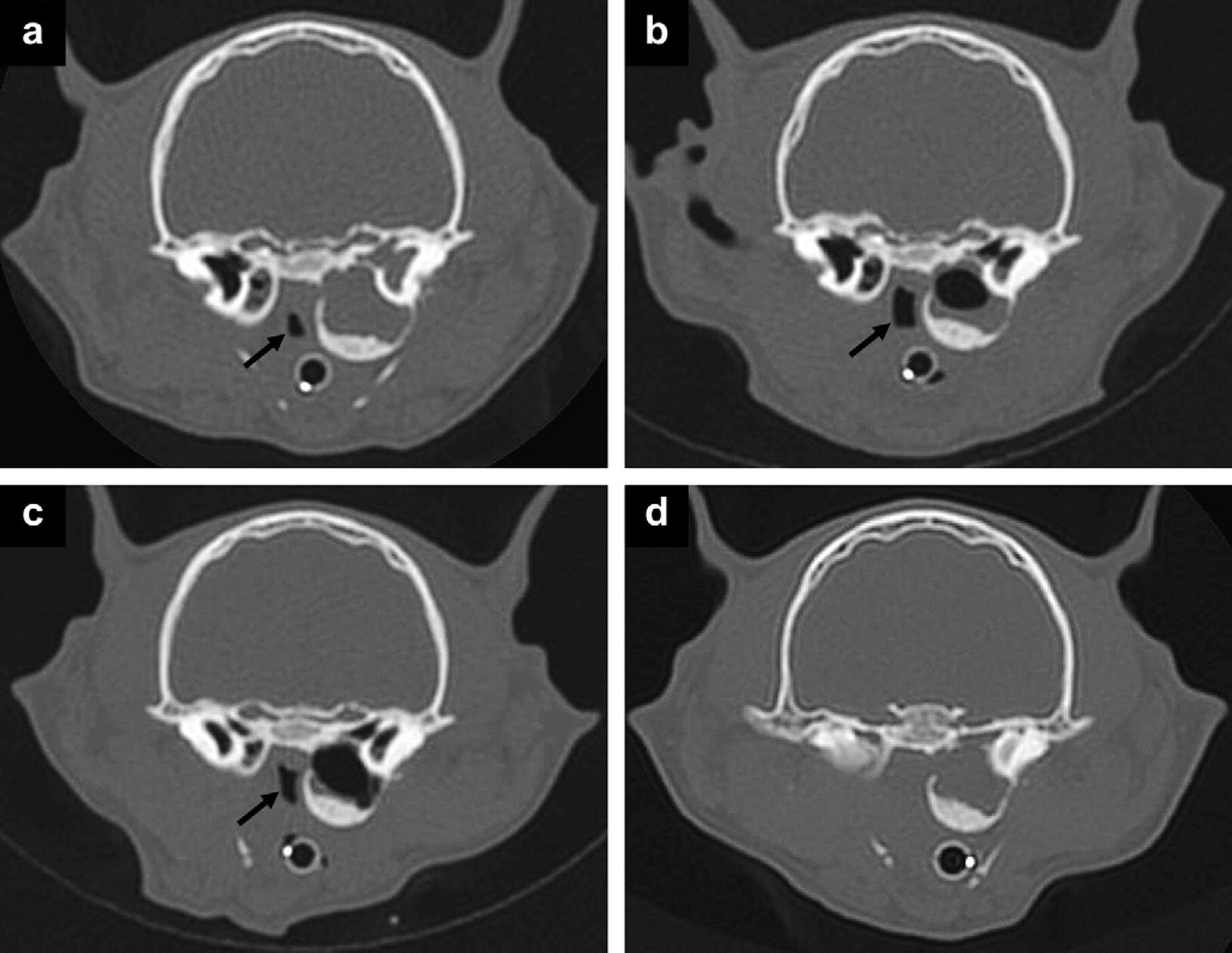
Subsequent CT-images of the head at a similar level (WW4000, WL450). (a) The first study shows expansion of the left tympanic bulla with compression of the nasopharynx (black arrow). The tympanic cavity is filled with soft tissue attenuating material. (b) A repeat CT-scan 1 month later shows decrease in soft tissue attenuating material within the left tympanic cavity. There is compression of the nasopharynx (black arrow); however, the lumen is increased in size compared to the previous study. The right tympanic bulla appears similar compared to the previous study. (c) A repeat CT-scan 2 months after initial presentation shows a further reduction in soft tissue attenuating material within the left tympanic cavity. The nasopharynx is slightly smaller than in (b) (black arrow). (d) Fourteen months after the initial presentation, the left tympanic bulla appears similar in size and shape to all previous studies. However, it is completely filled with soft tissue attenuating material. There is complete occlusion of the nasopharynx.
Otoscopic examination of both external ear canals showed increased opacity of the left tympanic membrane. Aspiration of the left middle ear via myringotomy revealed purulent, blood tinged material and cytology revealed marked neutrophilic inflammation with intra- and extra cellular rods. Bacterial culture revealed a mixed growth of organisms. A bacterial sensitivity was requested at the same time, but the laboratory reported a preponderance of several bacterial organisms and could not do sensitivity testing. On rhinoscopy, performed both per oral retroflexed (3.7 mm diameter flexible endoscope, ETM Germany) and rostral (1.9 mm diameter rigid endoscope, Karl Storz) there were no macroscopic changes of the nasal mucosa. A nasal flush was submitted for cytology and bacterial culture and nasal mucosal biopsies were taken for histopathology. These revealed very mild neutrophilic inflammation with some superficial hyphae, too narrow to be considered consistent with Aspergillus species, with a fruiting body with scattered spores. The fungal body was not associated with inflammation and thought to be an incidental finding. Bacterial (aerobic and anaerobic) and fungal cultures of the nasal flush were negative.
On the basis of these tests a diagnosis of mild neutrophilic rhinitis and infectious middle ear disease, causing secondary, chronic changes to the tympanic bulla was made. The different treatment options including antimicrobial therapy and/or ventral bulla osteotomy were discussed with the owner.
The cat was started on Enrofloxacin (Baytril; Bayer, 5 mg/kg q 24 h). On re-examination 1 month later, the owners reported resolution of the clinical signs. A repeat CT-scan (Fig 1b) showed the left tympanic bulla to be of similar size and shape and with similar wall thickness. There was evidence of a decrease in soft tissue attenuating material within the left tympanic bulla. The soft tissue was mainly located peripherally, while air attenuation was visible in the centre. The left bulla caused compression of the left lateral wall of the nasopharynx. The lumen of the nasopharynx was increased in size compared to the previous study, measuring 3 mm in width (Fig 1b). The right tympanic bulla and cavity appeared similar to the previous study. It was decided to continue antimicrobial therapy. One month later the clinical signs had not recurred and a repeat CT-scan (Fig 1c) showed no further changes in new bone formation or erosion of the left tympanic bulla but a further reduction of soft tissue attenuating material. The bulla was still compressing the nasopharynx. The expansion of the middle ear and thickening of the bony case were considered to be chronic change that was not likely to reverse. It was decided to monitor the cat and if the clinical signs recurred to consider ventral bulla osteotomy.
Ten months after the initial referral appointment the cat developed nasal discharge from the left nostril, which responded to antimicrobial therapy and 12 months after the initial referral appointment an increased upper respiratory tract noise became apparent, mainly emanating from the nasopharyngeal area. This clinical sign did not respond to antimicrobial therapy and the cat was re-referred 14 months after the initial referral appointment.
On physical examination the cat was subdued, but in good body condition. There was an increase in upper respiratory tract noise, coming from the nasopharyngeal area with marked reduction in airflow through both nostrils. The rest of the physical examination was similar to the previous examinations.
A repeat CT-scan of the skull (Fig 1d) revealed that the left tympanic bulla appeared similar to the first study, being filled with soft tissue attenuating material, which showed moderate peripheral contrast enhancement compatible with mucosal hyperplasia/granulation tissue in the periphery and fluid in the centre. The nasopharynx was occluded over a length of 6 mm (Fig 1d) by compression from the tympanic bulla. The right bulla was filled with soft tissue attenuating material, which showed moderate heterogeneous contrast enhancement.
Per oral retroflexed endoscopy (3.7 mm flexible endoscope, ETM Germany) revealed the nasopharyngeal mucosa bulging into the nasopharyngeal lumen, completely obliterating the nasopharyngeal lumen. The nasopharyngeal mucosa appeared macroscopically normal.
A unilateral left ventral bulla osteotomy was performed. The osteotomy was extended as far medially as possible to alleviate the obstruction. The left bulla was filled with thick, foul smelling, purulent material and also some soft tissue. The material was submitted for bacterial (both aerobic and anaerobic) and fungal culture and histopathology (including a periodic acid–Schiff (PAS) stain). The bulla was copiously lavaged with sterile saline.
Histopathology of the tissue from the middle ear was consistent with chronic otitis media with inflammatory polypoid changes. The culture revealed mixed bacterial growth and again the laboratory reported that it could not do sensitivity testing due to a preponderance of different organisms. A PAS stain was negative. A 14-day course of a cephalosporin was prescribed.
On repeat examination 1 month after the surgery, the cat did not show any clinical signs. Six months after surgery the owners report the cat to be in good health without any clinical signs.
Otitis media can result in signs of middle ear disease such as otic pain and lethargy and occasionally neurological signs particularly Horner's syndrome. 2 This cat did not show any overt clinical signs related to middle ear disease.
With the increase in advanced imaging modalities, such as CT it has become apparent that there are middle ear changes in a number of cats that present with upper respiratory tract disease (28%). 3 CT-changes in otitis media usually consist of an increase in soft tissue/fluid opacity within the middle ear and occasionally thickening of the tympanic bulla. These cats may not show clinical signs of middle ear disease. 4
In some cases, otitis media can result in the development of inflammatory polyps. These can extend into the pharynx through the Eustachian tube and cause increased upper respiratory tract noise and occasionally obstruction. It is assumed that in the case described here, nasopharyngeal obstruction was caused by compression of the tympanic bulla on the nasopharynx. Additionally, as the size of the tympanic bulla did not change, it is hypothesised that additional nasopharyngeal mucosal inflammation caused further swelling, which contributed to the complete occlusion of the nasopharynx. This is supported by the fact that the size of the nasopharyngeal lumen initially increased on antimicrobial therapy. The fact that the signs related to nasopharyngeal obstruction were relieved by a bulla osteotomy suggests that obstruction by the expansile bulla still played a large role.
This is the first reported case, to the authors’ knowledge, where otitis media caused expansion of the middle ear and to such an extent that it resulted in complete obstruction of the nasopharynx.