
Abstract
Clinical report
History
A 3-year-old spayed female British shorthair cat was presented to the Royal Veterinary College's Queen Mother Hospital for Animals for further assessment and management of a suspected oesophageal foreign body. The cat had been missing for 3 days. On her return, she retched and regurgitated on several occasions and displayed an inability to swallow food despite a good appetite. These signs prompted a visit to the referring veterinarian who performed cervical and thoracic radiography, which demonstrated the presence of a bony foreign body in the oesophagus at the level of the thoracic inlet.
Referral examination and initial investigations
On presentation to our institution, the cat was bright, alert and responsive. With the exception of mild dehydration, her vital parameters and major body systems assessment were within normal limits. The cat displayed discomfort on palpation of the base of her neck and was salivating excessively. Signs consistent with Horner's syndrome (ie, miosis, enophthalmos, palpebral ptosis and protrusion of the third eyelid) were present in the right eye. All of these clinical signs were consistent with the presence of an obstructive foreign body lodged in the caudal cervical/cranial thoracic oesophagus, with an associated lesion or compression of the cervical sympathetic chain (or, less likely, another cervical trauma or disease).
No abnormalities were detected on haematology and serum biochemistry. Topical administration of 10% phenylephrine in the right eye allowed classification of the Horner's syndrome as being of third order, confirming a postganglionic lesion. After initial fluid resuscitation, the cat underwent general anaesthesia. Following premedication with pethidine (5 mg/kg IM) (Pethidine injection BP; Martindale), anaesthesia was induced using an incremental dose of alfaxalone (Alfaxan; Vétoquinol), to effect. The cat was intubated and anaesthesia was maintained with a gaseous mixture of isoflurane and oxygen administered via a Jackson-Rees modification of an Ayre's T-piece breathing circuit.
Orthogonal thoracic radiographs, encompassing most of the cervical area, confirmed the presence of a 4 cm length of bone in the cat's cranial thoracic oesophagus — most likely the scapula of a chicken or rabbit (Fig 1). No other abnormality was present on this set of films. Endoscopic assessment revealed that the bony foreign body was occluding most of the oesophageal lumen, and was associated with marked ulceration of the oesophageal mucosa. No obvious area of perforation was identified.
Endoscopic retrieval of the foreign body was attempted, but quickly proved impossible due to the friability of the foreign body and the development of relatively marked intraluminal oesophageal haemorrhage as soon as traction was applied to the bone. The endoscopic procedure was thus aborted with a view to performing surgical retrieval of the bone but, almost immediately, a sudden deterioration in the ventilation and oxygenation anaesthetic parameters prompted further radiography of the cat's chest. This revealed a marked pneumomediastinum, pneumothorax and subcutaneous emphysema, all consistent with a rupture of the oesophagus at the level of the thoracic inlet (Fig 2).
The cat was ventilated and transferred to theatre without delay. The air accumulating in the pleural space was drained on two occasions via thoracocentesis as the cat was prepared for surgery. A constant rate infusion of fentanyl (3 μg/kg IV) (Sublimaze; Janssen-Cilag) was initiated and potentiated amoxicillin (20 mg/kg IV) (Augmentin; GlaxoSmithKline) was administered for prophylactic antibiosis.
Surgery
The cat was positioned in dorsal recumbency. After surgical preparation of the ventral part of the neck, chest and abdomen, a ventral midline cervical approach was made, in combination with a cranial sternotomy (to the level of the third pair of ribs). Exploration revealed that the oesophagus was contused over a 5 cm area and a small full-thickness perforation was present in its left hand side. The bone could be palpated within the oesophageal lumen. The neurovascular bundle containing the left recurrent laryngeal nerve was gently retracted using a vascular loop. The oesophagus was then fully exposed circumferentially from its surrounding connective tissue by blunt dissection. Stay sutures of 1.5 metric polypropylene were placed in the oesophageal wall, on either side of the foreign body, to allow minimally traumatic manipulation, and the the area around the oesophagus was packed with moist gauze swabs.
A 3 cm left-sided oesophagotomy was initially performed, starting at the level of the perforation. The foreign body was removed in one piece (Fig 3). The oesophageal mucosa was discoloured and grossly necrotic. Another area of perforation, dorsal to the one identified first, was uncovered. An oesophagectomy, with removal of the whole 5 cm length of damaged oesophageal wall, was then carried out (Fig 4).
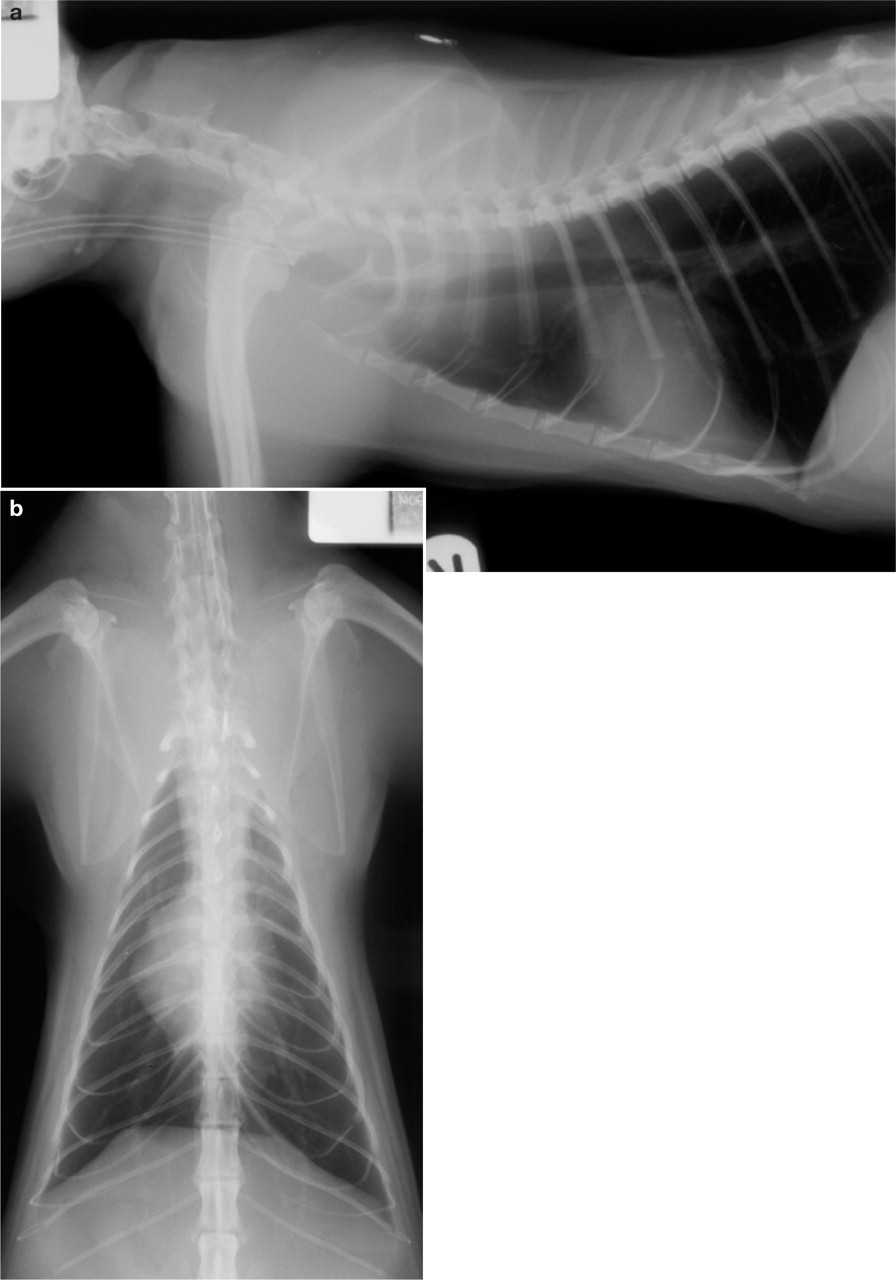
Radiographs taken under general anaesthesia, before oesophagoscopy. (a) Right lateral cervical and thoracic view; the bony oesophageal foreign body is visible at the level of the thoracic inlet/cranial oesophagus and is pushing the trachea ventrally. (b) Ventrodorsal cervical and thoracic view. The bony oesophageal foreign body is much more difficult to see due to superimposition by the caudal cervical and cranial thoracic vertebrae

Right lateral cervical and thoracic radiograph taken under general anaesthesia, just after oesophagoscopy and before surgery. Subcutaneous emphysema, pneumomediastinum, pneumothorax, pneumoperitoneum and gastric dilatation are all evident. Note that the bony oesophageal foreign body is still visible at the thoracic inlet, located slightly more cranially than it was before oesophagoscopic retrieval was attempted
A manual end-to-end anastomosis was performed using 1.5 metric polydioxanone in a single layer, full-thickness, simple interrupted pattern, with mild tension across the anastomosis site being overcome with the use of preplaced stay sutures. A mild to moderate amount of tension was present on completion of the procedure. The surgical site was copiously lavaged with 1 litre of warm sterile saline solution. The perioesophageal area was swabbed and a specimen sent off for microbial culture and sensitivity testing.
Surgeons’ gloves and instruments were changed, and a 1/4 inch Penrose drain was placed in the cervical wound, exiting on the left side. The sternotomy was closed with a combination of simple interrupted and figure-of-eight (around the sternal synchondrosis) patterns using 3.5 metric polydioxanone. The tissues were closed routinely in three layers. No thoracotomy tube was placed. A 16 French gauge de Pezzer silicone gastrostomy tube was then surgically placed via a ventral mid-line coeliotomy. The stomach wall was pexied to the left hand side of the abdominal wall and the site was omentalised before primary closure of the abdomen.
Orthogonal radiographs of the thorax and cranial abdomen were repeated postoperatively (Fig 5). These demonstrated the presence of a moderate pneumothorax, which was successfully drained by a single thoracocentesis. The cat maintained normal spontaneous ventilation and oxygenation throughout her recovery.

Oesophagotomy and retrieval of the oesophageal bony foreign body. (Cranial is to the right of the photograph and caudal is to the left)

Intraoperative visualisation of the grossly necrotic segment of the cervicothoracic oesophageal junction. The foreign body has been removed. Full-thickness 1.5 metric polypropylene sutures are visible in the cranial and caudal part of the oesophageal wall. (Cranial is to the right of the photograph and caudal is to the left)
Postoperative recovery and follow-up
The cat made a steady but good recovery (Fig 6). Analgesia was provided for the following 48 h by means of intravenous administration of methadone (0.2 mg/kg q4h) (Physeptone; Martindale) and then buprenorphine (0.02 mg/kg q8h) (Vetergesic; Reckitt Benckiser). Oral meloxicam (0.05 mg/kg q24h) (Metacam; Boehringer Ingel heim) was started on the day after surgery and continued for 7 days. Potentiated amoxicillin (20 mg/kg PO q12h) (Noroclav; Norbrook) was continued postoperatively.
Two bacterial strains — haemolytic Escherichia coli and Pasteurella species — were isolated on microbial culture. Both were sensitive to potentiated amoxicillin, which was administered for a total of 12 days after surgery. The Penrose drain was removed 2 days after the procedure, as minimal amounts of serous fluid were present at the time. Gastrostomy tube feeding, with an instant convalescence diet (Liquid Concentration Diet; Royal Canin), was started approximately 16 h after surgery. No food was fed by mouth, all oral medication was administered via the gastrostomy feeding tube and water consumption was only allowed after the fourth postoperative day.

Right lateral cervical and thoracic radiograph taken under general anaesthesia, just after surgery but before thoracocentesis. The bony oesophageal foreign body has been removed surgically. Note the presence of ventral cervical and ventral abdominal skin staples

The cat a few days after surgery
Oral food intake was resumed on the sixth postoperative day. Small amounts of wet food were fed and the cat tolerated this well for the first 24 h. However, on the seventh postoperative day, she started to regurgitate and vomit. The vomiting responded to medication with maropitant (0.5 mg/kg q24h SC) (Cerenia; Pfizer) but the regurgitation persisted for another 24 h. These episodes of regurgitation were observed independently from feeding, typically 1–2 h after the feeds, and were seen on five occasions over a 36 h period. An oesophagogram was performed on the eighth postoperative day (Fig 7). The study showed evidence of bolus formation and passage through the oesophageal lumen into the stomach. Some accumulation of contrast medium in the oesophageal lumen suggested a degree of abnormal oesophageal motility. However, no focal narrowing of the oesophagus was identified.
Maropitant was continued for another 5 days and ranitidine (3.5 mg/kg PO q12h) (Zantac; GlaxoSmithKline) was given over a 4-day period. By then, the previously displayed signs of vomiting and regurgitation, along with the anisocoria, were no longer present. The amount of oral feeding was progressively increased, while the amount of gastrostomy tube feeding was progressively decreased and eventually stopped on the 12th postoperative day. On that day, the plan was to remove the gastrostomy tube under light sedation. However, the mushroom tip of the de Pezzer tube fractured and the cat had to be anaesthetised and the fractured tip retrieved by endoscopy.
The oesophagoscopy allowed us to observe the intraluminal appearance of the surgical anastomosis. A small granulomatous lesion was present at the left ventrolateral aspect of the anastomosis but the overall patency of the oesophagus was preserved and only a very minimal degree of oesophageal narrowing was appreciated.

Oesophagogram obtained on the eighth postoperative day. The cat is conscious and has just swallowed a slurry containing barium. The bolus is going through the surgical site with no obvious area of oesophageal narrowing. Some contrast medium in the stomach confirms that the food/barium boluses are transported normally towards the aboral part of the oesophagus
The cat was discharged 13 days after surgery. At this stage, she was on no medication and could eat soft food normally. Soon after discharge, the cat started to be fed on a progressively increased amount of dry food, in order to allow her oesophageal musculature to work harder, with the aim of preventing excessive fibrous scar tissue formation and avoid development of an oesophageal stricture. The cat continued to recover well at home. She was reportedly normal at the last follow-up conversation with the owner 8 months later.
Discussion
Obstructive oesophageal foreign bodies have only rarely been reported in cats. 1–4 Indeed, in a recent study all of the obstructive digestive foreign bodies in 21 cats were aboral to the oesophagus. 5 In cats, fishhooks, needles and string foreign bodies are by far the most common. 6
Of the previously reported oesophageal cases, most presented with obstructive trichobezoars (presumably lodged in the oesophagus when vomited from the stomach) and only one was bony in nature. 3 This is very different to the situation in dogs where up to 89% of oesophageal foreign bodies can be bone. 7
There are four narrowed areas in the oesophagus where a foreign body could become lodged: the cricopharyngeal sphincter, the thoracic inlet, the heart base and the oesophageal hiatus. Obstruction may potentially lead to perforation due to sharp projections on the foreign body, chronicity of the lesion, progressive necrosis of the oesophageal wall and/or traumatic attempts to remove the foreign body. To the authors’ knowledge, no feline case has previously been reported with concurrent perforation of the oesophagus.
The cat's clinical signs, along with its physical examination and radiographic findings, made the identification of an oesophageal foreign body quite straightforward. Clinical and radiographic signs were initially not consistent with aspiration, mediastinitis, pneumomedi-astinum, pleural effusion or pneumothorax.
Removal of oesophageal foreign bodies is considered an emergency procedure because the longer an object remains in the oesophagus, the higher is the risk of aspiration and oesophageal wall injury due to pressure necrosis. 8 Non-surgical retrieval, under endoscopic guidance, was initially attempted as it is associated with lower morbidity and mortality than is surgical removal. 9 In two canine studies, oesophageal foreign bodies were successfully removed by endoscopy in 92% (63% were extracted orally and 29% were pushed into the stomach) and 84% of cases. 10,11 Despite careful manipulation of the foreign body in the present case, haemorrhage occurred, presumably due to the inflammation within the oesophagus. A sudden drop in oxygen saturation and arterial blood pressure, and increase in the fraction of expired carbon dioxide, revealed that a tension pneumothorax was developing, secondary to a perforation. This perforation might have been caused by endoscopic manipulation of the embedded foreign body within the surrounding friable oesophageal segment, or may have been present for some time but only became evident when the foreign body was dislodged.
Inability to remove the foreign body endoscopically, and perforation of the oesophagus with sufficient leakage to induce a rapidly developing, life-threatening pneumomediastinum and pneumothorax, represented indications for immediate surgical exploration of the area. 9 Such management is also supported in the human literature. 12 Inspection of the oesophagus at the thoracic inlet revealed a large, circumferential necrotic area that necessitated oesophageal resection and anastomosis. The length of the oesophagus that can be resected without undue risk of dehiscence is limited by anastomotic tension. In canine clinical patients, resection of more than 3–5 cm of the oesophagus increases the risk of dehiscence, 6 and this is assumed to be the same for cats.
Due to the large size of the oesophageal defect in this cat, an adjunctive technique such as a circumferential partial myotomy, 13 an ‘onlay’ patch (using omentum, local muscle flaps or pericardium) 9 or an oesophageal substitution technique 9 could have been considered. In an experimental model of oesophagoplasty in cats, the pericardium has been used successfully as a substitutive allograft in 12 individuals. 14 All of these patients survived the procedure until euthanasia, even though 11/12 developed a degree of oesophageal stenosis and 8/12 developed adhesions between the pericardial autograft and the surrounding lung lobes and/or mediastinum. The authors decided in this case that the tension at the anastomotic site was not great enough to require an adjunctive technique.
In this case, preplaced stay sutures were used to facilitate gentle tissue handling, maintain alignment and distribute tension evenly during simple reapposition of the oesophageal ends with a single layer, full-thickness suture pattern. The oesophageal wall furthest away from the surgeon was sutured first. Oesophageal anastomoses can also be performed with a double layer suture pattern or with surgical stapling equipment, 9,15 but the authors chose a single layer technique in this case for speed and simplicity, and because the space at the surgical site would not have permitted the use of stapling equipment. In this cat, perioperative antibiotics were administered due to the contaminated nature of the procedure. 16 There is also evidence in the literature that perioperative administration of systemic antibiotics lowers the rate of oesophageal anastomotic leakage and postoperative mortality. 17
The most commonly reported complications of oesophagectomy are anastomotic leakage, ischaemia and necrosis, and stricture formation. 18 The anastomosis healed and stricture formation did not occur, as shown by our radiographic findings 1 week postsurgery and our oesophagoscopic findings 12 days post-surgery. Oesophageal rest, enabled by the gastrostomy tube, was probably an important feature of this cat's management. Theoretically, corticosteroids could reduce the risk of stricture formation after oesophageal resection and anastomosis because they reduce fibrosis and collagen formation. However, in a controlled study of children with oesophagitis induced by caustic substance ingestion, oral steroids were not shown to be beneficial. 19 No controlled studies in animals have evaluated the use of systemic steroids after oesophageal stricture dilation or oesophageal surgery. In humans, it is recommended that normal swallowing mechanisms should be verified before the patient resumes oral intake. 20 This cat resumed normal grooming behaviour within 3 days of the surgery and, in doing so, demonstrated normal swallowing abilities.
In one retrospective survey of endoscopic and surgical treatment of oesophageal foreign bodies in dogs and cats, 66% of the animals with a diagnosed oesophageal perforation died. 21 Based on previous studies in human and veterinary medicine, and our experience with this case, we suggest that the following factors are important considerations when managing feline patients with a perforating oesophageal foreign body: prompt surgical intervention; the ability to convert to a surgical procedure under the same anaesthetic as a non-surgical retrieval; placement of a gastrostomy tube to allow oesophageal rest; and the availability of advanced anaesthetic and critical care support.