
Abstract
Alison Joyce and David Yates


The role of early neutering in cat welfare
The Royal Society for the Prevention of Cruelty to Animals (RSPCA) is the oldest and largest animal welfare charity in the world and one of the largest independent charities in the UK. The RSPCA uses a number of indicators to measure pet animal welfare. 1 In cats, these include the number of unwanted healthy cats taken into the care of the RSPCA; the number of non-microchipped cats taken into RSPCA care and the number of animal welfare complaints investigated by RSPCA inspectors.
In 2009, the RSPCA investigated approximately 24,000 complaints where the primary animal was a cat. 2 In the same year, over 8000 cats (the vast majority without a microchip, unpublished data) were admitted to the charity's nationally operated regional animal centres. The major reasons for entry into RSPCA care are listed in Table 1.
Animal charities have attempted to improve cat welfare using neutering initiatives to combat pet overpopulation. 3 For the cat population to reduce, the death rate must exceed the birth rate in a given time period. Life expectancy is increasing in the domestic cat; 4 therefore, a more profound effort must be directed towards suppressing reproduction in the cat. In free-roaming cats, annual euthanasia of at least 50% of the population has been suggested as a more effective means of control than neutering. 5 This is unlikely to receive favour as a method of population management, but highlights the magnitude of the control effort required. For owned cats, up to 70.5% of litters may be unplanned. 6 Consequently, early neutering remains the most appropriate surgical technique for long-term population control in both stray and pet cats.
Major reasons for cats to enter into RSPCA care

Definition of early-age neutering
Early neutering, or prepubertal gonadectomy, may be defined as neutering by 4 months of age — typically at between 6 and 14 weeks. 7 Puberty is the onset of reproductive and sexual maturity, and is consistent with the first oestrus in the female and production of functional spermatozoa in the male. 8 In the queen the timing of first oestrus is variable but, on average, it occurs between the ages of 8 and 10 months. 9,10 Exceptional cases of pregnancy may be seen as early as 4 months (Fig 1). The onset of puberty in tom cats is more consistently between 8 and 10 months of age. 11
When to early neuter
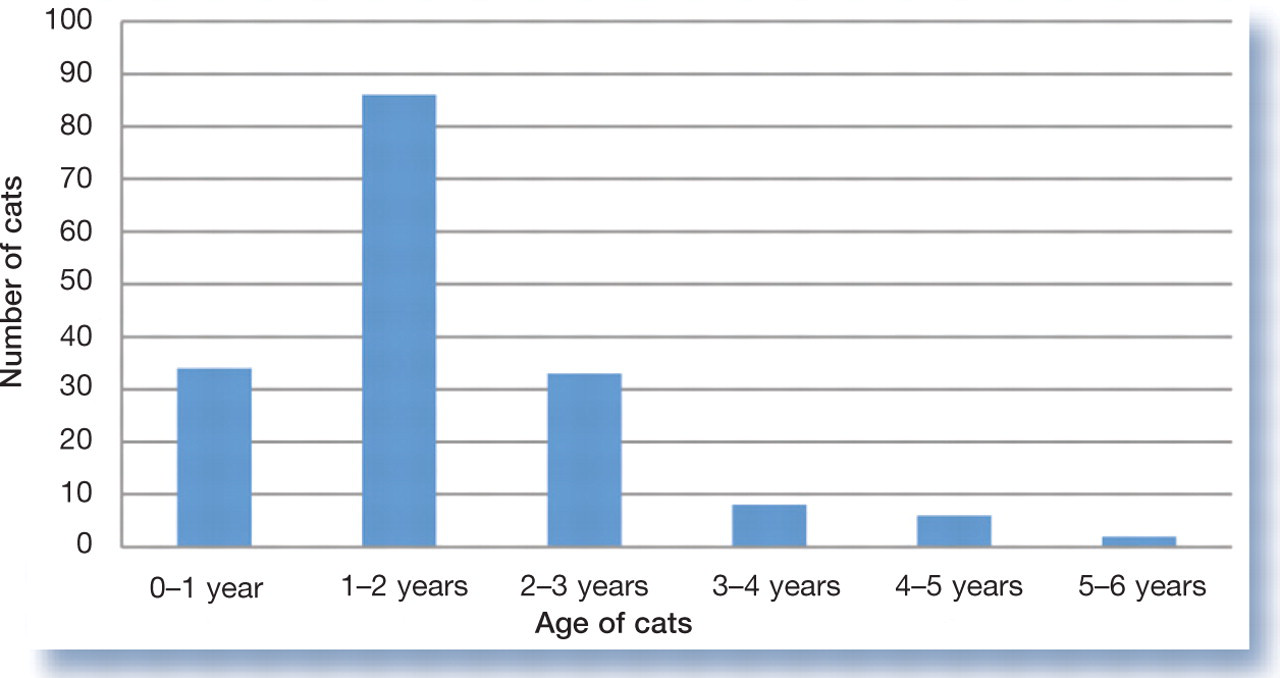
Age of kittens/cats confirmed pregnant at the point of elective neutering by the RSPCA Greater Manchester Animal Hospital 2005–09. Two cases were less than 4 months of age at surgery
Reasons to early neuter
Short- and long-term studies, up to 11 years post-procedure, have found no physical and few behavioural problems following early neutering in cats. 14,15 Male kittens that underwent early castration had a significantly lower incidence of abscesses, sexual behaviours, urine spraying and aggression towards veterinarians. In both sexes, the occurrence of asthma, gingivitis and hyperactivity was also reduced. 15 Shyness and hiding were the only behaviours found to increase in those animals neutered before 5.5 months. 15
Cats spayed before 6 months of age showed a 91% reduction in the risk of mammary carcinoma compared with intact cats. 16
What are the common concerns and how valid are they?
Health and physical sequelae
Speculated associations between early castration and the occurrence of feline lower urinary tract disease (FLUTD) may have led to a reluctance to perform prepubertal gonadectomy. 17,18 Yet long-term retrospective studies have actually documented a decreased occurrence of FLUTD in prepubertal gonadectomised males, 14 with further complementary work cementing the lack of correlation between age at neutering and the incidence of FLUTD. 15 Urethral diameter and urethral dynamic function measured by urethral pressure profiles were found not to vary between male cats neutered at 7 weeks, 7 months or as intact adults. 17
The external genitalia retain an infantile appearance in early-neutered cats. For males, the development of penile spines is dependent on androgenic stimulation, hence prepubertal gonadectomy results in a smooth glans penis. 8 In females, an infantile vulva exists, but the perivulvar dermatitis that is seen in some bitches with an infantile vulva does not appear to be a clinically significant problem in cats. 19
Neutering is a commonly associated risk factor for obesity. Metabolic rate has been shown to decrease in cats after gonadectomy, 20,21 and cats neutered at 7 weeks or 7 months were found to have a higher body mass and body condition score, and increased falciform fat, in comparison with intact cats. 14,22 Longer term studies found no correlation, however, between age at gonadectomy and obesity. 15 A predisposition for obesity is mulitfactorial and other uncontrolled variables such as diet, exercise and genetics make it difficult to determine solely the effects of neutering on obesity. Advice should be given to owners at the time of neutering about subsequent risks of obesity and that changes in diet and exercise may be necessary.
Prepubertal gonadectomy has been associated with delayed physeal closure of long bones. Distal radial physeal closure occurred approximately 8 weeks later for cats neutered at 7 weeks and 7 months compared with intact cats, although this was not found to affect adult size. 23 No clinical relevance of delayed physeal closure has been demonstrated. 15
Neutered cats are reported to be 8.7 times more likely to develop diabetes mellitus than their intact counterparts, 24 although no correlation between timing of neutering and risk of developing diabetes mellitus has been identified. Other risk factors are important — notably, breed, gender and increasing age.
Surgical risks
Short-term studies, during, immediately after and up to a week after early neutering, identified no increased surgical or anaesthetic risks associated with the procedure. 25,26
Prepubertal gonadectomy allows for more expedient surgery. 7,25 Lack of abdominal and bursal fat enables good visualisation and accurate haemostasis of small blood vessels (essential for minimising blood loss in animals with a relatively small blood volume). 27 A smaller incision is required and use of intradermal absorbable skin sutures eliminates the need for Elizabethan collars and/or postoperative checks. A lower rate of postoperative wound infections has also been documented following prepubertal compared with traditional-age neutering. 26
In 2009, the 3-day spay morbidity at the RSPCA Greater Manchester Hospital, defined as presentation at the hospital for a complication related to the spay procedure within 72 h of discharge, was less than 0.1% for early neuters, which is directly comparable to figures for complications resulting from traditional-age neuters at the hospital (unpublished data).
Anaesthesia for early-age neutering
Choice of agent/protocol
The paediatric period covers approximately the first 12 weeks of life and, from a physiological point of view, is unique (see box on page 6). Consequent differences in pharmaco-kinetics and pharmacodynamics contribute to increased sensitivity to drugs, prolongation of effects and a limited capacity for cardiovascular compensation. Clearly, this has important implications in terms of anaesthesia, and the choice of protocol requires careful consideration. Table 2 lists a number of protocols that have been used successfully for early-age neutering. The so-called ‘quad’ protocol was derived at the authors’ hospital.
Useful protocols for general anaesthesia in kittens undergoing early-age neutering

∗Atipamezole (Antisedan; Pfizer) is recommended as a reversal agent, at 10–50% volume of the previously administered medetomidine (Domitor; Pfizer), no sooner than 20 mins after initial intramuscular injection. Note that its use at 10% volume is unlicensed in cats
○The dosing protocol for the quad protocol, whereby equal volumes of each drug are administered IM, is given on page 7
Paediatric physioslogy — the implications for anaesthesia
Normal physiological measurements in kittens
Cardiac output is predominantly dependent on heart rate in paediatric animals. 28 The immature heart has a higher proportion of non-contractile cardiac tissue, limited ventricular compliance and thus a predetermined stroke volume that can poorly compensate for drug-related changes. 29,30 An immature sympathetic nervous system also restricts the ability to increase heart rate and contractility in response to drug-induced bradycardia, as seen with the use of α2 agonists; as such, the risk of hypotension developing is high. 30 Added to this, small volumes of blood loss, as little as 5 ml/kg, can have deleterious effects on paediatric blood pressure. 28,30,31
Tissue oxygen consumption, and consequently respiratory rate, are two to three times higher in paediatric patients. 30,32 Compliant lung and chest walls also mean that ventilation is less efficient and that the work of breathing is greater. Respiratory depression, respiratory disease or airway obstruction can thus result in severe hypoxaemia and ventilatory fatigue. 29
Practical implications
Oxygen should be provided throughout ovariohysterectomy even if anaesthetic depth and relaxation are adequate. Maintenance of a patent airway with endotracheal intubation is essential. Increased airway resistance and risks of obstruction are a result of a relatively narrow upper airway and larger tongue in the paediatric patient. Anaesthetic circuits require minimal resistance to airflow and minimal dead space. An appropriate and popular choice is the modified Ayre's T-piece, valveless or valved (Mapleson D). 28 High fresh gas flow rates are required to avoid rebreathing and should be calculated prior to surgery:
Practical implications
Attempts to minimise heat loss should be made:
– perform moderate hair clipping and minimal wetting at surgical preparation;
– use insulating materials such as reflective foil sheets and bubble wrap;
– use warming devices (eg, Bair Hugger);
– maintain an ambient temperature >20°C;
– most importantly, minimise the duration of anaesthesia/surgery. 33
Returning kittens to littermates is encouraged once a similar stage of recovery or standing is reached. This aids return to feeding and play, and minimises stress during in-patient stay.

Hypoalbuminaemia exists up until about 8 weeks of age, potentiating the effects of highly protein-bound drugs such as propofol. Immature hepatic enzyme systems persist up to 12 weeks of age, reducing the speed and capacity for drug transformation and metabolism and so prolonging effects. 28 Similarly, immature glomerular filtration rate and reduced renal blood flow affects the termination of drugs that are cleared via excretion. A reduced ability to concentrate urine means paediatric patients are more prone to dehydration.
Practical implications
The choice of anaesthetic agent/protocol needs careful consideration (see text). Water should not be restricted for more than an hour prior to surgery. 34 However, careful consideration should be given to supplementary fluid administration, as a kitten's cardiovascular system cannot tolerate large volumes of fluid.
Derivation of the ‘quad’ protocol
Early neutering has been performed at the RSPCA Greater Manchester Animal Hospital for almost 10 years. Experience gained in that time has been that current licensed intra-muscular protocols do not achieve reliable anaesthetic depth in kittens of lower body mass, most notably those under 1.5 kg. Dosing inadequacies in particularly small kittens have been attributed to a greater body surface area (BSA) to mass ratio, and this led to the derivation of the ‘quad’ protocol. 35
The dose of medetomidine was recalculated based on BSA, initially at 1000 μg/m 2 . Fig 2 compares volumes of medetomidine (Domitor; Pfizer) for body mass dosing based on BSA and body weight. As illustrated, cats of lower body mass (<2.2 kg) receive higher volumes of medetomidine if dosing is based on BSA.
Ketamine is a popular choice in anaesthetic combinations in cats because it is an induction agent (with a wide therapeutic index) providing somatic analgesia via the intramuscular route. Midazolam (Hypnovel; Roche Products) was incorporated to enhance muscle relaxation and sedation. It facilitates a reduction in the medetomidine dose (and subsequent cardiovascular depression) and, furthermore, its appetite-stimulating effects promote feeding on recovery. 36 This is of particular importance in reducing hypo-glycaemia and hypothermia in kittens. To provide multimodal analgesia, peri- and postoperatively, buprenorphine (Vetergesic, Alstoe; Buprecare, Animalcare) was added. Buprenorphine was chosen preferentially over butorphanol for the longevity of postoperative analgesia (6–12 h compared with 1–2 h). It has also been shown to produce mild to moderate increases in body temperature, thus helping to prevent post operative hypothermia. 37

Comparison of volumes of medetomidine for dosing cats based on body surface area (red line) and body weight (blue line)
Quad protocol — calculation of drug volume
Step 1: body mass is converted to body surface area (BSA):
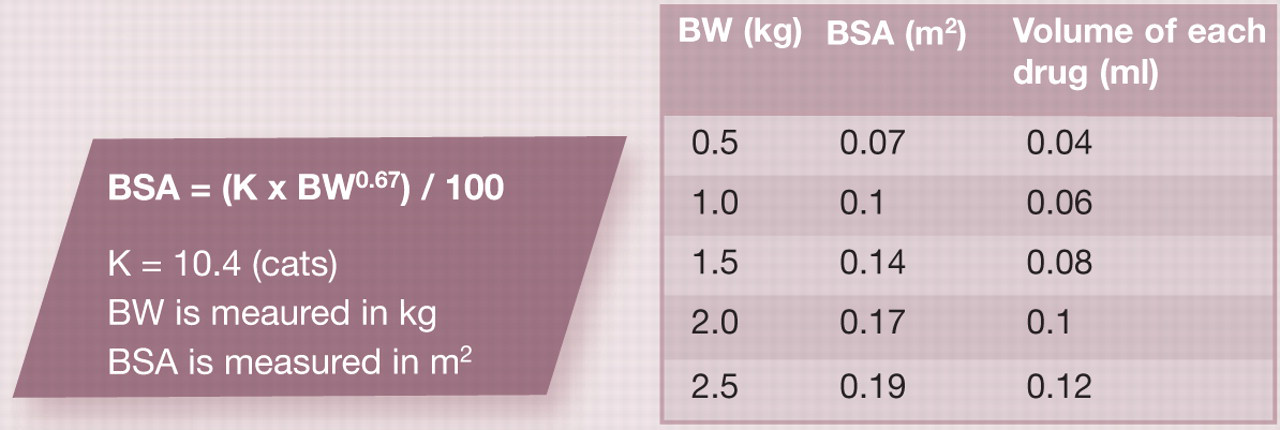
Step 2: BSA multiplied by a factor of 0.6 gives the volume of each agent in the quad combination (see table).
As shown in the box above, a very practical benefit of the quad protocol is that equal volumes of each drug are administered as a single intramuscular injection.
Monitoring
The anaesthetist should carefully monitor vital signs — heart rate, respiratory rate, temperature, capillary refill time and mucous membrane colour. Additional monitoring equipment should be selected carefully to avoid prolonging the length of anaesthesia. Precordial or oesophageal stethoscopes are most useful in monitoring heart and respiratory rates. Pulse oximetry, capnography and Doppler are other non-invasive monitoring techniques available for use in paediatrics. Readings can be unreliable, however, and as such their use should be well researched. Core temperature should be regularly recorded via an oesophageal or rectal probe.
A parameter that is not routinely monitored is blood glucose, yet hypoglycaemia may contribute to a prolonged recovery. Blood glucose can be measured using a test strip from a percutaneous sample. If levels fall below 5 mEq/l supplementation should be instituted, using either 5% dextrose (10 ml/kg/h) or oral glucose if the kitten can swallow. 33 Medetomidine may cause a rise in blood glucose level during the anaesthetic period by reducing endogenous insulin secretion. 38
Surgical approaches
The important practical considerations for early neuter (ovariohysterectomy and castration) surgeries — beyond those discussed above relating to anaesthesia — are outlined in the boxes on pages 8 and 9.
Surgical notes: early ovariohysterectomy
Preparation
Induce anaesthesia using an appropriate protocol (see text).
Recheck sex of the kitten.
Administer a subcutaneous non-steroidal anti-inflammatory injection (0.3 mg/kg meloxicam [Metacam; Boehringer Ingelheim]).
Gently express the bladder to optimise abdominal visualisation and reduce the risk of complications such as ureteral damage.
Provide corneal protection by applying eye lubricant to both eyes (eg, Viscotears, Novartis; Lacri-lube, Allergan).
Endotracheal intubation requires that a range of uncuffed endotracheal tubes (1.0–3.5 mm) is available. Local anaesthetic spray (2% lidocaine hydrochloride [eg, Intubeaze; Dechra Veterinary Products]) is applied to the larynx to prevent stimulation of the laryngeal reflex, and an appropriate-sized tube is selected. 33 A laryngoscope and good light source aid intubation.
Identify landmarks for a midline incision:
– <12 weeks of age: a relatively caudal incision is made, approximately two-thirds the distance from umbilicus (image a) to pubic brim (image b);
– >12 weeks of age: the incision is made equidistant from umbilicus to pubic brim.
Ovariohysterectomy (images c-j)
A moderate hair clip and minimal wetting throughout surgical preparation reduces the risk of hypothermia. Waterproof, disposable drapes are useful.
Make a surgical incision, approximately 10–20 mm in length. Minimal blunt dissection of the subcutaneous tissue is required to expose the linea alba. Enter the abdomen carefully.
A larger volume of abdominal serous fluid (specific gravity <1.020) may be seen in early neuters.
Reflect the bladder and carefully identify the uterus. The left horn runs over the descending colon and the bifurcation of the uterus can be seen close to the bladder neck. Tissue handling should be minimised and performed delicately to avoid excessive bleeding or trauma.
Spay routinely. The uterus is immature and taut but the ovaries are relatively easy to expose with gentle traction. Expose the left ovary first and clamp using three small haemostats. Ligate the ovarian and uterine vasculature using an appropriate-sized suture material (1.5–2 metric polyglactin 910 [Vicryl; Ethicon] or chromic catgut). Repeat for the right ovary.
Trace the uterine horns to the cervix and double ligate. Transfixing ligation is not necessary due to the immaturity of the vasculature.
Perform a routine three-layer abdominal closure:
– Muscle layer: simple interrupted or continuous sutures using 1.5–2 metric polydioxanone (PDS; Ethicon);
– Subcutaneous tissue: simple continuous sutures using 1.5 metric undyed poliglecaprone 25 (Monocryl; Ethicon);
– Skin: simple interrupted or continuous intradermal pattern using 1.5 metric undyed poliglecaprone 25. Final continuous knots should be buried using an Aberdeen knot.
Postoperative care
Extubate postoperatively to prevent laryngeal stimulation, oedema and tracheal damage.
Continue to insulate in recovery; an incubator may be used for particularly young kittens (image k). Return kitten to littermates at an appropriate time.

Raising awareness and overcoming tradition
Evidence-based studies on kittens following early neutering document shorter recovery times, lower morbidity and equivalent mortality rates compared with traditional-age neuters. 26 Furthermore, long-term studies have found similar behavioural and physical outcomes when contrasting the two neutering age groups. 14
Surgical notes: early castration
Preparation
Induce anaesthesia using an appropriate protocol (see text). Intubation is not usually necessary for male kittens, but should be considered if unfamiliar with the techniques of early castration.
Oxygen supplementation is recommended via mask or endotracheal tube and should be determined on a case-by-case basis.
Recheck sex and ensure the presence of both testicles. The testes are descended at birth but move within the inguinal canals until puberty. 11 Approximately 1% of kittens may be cryptorchid and the procedure should be delayed until 6 months if it is not possible to palpate both testes. 39
Castration
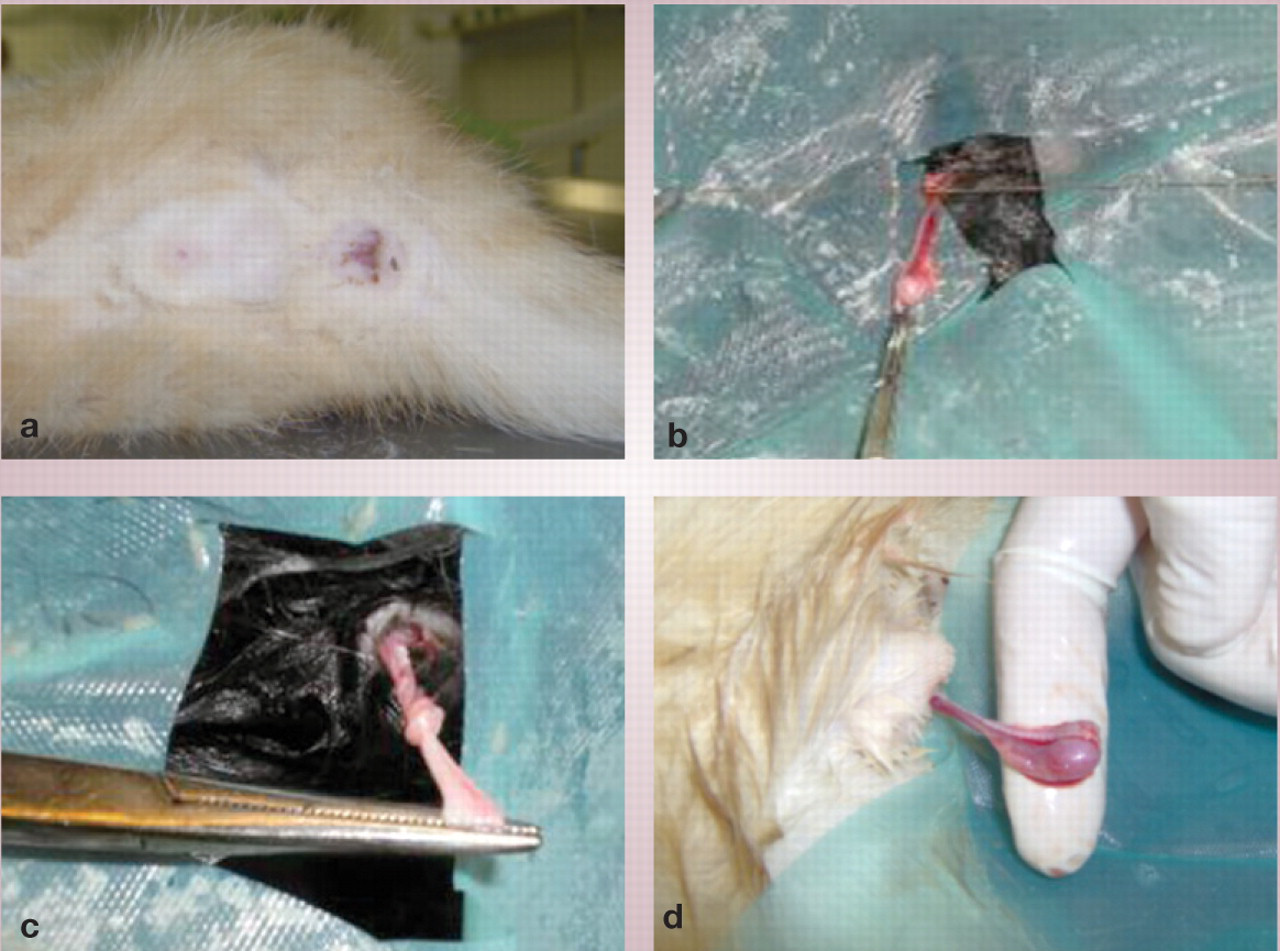
Bilateral scrotal incisions are made directly over the testes as the scrotum is undeveloped. The normal anatomy of a male kitten at 10 weeks of age, prior to scrotal incision, is shown (image a).
Three methods of castration are possible:
– Spermatic bundle is ligated with fine absorbable suture material (catgut or Vicryl; Ethicon) (image b) — open or closed castration. This method is particularly useful in very small kittens <10 weeks old.
– Spermatic bundle is tied on itself using haemostats (image c) — open or closed castration.
– Spermatic vessels are tied off with ductus deferens in an open castration (image d).
Postoperative care
Skin incisions are left to heal by secondary intention.
Support for early neutering
The American Association of Feline Practitioners (AAFP) recently released a position statement sanctioning early neutering, which is published on page 58 of this issue of J Feline Med Surg. Endorsements and support have also been issued by the American Veterinary Medical Association (AVMA), American Animal Hospital Association (AAHA), American Humane Association (AHA), Humane Society of the United States (HSUS), Association of Shelter Veterinarians, American Society for the Prevention of Cruelty to Animals (ASPCA), Society for Theriogenology, American College of Theriogenologists, 7 The Cat Group (see also pages 56–57 of this issue), 3 RSPCA and the International Society of Feline Medicine (ISFM).
Promotion of early neutering has the potential to have a significant impact on the cat population. Its implementation in both shelter medicine and private practice can be more extensive and successful with increased awareness and education of veterinarians and cat owners alike. An increasing number of studies, veterinary organisations and animal welfare charities (see above) support the concept of early neutering. However, with currently only about 28% of veterinarians in UK private practice agreeing with neutering between 12 and 16 weeks, 40 tradition must be further overcome to achieve a wider spread of approach to cat population control.
KEY SURGICAL POINTS
Withhold food (only) for a maximum of 3–4 h prior to surgery (2–3 h if <8 weeks old).
Keep kitten with littermates to reduce pre-operative stress/excitation.
Weigh the kitten — use scales accurate to two decimal places.
Consider the body surface area (‘quad') protocol for anaesthesia.
Minimise patient handling prior to induction.
Use an appropriate method of induction — intramuscular is preferred.
Perform a moderate hair clip and use minimal wetting during surgical preparation.
Maintain ambient temperature >20°C.
Use insulation throughout (eg, reflective sheets, Bair Hugger warming device).
Minimise the duration of general anaesthesia and surgery.
Ensure delicate, minimal tissue handling.
Feed kitten once it is standing.
Return kitten to its littermates for recovery.