
Abstract
The current report describes the diagnosis of a nasopharyngeal granuloma due to a fungal infection by Trichosporon loubieri. This is the first report of successful treatment of nasal granuloma formation caused by Trichosporon species infection in a cat.
In cats Cryptococcus species infection is a more commonly recognised cause of mycotic rhinosinusitis than disease caused by filamentous fungi, although nasal and periorbital infections with Aspergillus or Penicillium species have been reported. 1–7 Other fungal infections of the nasal cavity and sinuses have also been described in cats. 8–11 Nasal granuloma formation caused by Trichosporon species infection has been reported previously in a cat, however, treatment was not successful. 12
A 10-year-old female neutered Siamese was referred to Murdoch University Veterinary Hospital (MUVH) with a 6-month history of stertor, sneezing and bilateral nasal discharge. Initially the nasal discharge was serosanguinous, but had progressed to become purulent. Prior investigation by the referring veterinary surgeon had identified a nasopharyngeal mass. Histopathological examination of this mass showed granulomatous inflammation and fungal elements considered consistent with Cryptococcus species. However, a latex cryptococcal antigen agglutination test (LCAT) was negative. Mild clinical improvement had been observed after treatment with itraconazole (5 mg/kg sid per os (PO) for 7 days, then bid). However, this dosage was reduced (5 mg/kg sid PO) after 4 weeks and then discontinued after 8 weeks due to a moderate elevation in serum alanine aminotransferase (ALT), which coincided with worsening of respiratory signs.
On referral examination, 11 weeks after initiation of itraconazole therapy, the cat was alert with a body condition score of 4/9. Thoracic and cardiovascular examinations were unremarkable. Peripheral lymph nodes were normal in size and consistency and there was no evidence of ocular discharge, facial deformity or pain on palpation of the nose. While there was no airflow through the nares, no open mouth breathing was observed. Although the previous histopathology was not available for review, the report identified some morphological changes that were felt to be inconsistent with a diagnosis of Cryptococcus species infection. Given this assessment and the recent deterioration in clinical signs complete re-evaluation was recommended.
Serum biochemical analysis identified a mildly increased creatinine kinase (180 U/l; reference range (RR) 50–100 U/l), moderately increased ALT and aspartate aminotransferase (AST) activities (397 U/l; RR 0–83 U/l and 144 U/l; RR 26–43 U/l, respectively), a mild increase in total bilirubin (9 μmol/l; RR 0–8 μmol/l) and a mild increase in urea (12.1 mmol/l; RR 7.0–10.7 mmol/l).
Computed tomography was performed with a dual-slice helical scanner (Somatom Emotion (Duo); Siemens, Munich, Germany). Transverse contiguous slices (3 mm) of the nasal cavity were obtained. Pre- and post-contrast (600 mg/kg IV of an iodine-based contrast material; Iohexol) studies were performed. Examination of bone and soft tissue windows identified a large heterogenous, enhancing soft tissue mass obliterating the nasopharynx ventral to the sphenoid sinus. There was no evidence of lysis of the surrounding bone structures. The right frontal sinus contained a non-enhancing fluid density, surrounded by a thin rim of mucosal enhancement. The left frontal sinus was normal. Mucosal thickening was evident within the right dorsolateral nasal cavity.
On endoscopic examination of the nasopharynx there was a large, pale pink mass completely obstructing the choanae and this could be palpated through the soft palate. Multiple biopsies were collected from the nasal cavity and nasopharynx in addition to fine needle aspirates of the mass for histopathology, tissue culture and immediate impression smear cytology.
Impression smears from the mass were moderately cellular. A lightly proteinaceous background contained many erythrocytes, low numbers of platelets, nuclear debris and bare nuclei. Round to oval, encapsulated fungal organisms were observed amongst moderate numbers of well-preserved neutrophils and macrophages. Organisms were occasionally found within macrophages (Fig. 1). Small numbers of pseudohyphal forms and single thin and broad-based budding yeast forms were identified (Fig. 2a and b). Fungal hyphae were not detected. The fungal organisms were 2–8 μm long, 1–4 μm wide, with a thin capsule measuring 0.5–1 μm and contained granular, deep purple staining cytoplasm. These cytological features were initially considered likely to be due to Cryptococcus species, Candida species or another type of yeast.
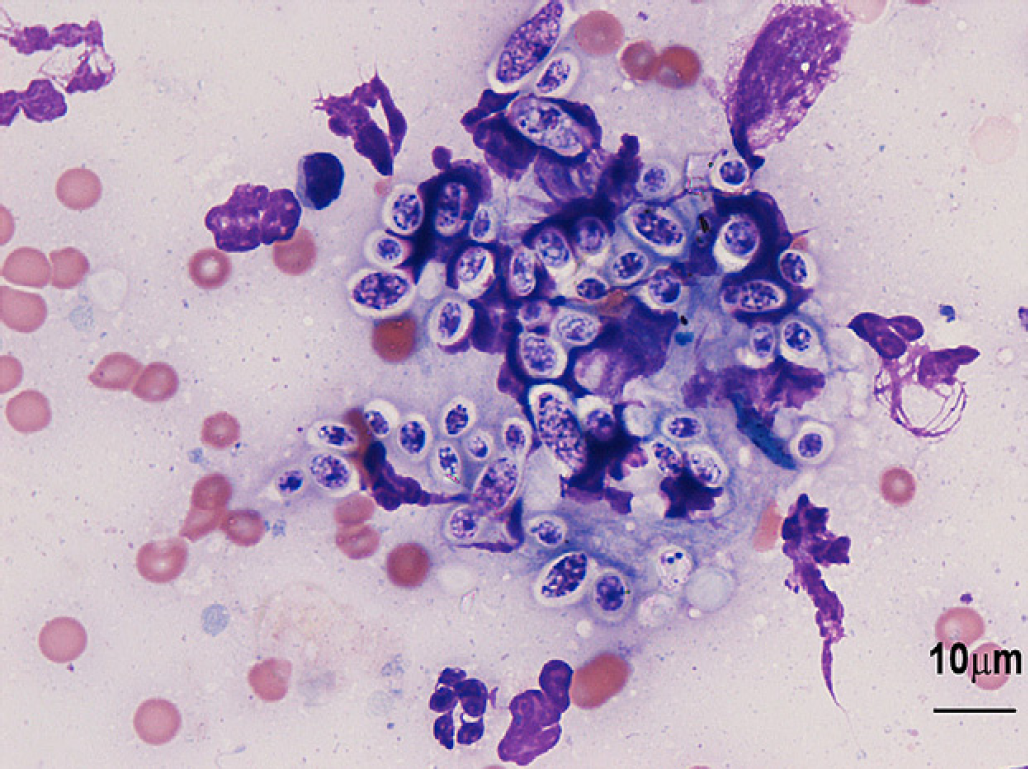
Impression smear of the nasal cavity mass revealing numerous yeast-like organisms with a thin clear staining capsule. Modified Wright-Giemsa, scale bar=10 μm.

Trichosporon loubieri. Single bud forms (a) and psuedomycelial forms (b) are shown. Modified Wright-Giemsa, scale bar=10 μm.
Histopathological sections of the mass were characterised by a mixed inflammatory infiltrate of predominantly activated macrophages and neutrophils with lesser numbers of plasma cells and lymphocytes contained within a fine fibrovascular stroma (Fig. 3a). Widespread throughout all sections were round to oval yeast-like fungi with a thin wall and a thin clear mucoid halo often contained within macrophages and causing expansion of the cytoplasm. These organisms were 2–8 μm in diameter with finely granular cytoplasm. Irregular shapes and pseudohyphae were also identified. The organisms stained positive with periodic acid-Schiff indicating the presence of polysaccharides in fungal cell walls (Fig. 3b). The histological assessment concluded fungal granulomas with intralesional yeast-like organisms the histomorphology of which was not felt typical of Cryptococcus species. Differential diagnoses of Histoplasma species and Candida species were considered and fungal culture was recommended.

Histologic sections of the nasal cavity mass. Mixed inflammatory infiltrate dominated by macrophages and neutrophils are seen with abundant intralesional Trichosporon loubieri organisms (a). Many macrophages are expanded by clusters and colonies of the organism. T loubieri is periodic acid-Schiff-positive (b). (a) H&E, scale bar=20 μm, (b) scale bar 20 μm.
Biopsies submitted for fungal culture produced a heavy growth of yeast with colony morphology atypical for Cryptococcus species and identified as a Trichosporon species. Further classification via DNA sequence analysis of the Internal transcribed spacer (ITS) region with universal primers was performed by using the Applied Biosystems Prism 3100 Avant Genetic Analyser (Foster City, CA, USA) with an Applied Biosystems BigDye Terminator v3.1 Cycle Sequencing kit. This identified the isolate as having 99% homology of the ITS region with T loubieri. Minimal inhibitory concentration (MIC) susceptibility testing by micro-broth dilution standardised for Candida species (Sensititre, Trek Diagnostic Systems; Cleveland, Ohio) demonstrated susceptibility to a number of antifungal agents including itraconazole, fluconazole, posaconazole and voriconazole (Table 1).
MIC testing results.

Subsequent urinalysis via cystocentesis detected a bacturia which was considered more likely to be due to contamination as urinalysis failed to identify pyuria or haematuria, urine was moderately concentrated (Urine specific gravity (USG) 1.031) and there were no clinical signs of lower urinary tract disease. Fungal culture was negative, however, bacterial culture was not performed. Feline immunodeficiency virus (FIV) (Rapid Immune Migration (RIM) antibody) and feline leukaemia virus (FeLV) (RIM antigen p27) testing was negative. Thoracic radiographs showed a mild focal interstitial lung pattern in the right middle lung lobe which was felt to be most likely due to atelectasis. Debulking of the lesion via digital palpation and nasal flushing as described previously 13,14 was recommended and considered an important component of treatment. While the procedure was attempted, anaesthetic complications necessitated discontinuation and no further investigations or procedures were permitted.
Due to the previously observed hepatotoxicity with itraconazole therapy and the results of sensitivity testing the cat was prescribed fluconazole (10 mg/kg q12 h; compounded) for a period of 6 months. Follow-up via telephone communication since discontinuation of therapy has indicated continued clinical remission, but further investigations were not undertaken and the cat remained asymptomatic 12 months after initial diagnosis.
Trichosporon species are ubiquitous saphrophytic yeast-like fungi of the family Cryptococcaceae and are generally not considered primary pathogens. 15,16 A range of conditions caused by Trichosporon species have been reported in immunocompetent humans including summer-type hypersensitivity, allergic pneumonia and white piedra which is characterised by benign superficial nodular lesions involving the hair shafts. Life-threatening disseminated infections have also been reported typically in immunocompromised and postoperative human patients. 15–17 Trichosporon species are the second most common disseminated infection behind Candida species in human patients with haematological malignancies and disseminated infection is frequently associated with mortality despite aggressive therapy. 15 As Trichosporon species are not considered pathogenic, opportunistic infection is probable in most cases.
In animals, Trichosporon species have been associated with outbreaks of mastitis in dairy herds and abortions in both cattle and horses. 16 Trichosporonosis is rare in companion animals with only four previous cases of infection in the cat reported in the literature of which only one was successfully treated. 12,18,19 Of these reported cases two had urinary tract involvement, one cutaneous infection and the fourth had disease of the nasal cavity. Both cats with urinary tract infection had chronic signs of lower urinary tract disease and this chronic mucosal irritation is likely to be an important factor in the development of secondary fungal infection.
Lymphoblastic lymphoma and incomplete clearing of Trichosporon species organisms was diagnosed on necropsy in one of the previous cases 2 months after surgical resection of cutaneous lesions had been considered curative. 18 In the current case there was no evidence of concurrent illness or immunosuppressive disease on physical examination or serological testing and the cat has remained clinically well during the 12-month period since discontinuation of therapy. Thoracic radiographs demonstrated only atelectasis and fungal disease was not identified grossly elsewhere. Vomition or inhalation of a foreign body, mucosal trauma or irritation are the most likely instigating factors in this and the previous case of nasal cavity disease. Localised immunodeficiency and in rare cases nasal neoplasia are proposed contributing factors in dogs with mycotic rhinitis; however, the same has not been demonstrated in cats. 20
In the described case a nasopharyngeal mass was identified and suspected to be due to Cryptococcus species infection on initial histopathological and cytological examination. Nasopharyngeal granuloma formation due to Cryptococcus species has previously been described in cats. 1,21 While the organism identified in this case had several similarities, subsequent examination demonstrated cytological, histopathological and morphological differences.
Cryptococcus species are extremely pleomorphic in cytological and histological preparations with a diameter of 4–15 μm and a shape that may vary from fusiform to a more spherical or globoid appearance. While non-encapsulated forms are occasionally identified, a thick polysaccharide capsule typically is present and this increases overall diameter to 8–40 μm. With Romanowsky-type stains Cryptococcus species organisms are deep pink to deep purple and may appear slightly granular. 22 The cytological and histopathological characteristics of Trichosporon species are rarely described in the veterinary or human literature as colony morphology and polymerase chain reactions are more commonly used diagnostic measures. Where they have been described their appearance is less pleomorphic than Cryptococcus species with a diameter of 3–8 μm and a more uniform spherical to oval shape. Capsular characteristics have been poorly defined, but typically a small to inconspicuous capsule is identified. 12,18 The cytological appearance of Cryptococcus species is demonstrated in Fig. 4 for comparison.

Direct smear of nasal swab from a dog demonstrating Cryptococcus sp organisms. Yeast forms are round to oval, pink staining, and surrounded by a variably sized, thick, clear capsule. Narrow-neck budding is also apparent (arrowhead). Modified Wright-Giemsa, scale bar=20 μm.
Narrow-based budding is described in Cryptococcus species infections and this feature, together with its wide mucoid capsule, usually assists differentiation from other yeast-like organisms. Previous cytological and histopathological examinations of Trichosporon species infections describe narrow-based budding, septate non-pigmented branching hyphae with non-parallel sides and arthroconidia in impression smears and tissue sections. 12,18,23 Pseudomycelial forms, also identified in the case described, are not characteristic of Cryptococcus species organisms.
While both organisms readily stain with periodic acid-Schiff and Gomori's methenamine silver indicating the presence of polysaccharides in their cell wall, Trichosporon species fail to demonstrate the presence of a capsule when stained with mucin stains or India ink. 12 The reason for this lack of staining is unclear, but may be due to the composition of the capsule or that the capsule is of much smaller size compared with Cryptococcus species; the latter is more likely. These techniques could have been used in this case to identify the organism as Trichosporon species.
Histopathological lesions present in this case were similar to those caused by Cryptococcus species organisms, with granulomatous nodules seen although mucinous or gelatinous masses have also been reported previously. 21,23 Trichosporon species was not considered as a potential causative agent initially in this case based on cytological and histological examinations. However, fungal colony morphology was atypical of Cryptococcus species and considered more consistent with Trichosporon species. Molecular methods including DNA sequence analysis are generally required for definitive diagnosis and were also performed in this case. 15 This case highlights the importance of tissue culture as part of the clinical assessment when granuloma formation is suspected to be due to fungal organisms. LCAT is reported to have a high sensitivity and specificity for cryptococcosis 24 although previous reports of false positive results in disseminated trichosporonosis exist. 25 Negative LCAT results in feline fungal disease should first be considered to represent infection with a non-cryptococcal organism rather than a true false negative.
Additional testing including DNA sequencing could have been performed on the previously collected histopathology samples without the need for additional diagnostics. However, these samples were not readily available and as complete re-evaluation of the extent of disease was determined to be necessary and debulking of the granuloma was planned, collection of additional biopsy samples was performed.
Itraconazole was not clinically effective in this case. Failure of therapy may have resulted from inadequate penetration of the large granuloma or an inability of the cat to tolerate safely a sufficient dose resulting in an insufficient duration of therapy. Debulking of the mass may have assisted in successful treatment with itraconazole but was not performed at initial diagnosis and while attempted upon referral was abandoned due to anaesthetic complications. In vitro susceptibility to a number of antifungal agents was determined via MIC testing using a micro-broth dilution technique standardised for Candida species (Sensititre, Trek Diagnostic Systems; Cleveland, Ohio) (Table 1). Direct translation of this information is difficult as MICs vary widely between Trichosporon species and specific breakpoints have not been established. 26,27 In this case fluconazole was chosen on the basis of sensitivity testing and pharmacokinetic studies in cats that indicated plasma concentrations above the MIC were achievable and were, therefore, likely to inhibit growth in vivo. 15,28
Re-evaluation of the amount of remaining disease by re-examination was recommended prior to discontinuing antifungal therapy, but was declined by the owner. Clinical signs as interpreted by the owner were relied upon to determine adequate length of therapy. Six months after commencing fluconazole therapy the cat's owner spontaneously ceased therapy and telephone follow-up over the following 12 months indicated no recurrence of clinical signs. In humans the detection of cell wall components in serum aids diagnosis of invasive systemic mycoses and may also be useful in therapeutic monitoring and prognostication. 29,30 Poor cross-reactivity of Trichosporon species with available galactomannan assays for Aspergillus species is seen 31 and β-d-glucan detection is considered more useful. 29,30 Given the novelty of this infection in veterinary patients the usefulness of such assays for diagnostic or therapeutic monitoring purposes is unknown. However, had increased β-d-glucan been identified in this case a declining titre might have been useful as an indication of successful therapy.
This case represents a clinically successful treatment of a granuloma caused by Trichosporon species infection in a cat. Infection by an otherwise non-pathogenic soil saphrophyte is most likely opportunistic secondary to nasal mucosal irritation or trauma. Tissue culture should be performed to correctly identifying causative organisms especially where LCAT results are negative or where the disease is in an atypical location. Where there is no evidence of concurrent immunosuppressive disease appropriate antifungal treatment can result in successful clinical resolution.