
Abstract
The diagnosis and surgical treatment of spinal epidural empyema (SEE) in a 2-year-old neutered male domestic shorthaired cat is described. SEE was diagnosed by computed tomographic myelography (CT myelography) and surgical exploration. The lesion was missed on both non-enhanced CT and conventional myelography. SEE should be considered in the differential diagnosis of progressive myelopathy in cats, and CT myelography should be undertaken when magnetic resonance imaging (MRI) cannot be performed.
A 2-year-old neutered male domestic shorthaired cat was referred to the Teaching Hospital of the Kurashiki University of Science and The Arts. One month before admission to the hospital, the cat had been examined by a veterinarian for progressive pelvic limb paralysis and the presence of severe tenderness in the lumbar region. The spinal radiographs obtained at that time were normal, and the cat was administered prednisolone (predonine; Shionogi; 1 mg/kg q24 h) for 10 days. With no improvement in the cat's condition, it was referred to our hospital for further examination.
Physical examination revealed severe muscular atrophy in the pelvic limbs, and neurological examination revealed proprioceptive deficits in the pelvic limbs. The segmental nerve reflexes in the pelvic limbs were normal or increased, with the left side more severely affected than the right, and there was loss of deep pain perception. On the basis of these findings, a spinal cord lesion was assumed to be present between T3 and L3.
Complete blood count (CBC) revealed a mild neutrophilia (268×102/μl; reference range, 25–115×102/μl); serum biochemical values were within the reference ranges.
Non-enhanced computed tomography (CT; Asteion 4, Toshiba Medical Systems Corporation) of the thoracic and lumbar regions of the vertebral column was performed on the same day under sedation with medetomidine hydrochloride (Domitor; Zenoaq; 0.05 mg/kg) and midazolam (Dormicum; Astellas; 0.2 mg/kg), and general anaesthesia was induced with propofol (Rapinovet; Schering-Plough; 8 mg/kg, IV) and maintained with inhaled isoflurane (Forane; Abbott Japan) and oxygen. No abnormalities were detected on non-enhanced CT. On conventional myelography (Omnipaque 240; iohexol; 0.3 ml/kg), a line of contrast material was not detected along the dorsal and ventral aspect of the spinal cord at L2–L4. The obtained myelogram did not, however, help in the characterisation of the lesion (Fig. 1). Therefore, CT myelography was performed, which revealed a questionable soft tissue density in the left dorsal aspect of the vertebral canal at L2–L4 (Fig. 2). No significant abnormalities were observed in the adjacent bone, soft tissues or in the lumbar cerebrospinal fluid. The clinical findings and neurological signs were ascribed to the extradural lesion. In the differential diagnosis of the lesion, the following conditions were considered: haematoma, granuloma, empyema and neoplasm. Surgical exploration and decompression were performed a few days later.

Lumbar myelography: (a) lateral image, (b) ventrodorsal image. The myelogram shows a line of contrast material was not detected along the spinal cord at L2–L4. This myelogram does not, however, further characterise the lesion.
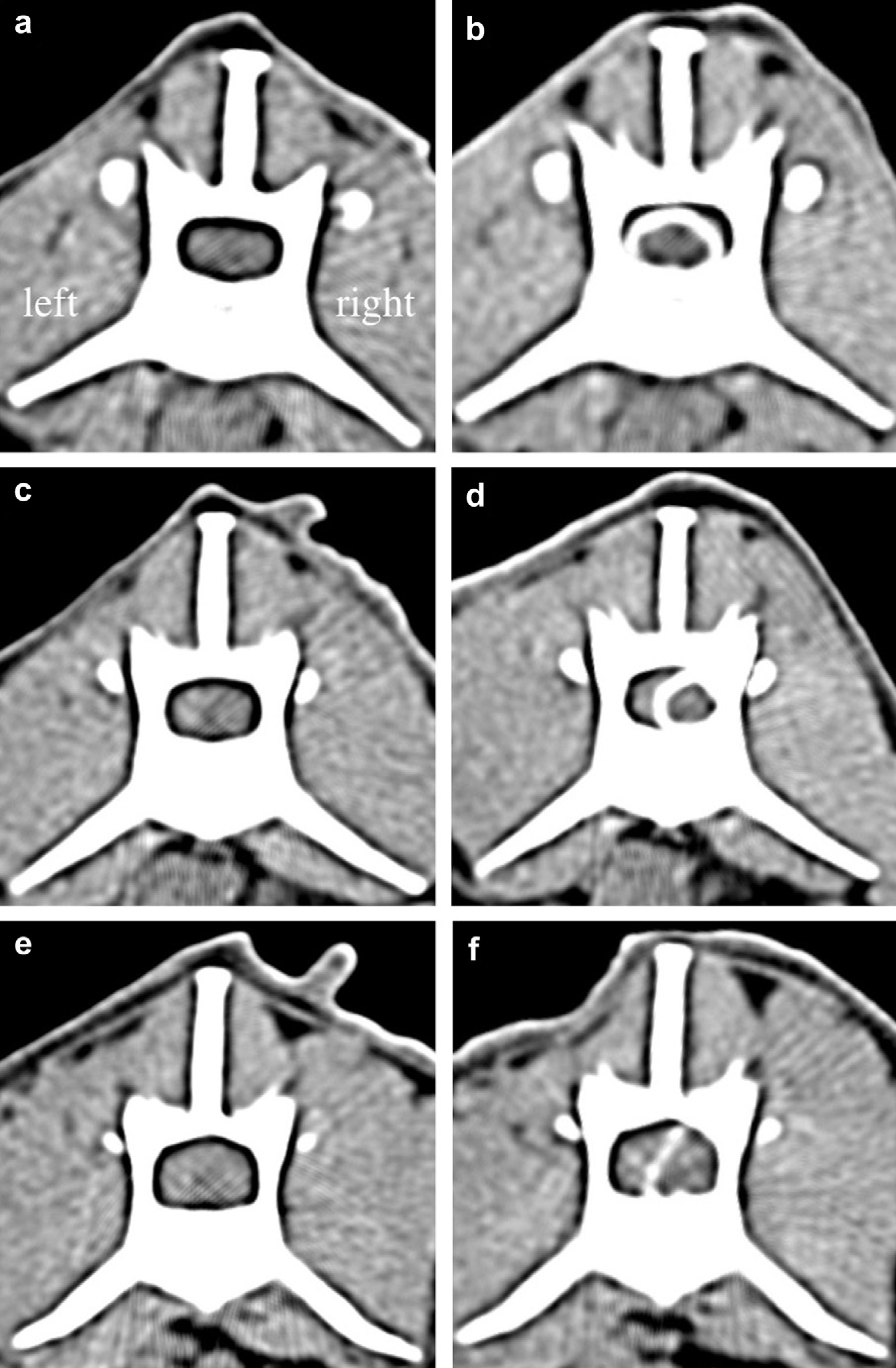
CT (left images) and CT myelography (right images) of the lumbar vertebrae at the levels L1 (a, b), L3 (c, d), and L4 (e, f). Extradural compression is not observed at L1 (a, b). At L3 and L4, there is a distinct soft tissue mass in the extradural space, and the spinal cord is severely compressed by the mass (c–f).
The vertebral column was accessed at L3–L4 via a dorsal approach. When preparing the surgical field, no cutaneous abnormalities were detected. There were no significant abnormalities in the subcutaneous tissue and paravertebral muscles. A standard dorsal laminectomy was performed, and a large amount of friable or fibrous tissue was found in the extradural space at L3–L4. Some of these tissues were adherent to the dorsal surface of the spinal cord, and the rest extended laterally to the left side of the extradural space and compressed the spinal cord. Macroscopic examination of the spinal cord revealed no abnormalities. The tissues were carefully removed, and the area of the lesion was flushed with a large amount of sterile saline solution and closed using standard methods.
Cytological and histopathological examination, aerobic bacterial culture, and sensitivity tests were performed using the epidural tissue samples; however, anaerobic bacterial culture could not be performed. The cytological examination revealed a large number of bacteria, neutrophils, and macrophages; some neutrophils and macrophages contained phagocytosed bacteria. The sample tissue contained many neutrophils, foamy macrophages, and granulomatous tissue with abundant neovascularisation. Histopathological analysis revealed pyogranulomatous inflammation. No aetiological agents were isolated in the aerobic bacterial culture.
The patient received intravenous ampicillin (Viccillin; Meijiseika; 30 mg/kg q12 h) for 3 days after surgery and oral ampicillin for 1 week until the results of bacterial culture were obtained. Oral clindamycin (Antirobe; Pfizer; 5 mg/kg q12 h) was administered for 3 weeks to eliminate anaerobic bacteria, if present.
Gradual improvement in the voluntary motor activity of the pelvic limbs was seen from 1 week after the operation. Three weeks after surgery, the cat could independently support its weight on the right pelvic limb, but not on the left. After 3 months, the cat had recovered enough to walk, although some ambulatory difficulties remained in the left leg.
Spinal epidural empyema (SEE) is characterised by the accumulation of purulent material in the epidural space of the vertebral canal. Although there are several reports on epidural abscesses in humans and epidural empyema in dogs, 1–3 there has been only one report of this condition in cats. 4 While SEE in dogs is caused by foreign bodies (grass awn and wooden sticks), bite wounds, haematogenous or lymphatic spread, or unknown causes, the one reported case in the cat was caused by a grass awn. 4 In humans, epidural abscesses are usually caused by local extension of osteomyelitis or discitis. 5 Fever, intense pain, weakness, and spinal cord dysfunction are characteristic findings in dogs and humans with SEE; however, these signs are not seen in all patients with SEE. 1,3,5–7 In the previously reported case, the cat had presented with signs of intense neck pain, fever, progressive tetraplegia, and was found to have inflammatory tissue with a grass awn fragment in the paravertebral region. 4 In this case, the patient did not show any abnormalities in the skin and paraveretebral region, and the cause of SEE is unknown. Anaerobic bacterial infection in bite wounds or trauma due to sharp objects was suspected in this case because no bacteria were found in the aerobic bacterial culture in spite of the presence of bacteria in purulent secretions. However, the cause of SEE could not be revealed because anaerobic bacterial culture could not be performed. When infection is suspected, anaerobic bacterial culture should always be performed with aerobic culture.
Conventional radiography is not reliable for diagnosing SEE, because radiologically detectable changes in the vertebrae appear several weeks after the disease onset. 5–8 Non-enhanced CT and magnetic resonance imaging (MRI) are commonly used for diagnosing SEE 1,4,5,9,10 ; however, in this case, the lesion was not detected on non-enhanced CT because in the images obtained, the spinal cord was indistinguishable from the tissue in the extradural space. Conventional myelography is an excellent technique for detecting extradural compressive lesions. 5,8 Both conventional myelography and non-enhanced CT are useful for locating the site of disc herniation 11,12 ; however, the former provided no information on the detail characterisation of the lesion in this case. In humans, CT myelography is superior to non-enhanced CT for the detection of SEE in terms of diagnostic accuracy and sensitivity (92% in the former). 5 In dogs, CT myelography was reported to be effective in detecting SEE. 10 In our case, the lesion was missed on non-enhanced CT, but detected on CT myelography. Although CT myelography could not reveal the causes, such as abscess, of an epidural lesion, it is at least effective in the detection of the lesion.
In humans, the prognosis of SEE is considered guarded; however, between 1950 and 1990, the mortality has reduced from 34% to 16%. 5 In dogs and cats, patient recovery is satisfactory after decompressive surgery with antibiotic therapy. 1,3,4,7,13,14 In this case, the neurological prognosis was good despite the relatively long clinical course.
SEE is a rare disease, especially in cats. The clinical signs can be ameliorated by decompressive surgery, drainage of the abscess and antibiotic therapy. Therefore, SEE should be included in the differential diagnosis of progressive myelopathy in cats. Furthermore, the lesion may not be detected on non-enhanced CT. Therefore, CT myelography should be performed when MRI examination cannot be performed.
Footnotes
Acknowledgments
The authors thank Messrs T Tokuoka and T Tomita, Tomita Animal Hospital for providing this case. This study had no source of funding.