
Abstract
Feline gingivostomatitis (FGS) is a common syndrome in cats; feline calicivirus (FCV), feline herpesvirus 1 (FHV-1), and Bartonella species are common differential diagnoses. In this study, blood from 70 cats with FGS and 61 healthy control cats was tested for Bartonella species antibodies in serum by enzyme-linked immunosorbent assay and Western blot immunoassay and DNA in blood using a conventional polymerase chain reaction assay. Additionally, fresh oral biopsies from cats with FGS (n=42) and 19 healthy controls were tested for FCV RNA, FHV-1 DNA and Bartonella species DNA. The prevalence rates for Bartonella species antibodies and DNA in the blood and the tissues did not differ between the two groups. FHV-1 DNA was also not significantly different between groups. Only FCV RNA was present in significantly more cats with FGS (40.5%) than control cats (0%). The results suggest that FCV was associated with FGS in some of the cats.
Feline gingivostomatitis (FGS) is a devastating, chronic disease of cats that results in painful erosive lesions in the pharynx, buccal mucosa, tongue and gingiva. Clinical signs can include oral pain, halitosis, dysphagia, anorexia, and weight loss. Currently prescribed therapies are variably successful and include combinations of antibiotic therapy, immunosuppressive drugs, interferon therapy, CO2 laser therapy, whole mouth tooth extractions, and a variety of other therapies. In many cats with FGS, cure is not achieved and so therapy is intermittent or chronic and some cats may be euthanized due to a poor quality of life. There are many proposed causes of FGS that include viral agents (feline leukemia virus [FeLV], feline immunodeficiency virus [FIV], feline calicivirus [FCV], feline herpesvirus 1 [FHV-1]), Gram-negative bacteria arising from normal oral flora, exuberant immune reaction to an infectious agent, physiologic or environmental stresses, nutritional factors, and genetic predisposition. 1,2
There have been multiple studies documenting FCV, FHV-1, FeLV, and FIV infections in cats with FGS. However, not all cats infected by these organisms develop FGS which makes interpretation of diagnostic test results in individual cats difficult. Different infectious agents may result in varying oral lesions. For example, caudal stomatitis in cats (previously ‘faucitis’ or ‘palatoglossitis’) appears to be induced by FCV in some cats. 3 Cats with FGS have different tissue cytokine profiles in the faucal tissue than normal cats thus emphasizing the potential for an immune-mediated component to the pathogenesis of the syndrome in some cats. 4
Bartonella species are organisms that have been described as re-emerging pathogens in recent years. Infections caused by Bartonella species can be chronic because of well-developed host evasion mechanisms which include the organism surviving within a number of different cells. 5,6 More recently, Bartonella henselae and Bartonella clarridgeiae have been suggested as an additional potential cause of FGS in two small serologic studies. 7,8 Most Bartonella species infected cats are subclinical carriers but they can exhibit intermittent bacteremia for months to years without apparent clinical consequence. 9,10 Bartonella henselae and B clarridgeiae are transmitted between cats by Ctenocephalides felis and so infection can be extremely common. Depending on the likelihood of flea exposure, studies of healthy cats have documented Bartonella species bacteremia in approximately 24% of cats and Bartonella species antibodies in the serum of up to 93% of cats. 11,12 In naturally exposed cats, Bartonella species have been associated with a number of chronic disease syndromes including uveitis and endocarditis. 13,14 Some experimentally infected cats have mild infiltrates of lymphocytes and plasma cells in some tissues suggesting that immune-mediated disease syndromes could occur in some cats. 15,16
Studies to date that have evaluated the relationship between FGS and Bartonella species are few and contradictory. In the first report, cats with antibodies against both FIV and Bartonella species were more likely than cats with FIV alone or Bartonella species antibodies alone to have FGS. 8 In the second report, 728 cats in Switzerland were tested for Bartonella species antibodies and the results assessed for clinical disease associations. 7 In that study, FGS was overrepresented in cats with Bartonella species antibodies in serum. In contrast, a similar study performed in North Carolina reported no association with FGS and Bartonella species antibodies in naturally exposed cats. 17 Lastly, a recent study of a closed colony of cats failed to show an association between Bartonella species infection or antibodies and FGS. 18 The majority of these studies relied on serum antibody titers to identify active infections. A stronger association between FGS and Bartonella species may be established by amplifying organismal DNA from blood and/or affected tissues and may provide a more reliable means of differentiating active infections from previous exposure to Bartonella species.
The primary purpose of this prospective study was to determine if Bartonella species antibodies in serum or Bartonella species DNA in blood were more prevalent in cats with FGS than in control cats from the same regions of the country. Additionally, the prevalence rates of Bartonella species DNA, FHV-1 DNA and FCV RNA in the palatal tissues of healthy cats were compared to that of cats with FGS to determine if positive test results correlate with the presence of FGS.
Materials and methods
This study was approved by Colorado State University Institutional Animal Care and Use Committee and the participating Humane Society's Director. Client consent was obtained by participating veterinarians.
Case selection and samples: client-owned cats
Client-owned animals were recruited from private practice veterinarians by advertising the study during continuing education lectures throughout the United States as well as on the American Association of Feline Practitioners email listserv and website (www.catvets.com). Samples from all cats with visible FGS lesions (evidence of inflammation or ulcerations along the gingiva, tongue, buccal or lingual mucosa, pharynx or caudal aspect of the oral cavity) and histopathologic descriptions from current or recent biopsies consistent with FGS were accepted into the study. The veterinarians were also asked to submit blood and serum samples from a client-owned healthy cat in the same age range for each FGS cat entered into the study to serve as a geographically matched control.
Veterinarians completed and submitted a form detailing history and current therapies for both the control cats and those with FGS. Case information collected for all cats included age categorized into age ranges (<1 year, 1–3 years, 4–6 years, 7–9 years, 10–12 years, ≥13 years), sex, indoor/outdoor status, single or multi-cat households, time since previous vaccination by time range (within 1 year, 2 years, 3 years, or unknown), vaccination products if applicable, history of fleas, anti-flea products if applicable, FeLV antigen test result, FIV antibody test result, history of signs of upper respiratory infection (URI), and reason for presentation to the clinic. For cats with FGS, the following additional information was requested: severity of lesions (mild, moderate or severe), location of all lesions (buccal mucosa, tongue, palate, gingiva), whether tooth extractions were previously performed, and the products, dosage, and duration of previous or current medications including antibiotics, glucocorticoids, and other drugs. Cats administered antibiotics within 7 days prior to enrollment were excluded because of potential effect on Bartonella species test rests, but other medications, including prednisone, other immunosuppressive drugs, and topical therapies were permitted.
Whole blood (1.5 ml) in EDTA tubes and serum samples (1 ml) from both the cat with FGS and the control cat were requested for enrollment. If the veterinarian was currently anesthetizing the FGS cat for a dental prophylaxis or tooth extraction, fresh tissue (minimum of 25 mg) was collected from a representative oral lesion. Samples were shipped within 24 h or frozen at −20°F and then shipped overnight on a cold pack to the Center for Companion Animal Studies at Colorado State University.
Case selection and samples: humane society cats
Oral biopsies were not available from the client-owned healthy cats and so normal tissues were needed from another source to serve as controls for the FGS tissue biopsies. Tissues were obtained immediately after euthanasia from unadoptable young adult cats housed at a humane society in north central Colorado. The cats were selected based on a normal oral examination. Tissues were collected from the right palatoglossal arch using a new 6 mm skin biopsy punch for each cat within 1 h after euthanasia. The tissue samples were frozen at −20 or −80°C until assayed. The cats had resided at the humane society for 1–33 days and 14/19 cats had been administered a commercially available FCV, FHV-1 and panleukopenia live vaccine for intranasal administration (UltraNasal, Heska Corporation, Loveland, CO) upon admission.
Nucleic acid amplification
On arrival at Colorado State University, DNA and RNA were extracted from tissues (maximum of 25 mg) and DNA was extracted from blood (200 μl) using a commercially available kit (Qiagen, Valencia, CA) following the manufacturer's instructions. Previously described polymerase chain reaction (PCR) assays were used to amplify Bartonella species DNA from blood and tissues as well as FHV-1 DNA from tissues. 19,20 A previously described reverse transcriptase PCR (RT-PCR) assay was used to amplify FCV RNA from tissues. 21
Serological assays
All available sera were assayed for Bartonella species IgG antibodies using a previously reported enzyme-linked immunosorbent assay (ELISA). 22 A titer of >1:64 was considered positive in the ELISA. Sera from 19 client-owned cats with FGS and 19 client-owned control cats that were positive in the Bartonella species ELISA were assayed by Western blot immunoassay. Antibodies against Bartonella species antigens with apparent molecular masses of 8 kDa, 20 kDa, 39 kDa, 48 kDa, 57 kDa, 62 kDa, 69 kDa, 73 kDa, and 82 kDa were considered to be immunodominant based on previous experiments with B henselae experimentally inoculated cats. 22
Statistical analysis
The proportion of cats with a history of URI or Bartonella species antibodies in serum was compared between client-owned cats with FGS and control cats by Fisher's exact test. To further determine the potential association between Bartonella species antibodies and FGS, the distribution of the paired sample results from cats with FGS and control cats submitted by practicing veterinarians were evaluated by logistic regression to determine odds ratios and 95% confidence intervals (GENMOD procedure in SAS, SAS Institute, Cary NC).
Logistic regression was also used to determine associations between Bartonella species ELISA results, health status (stomatitis or no stomatitis), age, flea risk as determined by state, reported flea exposure, housing status, history of a URI, vaccination history, and whether the cat was housed alone or in a multiple cat household. The state of origin was classified as low flea risk (Alaska, Arizona, Colorado, Idaho, Montana, Nevada, New Mexico, Utah, and Wyoming) or high-flea risk (all other states) based on a previous study. 23 The influence of Bartonella species ELISA antibody status (positive or negative) on lesion location and lesion severity was assessed by logistic regression. Wilcoxon's rank sum test was used to determine whether Bartonella ELISA titer magnitude was associated with presence of stomatitis. Because of the small numbers of Bartonella species PCR positive test results using blood from cats with FGS and control cats, statistical comparisons were not made and the results are presented descriptively.
Results of the Bartonella species PCR assay, the FHV-1 PCR assay, and the FCV RT-PCR assay on tissues from cats with FGS and healthy humane society cats were compared by Fisher's exact test. The influence of age, sex, housing, household, vaccination status, URI, administration of glucocorticoids, lesion location, and lesion severity on FCV status (RT-PCR positive or negative) was assessed by logistic regression (GENMOD procedure in SAS, SAS Institute, Cary NC). For all statistical analysis, significance was defined as P<0.05.
Results
Client-owned cat historical and clinical findings
A total of 131 client-owned cats were enrolled in the study, 70 of which had FGS confirmed by prior histopathology and 61 healthy control cats. For some parameters, the information was not available for all cats. The FGS group comprised 41 male-castrated cats and 29 female-spayed cats; the control group contained 35 male-castrated cats and 26 female-spayed cats. The age distribution for the FGS cats was: <1 year (two cats), 1–4 years (18 cats), 4–6 years (14 cats), 7–10 years (18 cats), 11–13 years (seven cats), and >13 years (11 cats). In the control group, age distribution was: <1 year (one cat), 1–4 years (16 cats), 4–6 years (14 cats), 7–10 years (16 cats), 11–13 years (six cats) and >13 (eight cats). Samples (cat with FGS/control cat) were received from Alabama (1/1), Arizona (2/2), California (11/9), Colorado (11/10), Florida (8/8), Illinois (1/1), Indiana (9/4), Massachusetts (1/1), Maryland (3/3), Minnesota (1/1), Montana (1/1), New York (1/1), Ohio (1/1), Oklahoma (2/2), Pennsylvania (1/1), South Carolina (1/1), Tennessee (1/1), Virginia (4/4), Washington (9/8), and Wisconsin (1/1).
Control cats were presented for routine wellness visits (31 cats), boarding (three cats) and one cat each for dental prophylaxis, castration, lower urinary tract infection, upper respiratory tract infection (URI), grooming, constipation, declaw and ‘other’. The remaining 19 cats were listed as ‘control’ or ‘study’ cat. Affected cats were presented for stomatitis (39 cats), routine examination (five cats), dental disease (four cats), gingivitis (two cats) and one cat each for alopecia, anorexia and diabetes, anorexia and lethargy, anorexia and weight loss, bleeding gums, coughing, dental prophylaxis, drooling, diabetes only, halitosis, inappropriate elimination, nasal discharge, oral pain, periodontal disease and URI. For five affected cats, the complaint was listed as ‘study’.
The majority of both groups of cats lived in multiple households (cats with FGS: 63/70 [90.0%]; control cats: 50/60 [83.3%]; unknown; one cat in the control group). Overall, 58/70 (82.9%) cats with FGS and 50/61 (82.0%) of the control cats lived indoors only. Overall, 18/45 (40.0%) cats with FGS and 10/42 (23.8%) of the control cats in which a flea history was known had exposure to fleas. All cats previously assayed for FeLV antigen and FIV antibodies by the participating veterinarian were negative. However, 12 cats with FGS and 14 control cats had not been tested for FeLV antigen and 14 cats with FGS and 17 control cats had not been tested for FIV antibodies. A history of URI was reported in 23/60 (38.3%) of the cats with FGS in which a history was known and 7/56 (12.5%) of the control cats with a known history; this result was statistically significant (P<0.0016).
Lesion location was reported for 68 cats with FGS and varied among the cats (Table 1). Of the 65 cats for which lesion severity was recorded, 2/65 (3.1%) were rated as mild, 21/65 (32.3%) as moderate, and 42/65 (64.6%) as severe. Of the 68 cats with a reported duration of FGS, 44/68 (64.7%) was for >6 months, 7/68 cats (10.3%) was for 3–6 months, 16/68 cats (23.5%) was for 1–2 months, and one case was acute (within 2–3 weeks). Forty-five of 70 cats (64.3%) had been administered one or more antibiotics (amoxicillin, amoxicillin–clavulanic acid, cephalexin, clindamycin, doxycycline, enrofloxacin, marbofloxacin, metronidazole, azithromycin); 24 cats (34.3%) had been administered glucocorticoids; 34 cats (48.6%) had undergone tooth extractions (average number extracted teeth=10.9); and 26 cats (37.1%) had been administered other therapies (topical rinses, pain management, brushing regimens, non-steroidal anti-inflammatory drugs [NSAIDs], laser therapy, antihistamines, lysine and/or novel diets).
Overall distribution of lesions in cats with FGS.

Serum and blood assay results from client-owned cats
Samples from all cats with FGS and control cats were negative for FeLV antigen and FIV antibodies.
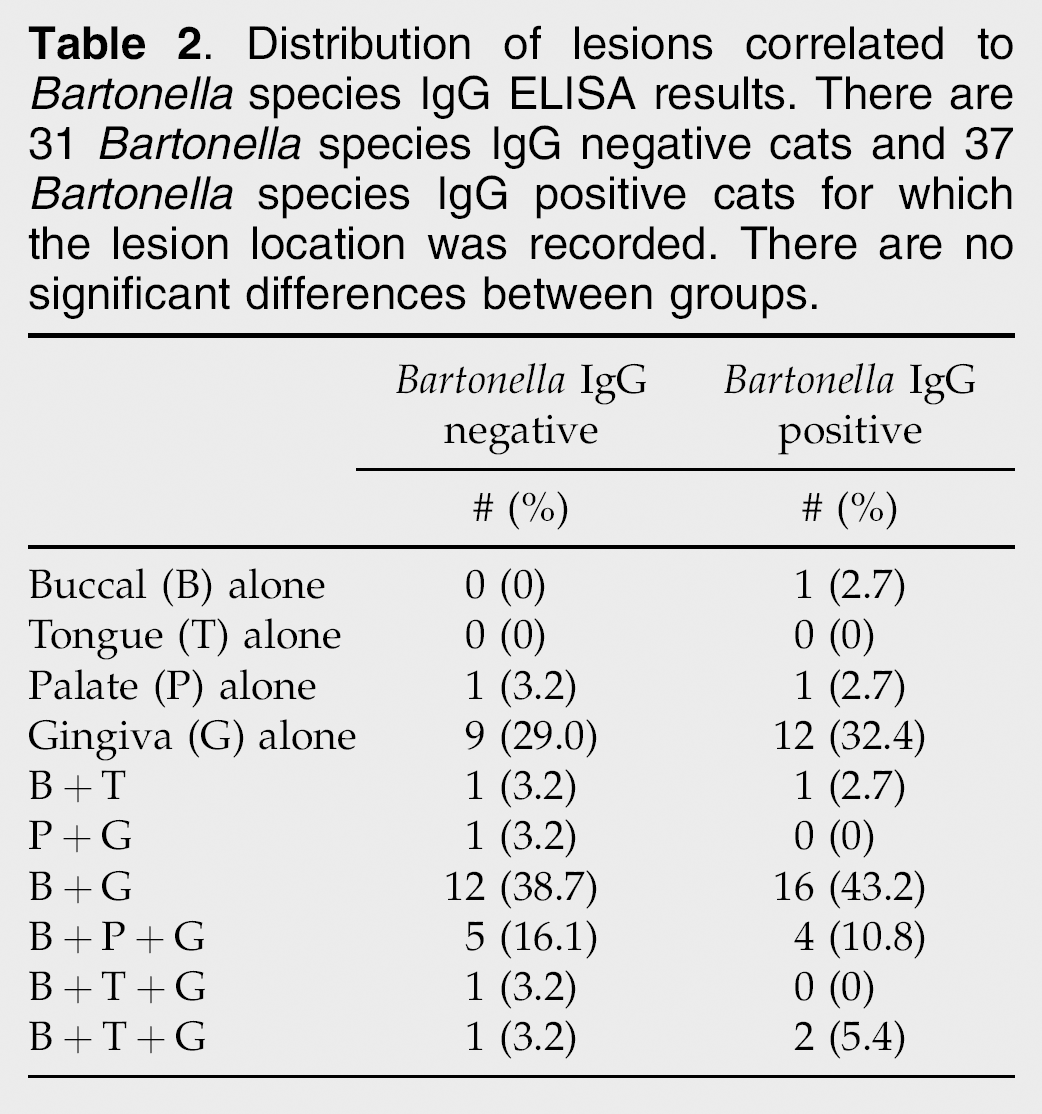
The prevalence of Bartonella spp. antibody titers in cats with FGS (37/70 [52.9%]) and the control cats (36/61 [59.0%]) was not significantly different by Fisher's exact test or logistic regression (P>0.05). However, cats of either group with exposure to fleas or originating from a high-flea risk region were significantly more likely to have a positive Bartonella species IgG titer (P<0.05). There were no significant differences in lesion severity (data not shown) or lesion location between cats with FGS and controls in regards to Bartonella species IgG titer (Table 2).
Distribution of lesions correlated to Bartonella species IgG ELISA results. There are 31 Bartonella species IgG negative cats and 37 Bartonella species IgG positive cats for which the lesion location was recorded. There are no significant differences between groups.
A number of the immunodominant Bartonella species antigens were recognized in serum of cats with and without FGS (Table 3). However, there was no obvious antigen recognition pattern that appeared to differentiate cats with FGS from control cats.
Bartonella species antigen recognition patterns of cats with FGS and control cats.

Numbers of cats recognizing each antigen. There were 19 cats in each group. There were no significant antigen recognition patterns noted between groups.
Bartonella species DNA was amplified from the blood of 8/70 cats (11.4%) with FGS and 5/61 (8.2%) control cats. Bartonella clarridgeiae DNA was amplified from the blood of two of the cats with FGS and two control cats; B henselae was amplified from the blood of the remaining positive cats. Of the Bartonella species PCR positive cats, 12/13 cats were positive for Bartonella species antibodies in serum by ELISA.
Tissue assay results
A total of 42 fresh frozen tissue samples were submitted from cats with FGS and 19 control cats. The results of the Bartonella species PCR assay, FHV-1 assay, and FCV assay were compared between groups and are presented in Table 4. Detection of FCV RNA in a greater number of cats with FGS was the only significant finding (P=0.0006). None of the covariates analyzed for FCV were statistically significant (Table 5). The distribution of lesions in the 17 cats with FGS that were positive for FCV RNA in tissues was: buccal and gingival for nine cats; gingival alone for three cats; buccal, gingival and palatal for three cats; and buccal and tongue for two cats.
Distribution of FHV-1 DNA, FCV RNA, and Bartonella species DNA in tissues of cats with FGS and control cats.

Associations between covariates and the presence of FCV RNA in the tissues of cats with FGS.

The isolate from all three tissue samples that were positive for Bartonella species DNA was B clarridgeiae. Of these, two cats were concurrently positive for B clarridgeiae DNA in blood and all three were Bartonella species serum antibody positive by ELISA.
Discussion
Results of this study failed to make an association between Bartonella species test results and the presence of FGS. These findings could indicate that Bartonella species infections are not associated with this syndrome. Bartonella species infection was initially proposed as a potential cause of FGS in part because of the presence of lymphocytes and plasma cells in tissues of some experimentally inoculated cats which is similar to the infiltrates found in most cats with FGS. 16 However, the infiltrates in cats experimentally inoculated with Bartonella species are generally very mild and to our knowledge FGS has never been reported in a cat with experimentally-induced Bartonella species infection. This includes one group of cats that were co-infected with both FHV-1, another proposed cause of FGS, and B henselae. 24 It is also possible that Bartonella species infections are a cause of FGS but a link was not made because of either our study design or the inherent problems associated with interpreting Bartonella species test results.
Given the wide range of prevalence rates in cat populations, it is not surprising that some cats from both groups tested antibody titer positive for Bartonella species. This makes it difficult to determine if there is a correlation between presence of Bartonella species antibodies and disease. In addition, there were no obvious antigen recognition patterns detected by Western blot immunoassay that correlated to FGS. These findings are similar to a previous report and emphasize that detection of Bartonella species antibodies by any method cannot be used in individuals to prove Bartonella species associated FGS. 18 It was also not surprising to find that a history of flea exposure was significantly correlated with a positive Bartonella species titer as this organism is transmitted by the Ctenocephalides flea. Temperate regions which support the growth and reproduction of fleas would be expected to have a higher prevalence of bartonellosis. Future studies could focus on high-flea regions in order to obtain a sample size large enough for statistical evaluation of the association of Bartonella species and FGS.
In this study, while most cats came from high risk regions and many cats with FGS were Bartonella species seropositive, only small numbers of cats were positive for Bartonella species DNA in blood and tissues precluding statistical analyses. In other studies of naturally infected cats, approximately 24% of seropositive cats are bacteremic and so prevalence rates for Bartonella species DNA in blood or tissues may merely reflect transient bacteremia. 11 However, it is also possible that prior therapy may have lowered Bartonella species DNA levels in the blood to undetectable limits. Of the cats with stomatitis for >6 months, 28/43 (65.1%) had received antibiotics and 64.7% (11/17) of the cats that had a disease duration of 1–2 months received antibiotics. Bartonella henselae infections in humans have been treated with erythromycin, chloramphenicol, gentamicin, trimethoprim–sulfamethoxazole, doxycycline and ciprofloxacin, with various outcomes; however, extended therapy was often necessary in these cases and spontaneous resolution could not be ruled out. 25 Referring veterinarians reporting treatment with antibiotics in our study recorded use of clindamycin, chloramphenicol, enrofloxacin, marbofloxacin, azithromycin, cephalexin, amoxicillin, amoxicillin–clavulanic acid and metronidazole. Although cats were excluded from the study if they had received antibiotics within 7 days prior to sample collection, it is possible that recent use of antibiotics may have decreased the organism load below the level of the PCR assay detection or that previous therapy temporarily cleared the organism from the bloodstream. Doxycycline therapy suppressed bacteremia in 4/8 cats in one experimental study, but bacteremia returned within 3 weeks of therapy. 26 The time elapsed from antibiotic therapy was not reported by the referring veterinarians in our study so it cannot be determined if temporary suppression of the organisms accounted for the lack of significant difference in the affected cats compared to the controls.
There were notable discrepancies between results of PCR using blood and tissues from the FGS cats. Eight cats had Bartonella species DNA (six B henselae; two B clarridgeiae) amplified from blood, but DNA of a Bartonella species was only amplified from tissues of two of these cats (B clarridgeiae). A third cat had B clarridgeiae DNA amplified from tissues but was negative in blood. These results suggest bacteremia does not always imply distribution of the organism to tissues and vice versa. And although the number of cats in which Bartonella species was present in the tissues was small, all three cats were positive for B clarridgeiae. These results may suggest that this species may have different virulence characteristics that could lead to FGS in susceptible cats. However, such a supposition needs to be investigated further. Bartonella species were detected in the tissues of 8.8% of the FGS cats but in none of the tissues from the humane society cats, though this difference was not significant. The control cats for these tissue comparisons were all cats from Colorado which carries little risk for flea exposure and so these data should be discounted. The three cats that had Bartonella species DNA amplified from the tissue were from Indiana, Maryland and Virginia where flea exposure is more likely. A larger control group from a flea region would perhaps provide a more meaningful data for this organism.
The host-dependent immune response to an organism may determine the outcome of an infection in that host. One murine study of immunocompetent mice has implicated a predominantly T-helper type 1 (Th1) cell-mediated response to parenteral infection with B henselae while another demonstrated a mixed Th1 and Th2 phenotypes in response to both parenteral and mucosal routes of infection. 27,28 One feline study compared the cytokine profile of FGS cats to healthy controls cats. Cats with FGS demonstrated a mixed type 1/type 2 response while a type 1 cytokine profile was the typical response in cats without FGS. 29 This finding suggests that the cell-mediated response may be altered in cats with FGS and may explain why some cats develop FGS and others do not given the same antigenic stimulation. The inciting organism, such as Bartonella species, may have been cleared from the blood and the tissues, but produced an aberrant mixed immunologic response that perpetuates the oral inflammation. It would, therefore, be difficult to isolate an individual antigen responsible for the FGS. This host–pathogen interaction may explain why the results of this study with respect to Bartonella species are not significant.
The finding that a history of URIs was significantly associated with cats with FGS in this study was the impetus for investigating the presence of DNA or RNA from other infectious disease agents within the tissues. The most common etiologies for URIs in cats include FCV, FHV-1 and Chlamydophila felis. 30 FCV has been previously implicated as an etiologic agent in FGS. In one study of FGS cats, FCV was isolated from the oropharynx in 92% of 36 British cats presenting to a university and 79% of 42 cats presenting to general practices compared to controls (19% in both populations). 31 In another study, 88% of cats with chronic FGS presenting to a referral dentistry practice were shedding both FCV and FHV-1. Recently, an FGS cat treated with thalidomide became FCV negative at the same time as clinical resolution of the FGS was noted. 32 Acute FGS has been induced in experimental studies of FCV, but chronic FGS has not been experimentally reproduced using FCV as an agent, nor has progression from acute to chronic FGS been documented. 33 Given that tissues from the humane society cats were likely to have had high exposure to FCV in the humane society environment and the majority of these cats received an intranasal vaccine, we would have expected this group to have a high prevalence of FCV RNA amplified from the tissue from either exposure or the vaccine. Thus, detection of FCV RNA in the tissues of more cats with FGS than humane society cats suggests a disease association with FCV. However, we failed to show an association between FCV RNA in tissues and lesion severity or location. This may indicate that all the lesions reported could be associated with FCV or may merely reflect the small sample size in the study.
We also failed to show a significant difference between either of the groups with respect to FHV-1 DNA in the tissue. Like FCV, FHV-1 is associated with URIs in cats and may become a latent or chronic infection. In addition, one study demonstrated that 88% of cats with FGS were shedding both FHV-1 and FCV in the saliva simultaneously. Therefore, FHV-1 might be expected to induce FGS in some cats. In our study, only two cats from the FGS group and no cats from the control group had dual FHV-1/FCV infections so there did not appear to be a permissive effect of either virus. But because FHV-1 is so widespread in the cat population, including healthy cats, larger numbers of cats may be required to observe a significant difference.
As discussed, there are a number of limitations to this study. As it is likely that FGS is multi-factorial, it will continue to prove difficult to make disease associations in individual cats. In a future study, it would be optimal to develop a lesion scoring and localization system in collaboration with veterinary dentists to try to more tightly standardize criteria.
Footnotes
Acknowledgements
The project was funded by a grant from the American Association of Feline Practitioners and was supported by the Center for Companion Animal Studies at Colorado State University (![]() ). For editing comments, thanks go to Brian Hewitt, DVM, Cheyenne West Animal Hospital, 3650 N Buffalo, Las Vegas, NV 89129.
). For editing comments, thanks go to Brian Hewitt, DVM, Cheyenne West Animal Hospital, 3650 N Buffalo, Las Vegas, NV 89129.