
Abstract
Clinical report
An 11-week-old female entire domestic shorthair cat weighing 1.2 kg was referred to the Royal Veterinary College, London, for further investigation of constipation since weaning. The owners reported the kitten defecated once every 2–3 days with frequent episodes of tenesmus and pain. No haematochezia or mucochezia was reported and a mixture of dry solid faeces and diarrhoea had been noted. The kitten was otherwise very bright with a normal appetite, although she was smaller than her littermates which were apparently clinically healthy. Lactulose (Lactulose; Novartis), 2 ml q8h PO for 4 days, had been prescribed and resulted in some improvement in the constipation. A combination of proprietary dry and wet kitten food was being fed.
On physical examination, the kitten was bright and alert. She was an appropriate size and proportionately grown. The abdomen was distended, with a large volume of firm faeces palpable in the colon, and the anus was inflamed. The rest of the physical examination was unremarkable. The differential diagnoses at this time included congenital megacolon, structural gastrointestinal anomaly, colonic stricture or congenital hypothyroidism.
Venous blood gas and electrolyte analysis was within normal limits and serum thyroxine was just below the reference range (18.8 nmol/1, reference range 19–65 nmol/1). Urinalysis of a free catch urine sample revealed a specific gravity of 1.017 and a pH of 7; sediment examination was unremarkable. Right lateral and ventrodorsal abdominal radiographs showed a lack of serosal detail and a large volume of faeces in the descending and transverse colon (Fig 1).

Lateral abdominal radiograph showing reduced serosal detail, and a large volume of faeces in the descending and transverse colon
Two sodium citrate/sodium alkylsulphoacetate enemas (Microlax; UCB Pharma) were administered 12 h apart, resulting in the passage of two 1 cm diameter firm faecal balls. The kitten was anaesthetised with pethidine (Pethidine; Martindale Pharma) 4 mg/kg IM as a premedicant followed by propofol (Vetofol; Norbrook) 6 mg/kg IV at induction. Anaesthesia was maintained with isoflurane (Isocare; Animalcare) in oxygen delivered via a non-rebreathing system, with endotracheal intubation. Ten millilitres of warm water were used as an enema. Subsequent colonoscopy revealed no gross abnormalities from the rectum to the ileocolic valve. No biopsies were taken.
The kitten recovered uneventfully and lactulose 0.5 ml q8h PO was prescribed; the kitten defaecated normally the following day. The option to continue medical management, followed if necessary by subtotal colectomy when the kitten had grown larger, was declined by the owners and euthanasia was requested.
At necropsy the large intestine was moderately dilated (2 cm diameter maximum) and contained soft-formed faecal material. Two small gall bladders, each with a separate bile duct which fused after approximately 3 mm, were present and considered an incidental finding.
A range of tissues was fixed (in 10% formol saline) and processed for histological examination using standard methods. Haematoxylin and eosin (H&E)-stained sections of the large intestine included scarce ganglia within myenteric (Auerbach's) plexi and only marginally more numerous ganglia within submucosal (Meissner's) plexi (Fig 2). No significant histological abnormalities were recognised in the stomach or small intestine. These findings were considered consistent with hypoganglionosis in the large intestine, which was presumed to be congenital due to the history and young age of the animal. Immunohistochemistry for substance P, neurofilament and synaptophysin revealed positive staining of neurons and nerve fibres in a similar location and distribution to the H&E-stained sections.
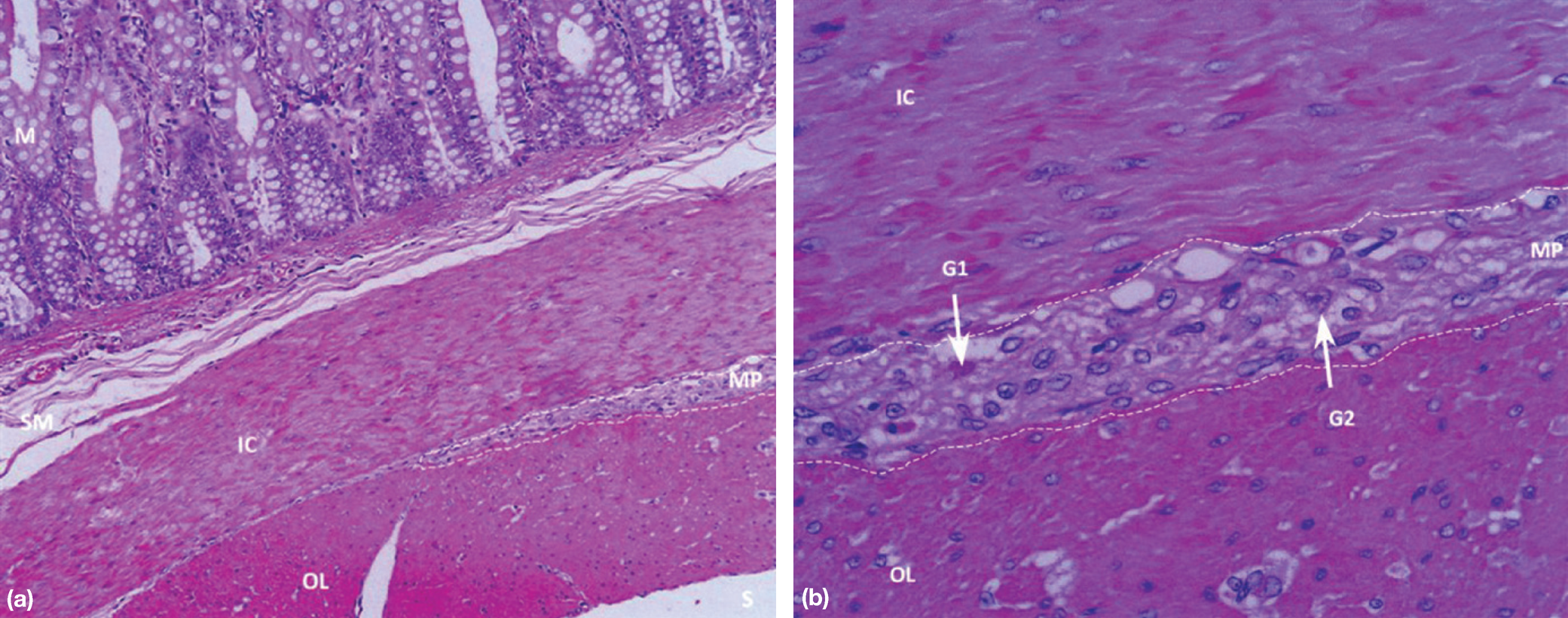
Histological appearance of a section of colon from the kitten. (a) Broken line labelled MP denotes expected site of myenteric (Auerbach's) plexus between inner circular (IC) and outer longitudinal (OL) layers of muscularis externa. S = serosal surface, M = mucosa. Fragmentation of the submucosa (SM) is an artefact in this section. H&E × 200. (b) Higher power view. See above for definitions of MP, IC and OL. Most of the cells visible in the area (MP) bound by the broken lines are support cells. Very rare ganglion cells are recognisable by amphophilic cytoplasm (G1) or by the presence of prominent nuclei (G2). H&E × 400
Discussion
Feline megacolon can be caused by primary (idiopathic, congenital) or secondary (malunion of a pelvic fracture, neuromuscular dysfunction, rectal stricture, neoplasia, metabolic or endocrine disease) abnormalities. 1 Previously reported studies of colonic smooth muscle function in cats with idiopathic megacolon have found disturbances in the activation of smooth muscle myofilaments, but few histological abnormalities of smooth muscle cells or of myenteric or submucosal plexus neurons, 2 in contrast to this case.
Hirschsprung's disease is a well described congenital form of neurogenic megacolon causing severe constipation in children. 3 It results in a functional obstruction due to a lack of ganglion cells of the myenteric (Auerbach's) and submucosal (Meissner's) plexi in the distal colon and is, therefore, similar to this case. Hirschsprung's disease presents, in 90% of cases, in the neonatal period with a history of delayed passage of meconium and signs of bowel obstruction such as vomiting and abdominal distension. 4 Approximately 10% of patients present outside the neonatal period, some into early adult life, with a history of severe constipation and intermittent abdominal distension. Rosin et al suggested the condition may occur in cats; 5 however, a true existence in this species has not previously been documented.
Histologically, ganglia of the myenteric and submucosal plexi are absent in the distal affected bowel in Hirschsprung's disease. Immunoreactivity for retinoblastoma oncoprotein has been reported to be more sensitive than routine H&E stains in identifying ganglion cells. 7 Had immunohistochemistry for retinoblastoma oncoprotein been performed in this case, more numerous ganglion cells might have been identified.
Feline dysautonomia is caused by degeneration of both sympathetic and parasympathetic divisions of the autonomic nervous system and enteric nervous system, whereas the enteric nervous system only was affected in this case. A depletion of immunoreactivity for substance P has been reported for peptidergic neurons throughout the gastrointestinal tract in cats with dysautonomia, 8 and synaptophysin has proved to be a useful diagnostic marker for neuron degeneration associated with this disease. 9 Immunohistochemistry for substance P was positive in this case, indicating the presence of some neurons and nerve fibres, but the synaptophysin expression pattern did not suggest neuron degeneration. A morphometric study using age-matched normal control cats to confirm the hypoganglionosis would have been ideal but was not ethically justifiable. As dysautonomia has been reported in cats as young as 6 weeks of age, 8 it is possible that this was an early case of dysautonomia where sympathetic and parasympathetic neuronal degeneration had not yet developed.
A variety of concurrent congenital anomalies have been reported in around 10% of sporadic cases and 25% of familial cases of Hirschsprung's disease. 4 These vary from regional abnormalities such as megaloureter, hydronephrosis and stenosis of the large intestine, rectum and anal canal, to nonregional anomalies such as aortic and ventricular septal defects. Congenital hepatobiliary abnormalities were not reported in a cohort of 178 patients with Hirschsprung's disease, so the significance of the duplex gall bladder found in the current case is uncertain. 10
Chronic constipation secondary to congenital hypothyroidism has been reported because of decreased gastrointestinal motility. 11 This was considered an unlikely differential in this case due to lack of other clinical signs associated with hypothyroidism — such as disproportionate dwarfism, mental dullness, bradycardia and hypothermia. Thyroxine was probably mildly decreased in this case due to sick euthyroidism.
Although colonic hypo- or aganglionosis was suspected previously in 2% of cases of obstipation in cats, 2 it was not proven. As far as the current authors are aware, this is the first reported case of congenital hypoganglionosis in a kitten with histopathological confirmation of the diagnosis. Given the similarities in age at presentation, clinical signs, radiographic abnormalities and histopathology compared with Hirschsprung's disease in man, which occurs with a frequency of 1 in 5000 live births, congenital colonic hypo- or aganglionosis could be a more common cause of constipation in kittens and young cats than has previously been reported. 4 Further studies of kittens and young cats with constipation would, however, be required to confirm this.