
Abstract


As discussed in the accompanying article on medical treatment (
Critically, corneal surgery should only be embarked on if the surgeon possesses the skills to handle a perforated cornea — which is a risk with any corneal procedure. Apparently innocuous surgeries can rapidly become involved, and it is always best to be prepared for the worst-case scenario.
Equipment and instruments for corneal surgery
Magnification
Corneal surgery requires magnification, and should not be attempted without surgical loupes or an operating microscope (Fig 1). Surgical loupes vary in magnification from 2–8 ×. For the inexperienced user it is easier to start with lower magnifications and work up. The greater the magnification the smaller the field of view, and the smaller the depth of field, both of which can be difficult to adapt to. Slight head movements can render the visual field out of focus, especially at higher magnifications, and some users report a sensation of seasickness until they are comfortable with their use. Taking the time to practise routine surgery with loupes will familiarise the surgeon with the techniques required for successful surgery with magnification. Surgical loupes have a fixed working distance (eg, 42 cm), and this will need to be comfortable for the surgeon (straining the back or neck in lengthy surgeries is a recipe for a short career). Lighting is also an important factor, as wearing surgical loupes will decrease the light available to the surgeon. Some loupes have a light attachment, which is useful; otherwise a good theatre light will be required to provide increased illumination.

(a) Microsurgical loupes (Keeler 5.5×, 42 cm working distance); (b) Operating microscope, capable of magnifications of up to 42×
MEDICAL TREATMENT OF CORNEAL ULCERS
A sister article addressing medical treatment options appears on pages 384–397 of this issue of J Feline Med Surg, and at:
An operating microscope is capable of much greater magnifications and is preferable where this facility is available. Although some experience is required to achieve dexterity under an operating microscope, the skills are an extension of those attained with the use of magnifying surgical loupes.
Microsurgical instruments
Microsurgical instruments are required for corneal surgery and the basic items include:
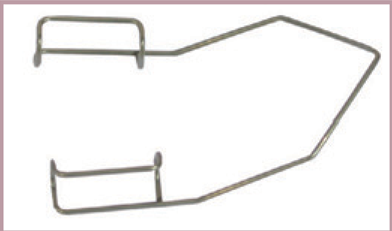
Eyelid speculum (wire Barraquer speculums are a good choice in cats as they are lightweight and avoid pressure on a potentially fragile eye);
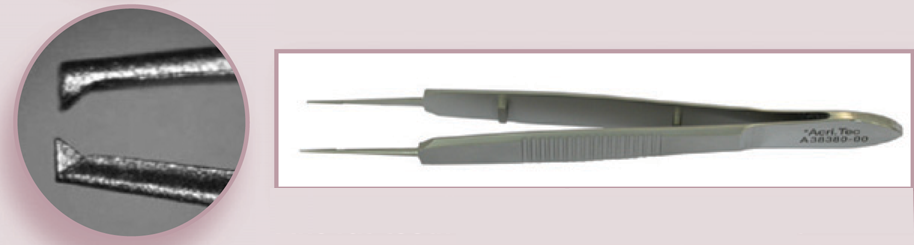
Colibri or fine rat-tooth forceps;
Specialist scalpel blades (beaver blades and handle, crescent knives and restricted-depth knives);
Microneedle holders, without lock, for both 6/0 and 8/0 (or finer) vicryl (those with a lock are best avoided as the action of unlocking may be transmitted down the grasped needle and disrupt delicate tissues);
Westcott tenotomy scissors and Stevens tenotomy scissors.
Use of fine surgical gloves with a textured surface (eg, Biogel M) much improves the ability to handle microsurgical instruments.
Positioning the eye for corneal surgery
Of paramount importance (yet an often overlooked consideration) is the position of the eye — which should be parallel to the surgeon and the operating table. The use of neuromuscular blocking agents to paralyse extraocular muscle function, creating a centrally positioned eye, is ideal for corneal surgery. Unfortunately the need for a ventilator, nerve stimulator and appropriately trained personnel makes this unsuitable in most practices. Stay sutures can be used to hold the eye centrally; however, care must be taken when placing these so that the eye is not perforated by the needle (a superficial bite of sclera is all that is required) and that tissue which may be required for a grafting procedure (eg, conjunctival pedicle graft) is not damaged by the needle or suture material.
Vacuum surgical pillow bags can be used to position the head comfortably for the patient (while ensuring a free airway) and the surgeon. Air is then drawn out of the pillow bag via a small hand-pump and the position fixed. These are excellent and well worth the investment. (It probably goes without saying that tissue clamps or towel forceps should not be applied to the pillow, as this will cause a leak and prevent a vacuum forming, hence the bag will not fix in a set position.)
These instruments need gentle cleaning and care. Ultrasonic instrument cleaning machines are useful provided instruments are placed in small strips of rubber matting and are not allowed to jostle against one another (as this will damage them). If instruments are placed on large rubber finger mats this may impede ultrasonic cleaning. Instruments of different metal types should not be placed together, to avoid electroplating between instruments.
Viscoelastic agents
Surgeries that may involve intraocular work, whether intentional or not (eg, corneal foreign body that penetrates the anterior chamber or descemetocoele that ruptures intra-operatively), may require viscoelastic substances to reform the anterior chamber and separate tissues (eg, synechiae). There are a number of viscoelastic agents available commercially that vary in their rheological properties (cohesion, dispersion, elasticity, coatability and pseudoplasticity).
Barraquer eyelid speculum. Courtesy of AcriVet
Colibri forceps. Courtesy of AcriVet

Fine rat-tooth forceps. Courtesy of AcriVet
Westcott tenotomy scissors. Courtesy of AcriVet

Sharpoint restricted depth knife (300 μm) — the button on the blade prevents the knife incising deeper than desired

Sharpoint I angled bevel-up crescent I knife I (performing la superficial I keratectomy I in a horse)

Microneedle holders suitable for use with 8/0 vicryl or finer suture material

Preparing for surgery
For corneal procedures eyelash clipping is sufficient. Clipping of periocular hair may increase the risk of patient irritation and rubbing postoperatively. Fine blunt/blunt curved scissors should be coated with lubricant and the lashes trimmed close to their base. The lubricant helps to catch hairs and avoid them falling onto the ocular surface. Lubricant can also be used to coat the eye prior to clipping; on subsequent flushing, any stray hairs will be removed with it.
Povidone-iodine is an excellent ocular disinfectant with both antibacterial and antifungal activity. It is important that the solution formulation is used as the scrub, as tincture formulations are irritant and damaging to the ocular surface. Povidone-iodine is not well tolerated by the corneal endothelium and therefore it should not be used in the preparation of a ruptured globe; sterile saline only should be used to prepare such an eye for surgery.
A paradoxical effect is seen on dilution of povidone-iodine, with more dilute solutions exhibiting a greater antibacterial action compared with stock solution. Dilutions of 1 in 10 to 1 in 50 for ocular surgery are reported in the literature based on tissue tolerance and bacterial counts. The author uses a dilution of 1 in 10 for eyelids and 1 in 50 for the ocular surface.
Corneal foreign body
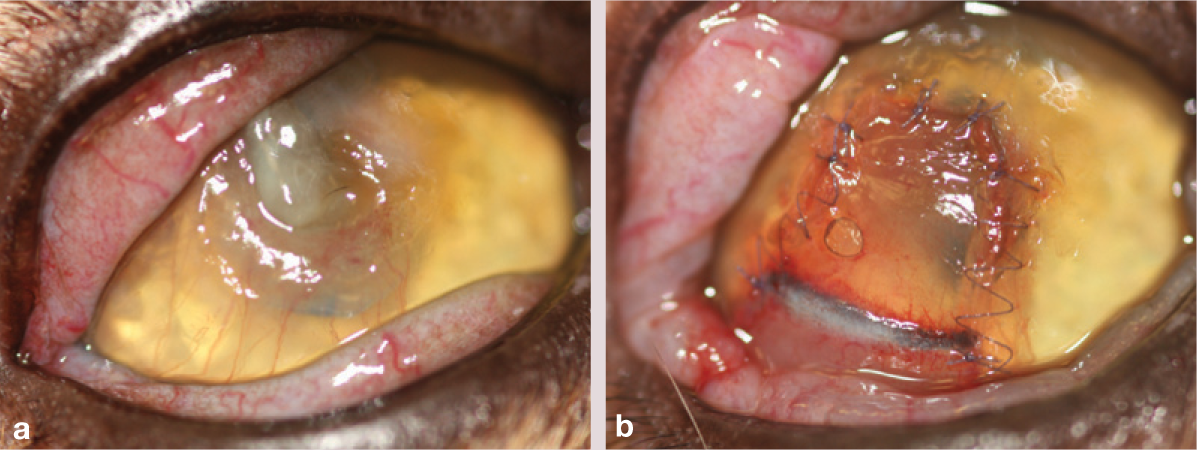
Corneal foreign bodies are not encountered as frequently in cats as in dogs, but the treatment approach is similar — removal should be undertaken under general anaesthesia and the surgeon should be prepared for intraocular surgery (Figs 2 and 3). The foreign body should ideally be impaled perpendicularly to the route of entry (eg, with a fine gauge needle or foreign body spud) and withdrawn carefully along its original track. (Grasping the foreign body in the same plane is more likely to push it further posteriorly, potentially into the anterior chamber.)
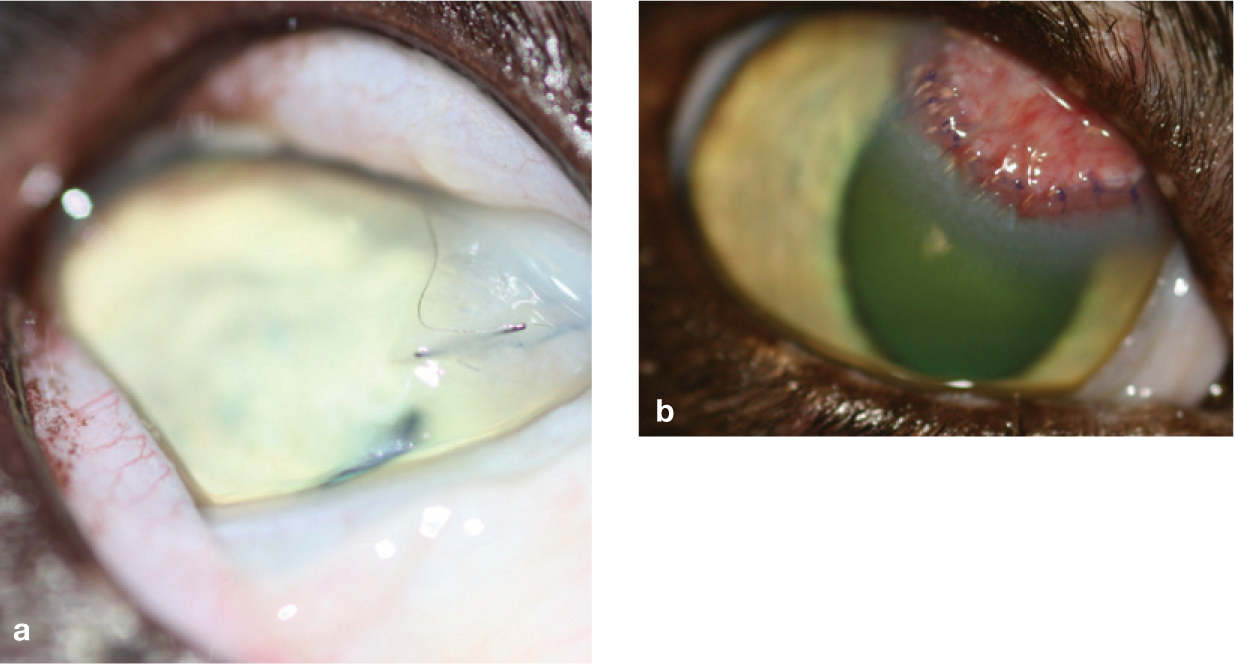
(a) Deep stromal corneal foreign bodies (cat hairs) following a cat fight. Note the marked chemosis and miosis, which were accompanied by a localised stromal cellular infiltrate. (b) Appearance 2 weeks after foreign body removal and placement of a conjunctival advancement graft

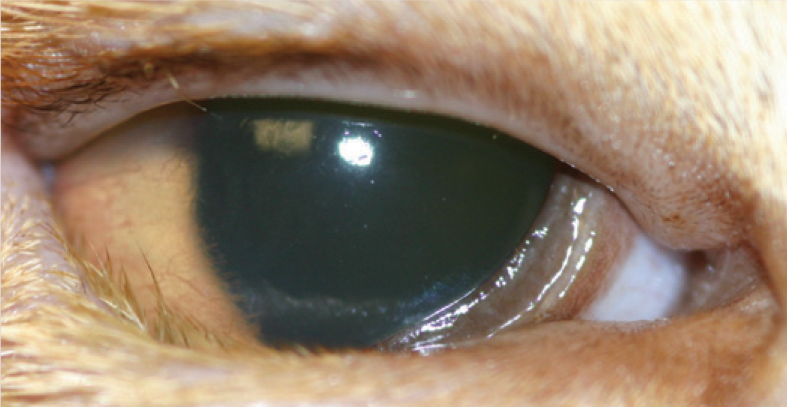
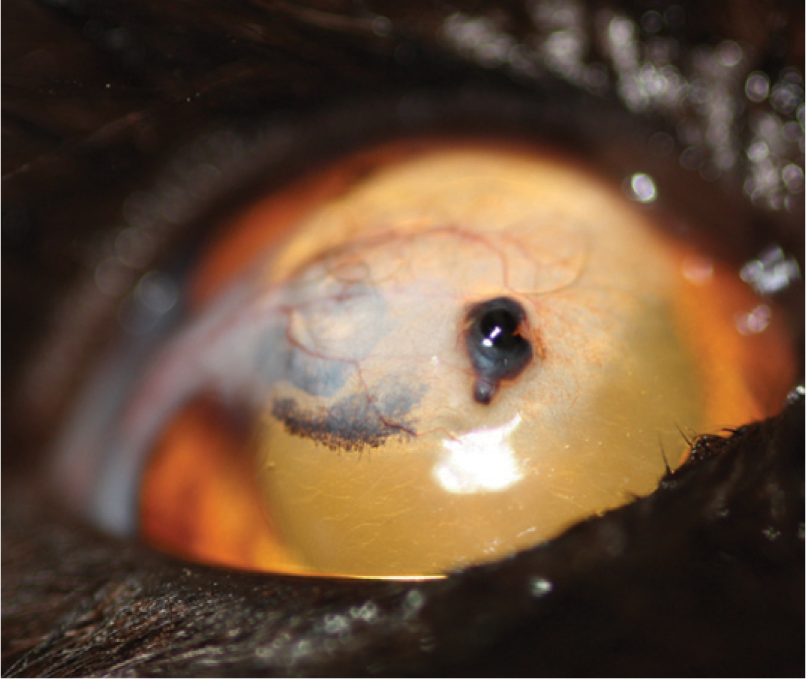
Mid-stromal corneal foreign body (thorn) in a domestic shorthair cat
Where this is not possible, the foreign body may have to be approached via an incision alongside the track of entry, with the creation of a trough through which it can be removed. These cases are best referred, where possible, so that an operating microscope can be used for the surgery.
Entropion, ectopic cilia and distichiasis
Entropion can be a cause of corneal ulceration in cats. Conversely, chronic ulceration may cause a spastic entropion that, with fibrosis, becomes irreducible even following application of topical local anaesthetic (Fig 4). Entropion may also be encountered in older cats where loss of the orbital fat pad results in enophthalmia (sinking of the globe), less support to the eyelids and secondary entropion. 2 Irrespective of the cause, surgical correction of the entropion is required. In most cases a simple Hotz-Celsus procedure is the best surgical remedy (Fig 5).
Entropion in a 3-year-old Abyssinian following chronic corneal ulceration and fibrosis of a resultant spastic entropion

(a) Entropion in a 12-year-old cat due to weight loss and enophthalmos (sinking of the eye in its socket due to loss of retrobulbar tissue, particularly adipose tissue). (b) Appearance following Hotz-Celsus correction of lower eyelid entropion
In the case of ectopic cilia or distichiasis (Figs 6 and 7), both of which are uncommon in cats, excision of the offending hair follicle(s) is curative. Placement of a therapeutic soft contact lens, while any accompanying ulcer heals, provides pain relief. Multiple distichia can be treated by excision if few in number, or electrolysis or cryotherapy if more numerous.

Distichiasis in a domestic shorthair kitten

Distichia on the medial lower eyelid, chronic corneal ulceration and stromal keratitis
Eyelid agenesis
Eyelid agenesis is encountered sporadically in cats.3,4 As well as occurring in domestic cats (Fig 8), particularly in the Birman and Burmese breeds, this congenital abnormality has also been seen in Snow Leopards 5 and a Texas cougar. 6

One-year-old domestic shorthair cat with unilateral (left) eyelid agenesis. The eye was microphthalmic with a micropalpebral fissure
Surgical correction of eyelid agenesis can be involved and these cases are best referred. Some authors have described the successful use of cryotherapy to treat any associated trichiasis (hair contact with the cornea), although the exposure of the cornea often requires additional treatment (see later). 6
Several blepharoplastic surgeries have been described to reconstruct the upper eyelid defect in agenesis including the Roberts and Bistner technique, 7 a modification of the Mustardé technique, 8 a two-stage cross lid flap, 9 and a two-stage technique using sub-dermal collagen and the Stades procedure. 10
Corneal lacerations
Corneal lacerations can be directly sutured provided there is no corneal deficit (which would cause unacceptable astigmatism with direct suturing) and the cornea is sufficiently healthy to hold the sutures (Fig 9). Sutured lacerations can be covered with a conjunctival graft (simple advancement if adjacent to the limbus, or pedicle if more central [see page 402]) if there is doubt over the closure or adequacy of infection control (bringing blood vessels directly to the site will speed clearance).

Cat scratch laceration of the lateral cornea, repaired with direct corneal sutures
Suturing is best performed using an operating microscope. Where referral is not possible (to an institution with this equipment) the use of surgical magnification loupes is essential — as, indeed, for any corneal surgery.
Stromal abscess
Stromal abscessation can develop following stromal ulceration, when overlying epithelial healing occurs, sequestering bacterial or fungal infection within the stroma. 11 Treatment of the microorganism is hindered by the epithelial barrier to drug penetration, 12 necessitating debridement of surface epithelium to assist penetration of topical medications.11,13 Debridement may need to be repeated; alternatively, a conjunctival graft, and therefore vascular supply, can be sutured over the abscess after epithelial debridement or surgical excision of the abscess. 11
Conjunctival pedicle graft
Conjunctival pedicle graft in a cat following superficial keratectomy for treatment of a sequestrum

A conjunctival pedicle graft provides both tectonic (albeit minimal) and vascular support to a corneal ulcer. The tectonic support of a conjunctival graft is not as great as that provided by cornea (eg, as used in corneoconjunctival transposition, lamellar keratoplasty, and penetrating keratoplasty techniques).
In most superficial nonprogressive ulcers a pedicle graft is not required, and will only contribute to scarring. However, for malacic, infected or very deep stromal ulcers this surgical treatment is often indicated.
When resection of a sequestrum is incomplete (ie, where deep or full thickness corneal resection would otherwise leave a weakened cornea), placement of a conjunctival pedicle graft may, according to some authors, prevent deterioration of the remaining sequestrum. 18
The pedicle can be sectioned after 6–8 weeks if a vascular supply is no longer needed (eg, healing is complete, and there is no sequestrum), to reduce scarring, although many grafts will significantly thin with time in cats even without pedicle sectioning.
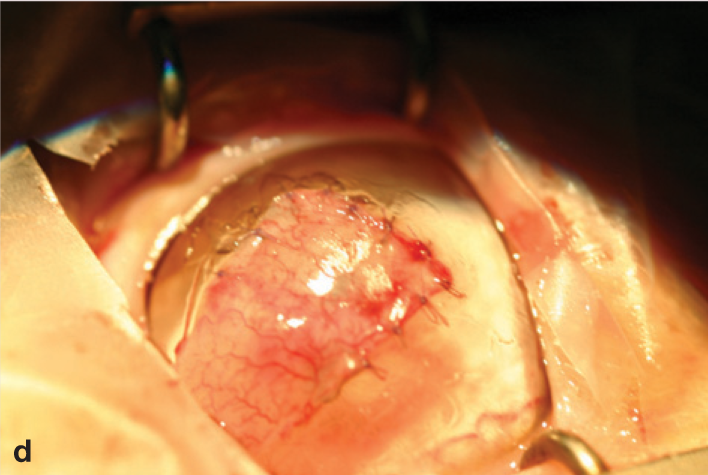
(a) A sequestrum has been resected by superficial keratectomy but faint corneal pigmentation remains and therefore a pedicle graft is planned. The conjunctiva is incised perpendicularly to the limbus and undermined

(b) The conjunctiva is incised along the limbus. A second incision is then made parallel to this first incision at an appropriate width to cover the corneal defect (minimum 1–2 mm wider than the defect)

(c) The pedicle is trimmed to remove excess Tenon's capsule, which may otherwise cause contracture of the graft and retraction from the corneal sutures

(d) The conjunctival graft is sutured into the defect, usually starting with cardinal sutures at each of the corners, followed by intervening sutures
(e) Limbal sutures may be added to improve the stability of the graft on the cornea and resist contraction of the pedicle

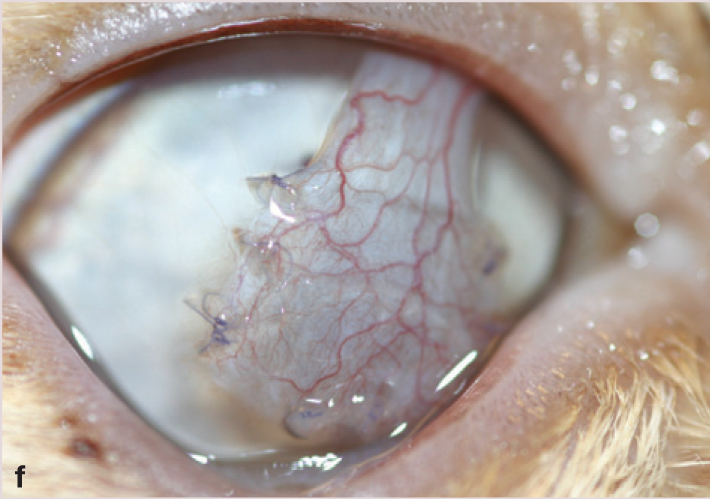
(f) Appearance of the pedicle graft 21 days postoperatively
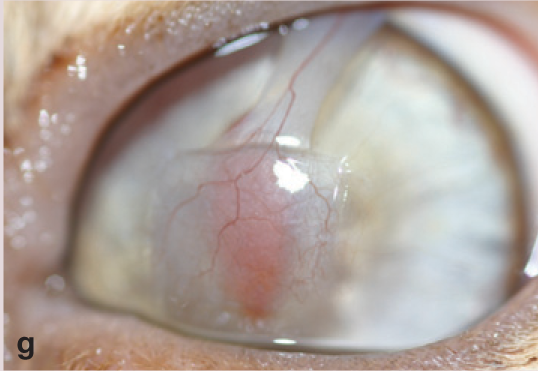
(g) A similar graft 6 months postoperatively, showing thinning without pedicle sectioning
Complete excision of the abscess can be undertaken by penetrating keratoplasty (corneal transplant), lamellar keratoplasty supported by a conjunctival graft, or corneo scleral/conjunctival transposition (see page 404). 14
Sequestra
Once a sequestrum forms within an ulcer bed, healing is unlikely with medical treatment alone. 15 Treatment requires surgical excision of the sequestrum (Fig 10). The depth of the corneal necrosis is very difficult to assess pre-operatively without the benefit of advanced imaging modalities (ultra-high resolution ultrasound biomicroscopy). 16

Postoperative appearance following superficial keratectomy for sequestrum removal, in this case without conjunctival graft placement
Conjunctival island graft
Chronic sequestrum surrounded by marked granulation tissue. Treatment comprised superficial keratectomy and conjunctival island graft placement

Where extensive corneal vascularisation is already established, and minimal tectonic support alone is required, a conjunctival island graft can be placed. The island will often re-vascularise from corneal blood vessels.
For descemetocoeles, extra support can be provided below the island using autologous Tenon's capsule, or porcine small intestinal submucosa (Vet BioSISt; Smiths Medical, WI, USA). 20
Vet BioSISt can also be used without a conjunctival covering. The product does not have high tensile strength (tectonic support) alone but can be used in multiple layers. 21 The veterinary use of porcine small intestinal submucosa in ocular surgery has been described in four studies.20,22–24 Three of these involved cats, the largest series reporting a success rate of 80% (ie, no further surgery required and vision maintained). 20
(a) Descemetocoele with extensive corneal vascularisation and granulation tissue

(b) Two layers of Vet BioSISt have been sutured below a conjunctival island graft taken from the ventral conjunctival fornix

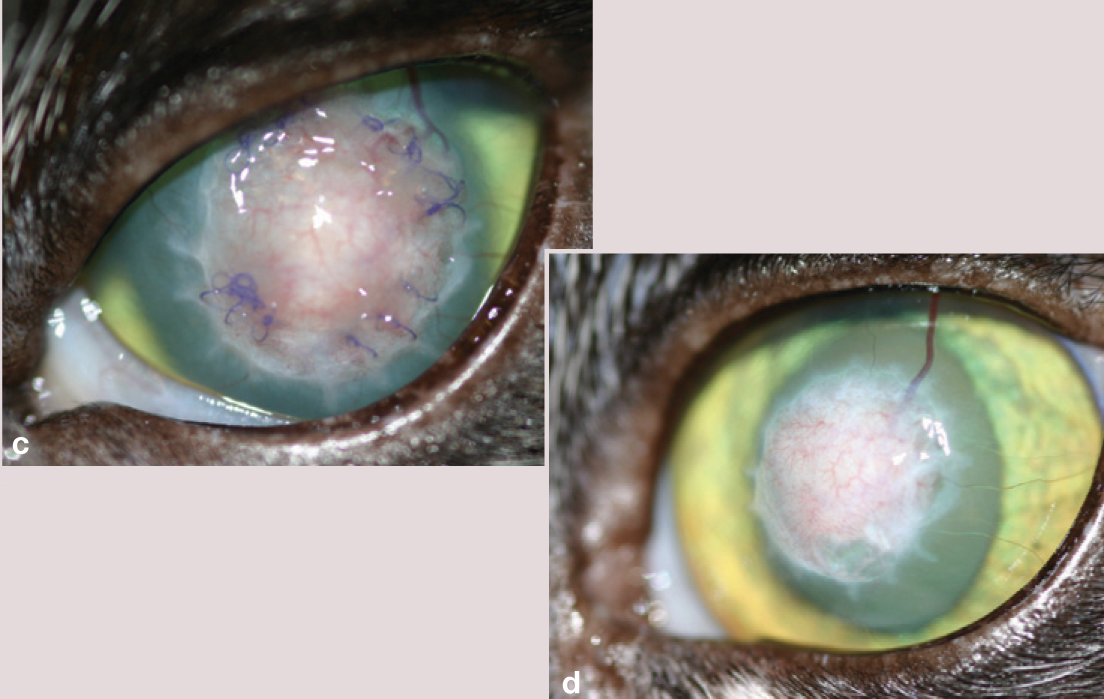
Appearance at 22 days (c) and 9 weeks (d) postoperatively
If all of the sequestrum can be successfully excised, placement of a therapeutic soft contact lens may be analgesic in the postoperative period. If the sequestrum cannot be completely excised, or requires very deep (>0.3 mm) dissection, a conjunctival pedicle graft may be required to cover the defect (see page 402).17,18 Surgical treatment of a sequestrum using a corneoscleral or corneoconjunctival transposition (see right) may result in less scarring. 19
Recurrence of sequestrum following surgical excision has been reported (Fig 11), although this is more common if the sequestrum pigment cannot be completely removed. 17 Reduced rates of recurrence following conjunctival graft placement have been described, particularly when the pedicle (and therefore vascular supply) is not sectioned. 18 However, this finding was not confirmed by the later retrospective study, in which the decision to place a conjunctival pedicle graft was at the surgeon's discretion, with deep and extensive sequestra being more likely to receive a graft. 17 Those cases where the conjunctival pedicle was subsequently sectioned were more likely suffer complications, including sequestrum recurrence. 17
Sequestrum recurrence at the site of a previous keratectomy and conjunctival pedicle graft, performed 18 months earlier. This lesion was treated by superficial keratectomy alone
A study of 17 cases of feline sequestrum treated by lamellar keratectomy and corneo-conjunctival transposition (see right) reported no recurrence. 19
Exposure keratopathy
Exposure of the cornea may occur due to lagophthalmos (inability to complete a blink reflex). The palpebral reflex may be absent due to a neurological deficit (trigeminal or facial nerve paralysis), or there may be mechanical restriction of the eyelids (eg, an erosive or restrictive eyelid lesion such as squamous cell carcinoma or idiopathic orbital sclerosing pseudotumour).
Treatment of the lesion or neoplasm (excision, brachytherapy, plesiotherapy, photo-dynamic therapy), and supportive care of the cornea (false tear preparation and/or contact lens), with antibacterial therapy if appropriate, is indicated. The prognosis in cases of idiopathic orbital sclerosing pseudotumour is poor; enucleation is often the only treatment option.
Cyanoacrylate tissue glue
Butyl 2-cyanoacrylate tissue glue application has been reported to be successful in 10 cases of feline ulcerative keratitis. In two cases, glue was applied after partial dehiscence of a conjunctival graft, in six it was used on stromal ulcers (bacterial, keratomalacic and non-perforating laceration) and in another two it was used after superficial keratectomy for sequestrum removal. 25 Tissue glue should not be used on a descemetocoele or full-thickness perforation because of the risk of toxic effects on intraocular structures with inadvertent intraocular penetration. On polymerisation of liquid tissue glue, heat is released that may cause rupture of a descemetocoele. There are conflicting reports on the antibacterial versus bacterial promoting effects of cyanoacrylate glues.26,27
Corneoconjunctival transposition
Corneoconjunctival transposition is a useful technique where greater tectonic support is required, infection is controlled and reduced scarring is desired. 18
Cornea adjacent to the ulcer bed is sectioned in a part thickness flap and extended into the adjacent conjunctiva. This raised graft is I then drawn forward over the defect and sutured in place.
(a) Deep malacic stromal ulcer with sequestrum in the central cornea of a one-eyed domestic shorthair cat. (b) Appearance following corneoconjunctival transposition; linear pigmented tissue represents the transposed limbus
(a) Deep stromal ulcer, with surrounding (180°) vascularisation, which was treated by corneoconjunctival transposition. (b) Appearance of a corneoconjunctival transposition, 9 months postoperatively

Temporary tarsorrhaphy placement is a useful procedure to limit exposure and is essential in cats with trigeminal paralysis affecting corneal sensation (neurotrophic keratitis). Some cases of facial nerve paralysis (neuro-paralytic keratitis) can benefit from temporary tarsorrhaphy placement, particularly where tear production is affected.
KEY POINTS
Surgical intervention should be considered when two-thirds or more of the corneal depth has been lost, an ulcer is rapidly progressing (eg, keratomalacia), the ulcer is failing to respond to medical treatment as expected, a contributing factor such as entropion has been identified, or healing is compromised by poor tear production or corneal exposure.
Corneal foreign bodies, descemetocoeles and corneal perforations represent surgical emergencies.
Corneal surgery should be undertaken by those who are equipped for and experienced in intraocular surgery, as some cases may require this intraoperatively, once the surgeon is past the point of no return.
When choosing the appropriate procedure, consider whether physical support and/or vascularisation is required.