
Abstract
Medical records of 77 cats that had clinical signs of vestibular disease and magnetic resonance imaging (MRI) of the head were reviewed retrospectively. The aetiological, clinical and MRI characteristics were described and evaluated for a relationship with patient outcome. Forty cats (52%) had signs of central vestibular dysfunction (CVD), which was part of a multifocal disease in 17 cats (43%). The most frequent causes of CVD were inflammatory conditions (18 cats; 45%), including bacterial inflammation as an intracranial extension of otitis interna (five cats; 13%), feline infectious peritonitis (three cats; 8%) and toxoplasmosis (two cats; 5%). Neoplasia (12 cats; 30%) and vascular disease (four cats; 10%) were respectively the second and the third most frequent causes of CVD. Thiamine deficiency was diagnosed in one cat based on MRI findings and improvement following vitamin B1 supplementation. Of 37 cats (48%) with peripheral vestibular dysfunction (PVD), idiopathic vestibular syndrome (IVS) was suspected in 16 (43%) and otitis media/interna was suspected in 16 (43%). Within the group of cats with evident MRI lesions, the location of the imaged lesions agreed with the clinical classification of vestibular dysfunction in 52/55 (95%) cats. Most of the cats (nine cases; 56%) with presumed IVS had rapid and complete recovery of their clinical signs. As most of these cats presented with progressive clinical signs over 3 weeks they were classified as having ‘atypical’ IVS to differentiate them from cats with the typical non-progressive IVS. No underlying systemic diseases were documented in any of these cases. Statistically significant predictors of survival included neurolocalisation (central or peripheral vestibular system), age and gender. No difference in survival was observed between cats with presumed idiopathic peripheral syndrome and cats with otitis media/interna.
Vestibular dysfunction refers to any of the clinical signs that reflect disease affecting any part of the vestibular system. These signs are usually unilateral and may include loss of balance, asymmetric rolling, leaning or falling ataxia, head tilt, spontaneous/positional nystagmus and/or strabismus. 1 Otitis media/interna and idiopathic vestibular syndrome (IVS) are considered the two most frequent aetiologies for cats with peripheral vestibular dysfunction (PVD). 1–3 Central vestibular dysfunction (CVD) in cats may be caused by tumours, inflammatory/infectious diseases, 1,4,5 thiamine deficiency, 6 vascular, 3 traumatic, 3 and toxic conditions. 7 Congenital conditions are infrequently associated with CVD. 1 Therapy and prognosis in animals with vestibular dysfunction depend on lesion localisation and aetiology. Of the methods used to investigate vestibular dysfunction, cerebrospinal fluid (CSF) analysis or radiography do not usually enable definitive diagnosis. 8 Computed tomography (CT) is more sensitive for investigation of middle and inner ear diseases than radiography, 9 but visualisation of the caudal fossa (cerebellum and brainstem) is limited by bone-related artefacts when using this modality. 10 Magnetic resonance imaging (MRI) is considered the imaging test of choice to investigate causes of intracranial causes of vestibular dysfunction and inner ear anatomy is also well depicted, especially on T2-weighted images because the endolymph appears markedly hyperintense in comparison to surrounding structures. T1-weighted images following intravenous contrast administration are useful for detecting inflammatory conditions of the inner ear. A few reports, 11–14 and one case series, 5 have described MRI findings in dogs with vestibular dysfunction. There are far fewer MRI reports of cats with vestibular dysfunction and these include cases with otitis media/interna, brainstem abscessation and intracranial neoplasia. 4,11
The relative frequency of diseases causing peripheral and central vestibular signs in cats has not been investigated with MRI in a large number of cases. Such knowledge would aid differential diagnosis, formulation of a rational diagnostic plan and prognosis. Anecdotal evidence has suggested that many cats with progressive PVD have negative diagnostic tests, including MRI. The clinical outcome of such cats is largely unknown and this formed part of the current investigation.
The aims of the present study were to describe the epidemiology, clinical and MRI findings in a series of cats with vestibular signs and to identify associations between these variables and patient outcome.
Materials and methods
Selection criteria
Medical records for the period January 2001 to May 2006 at The Queen Mother Hospital for Animals, Royal Veterinary College, University of London, and the Animal Health Trust were searched for cats with clinical signs consistent with vestibular dysfunction, which had undergone MRI of the head and had a minimum follow-up of 3 months after diagnosis. Data from the medical records included signalment, history, clinical signs, neurolocalisation, MRI results, CSF analysis (total and differential cell count, total protein count, cytology), infectious disease serology and polymerase chain reaction, thoracic and abdominal imaging, presumptive diagnosis and results of histology when available. Telephone follow-up of all cats discharged alive was attempted in May 2006. Outcome was classified as alive, lost to follow-up, death as a result of vestibular disease, death for another reason or death due to unknown cause.
Vestibular dysfunction was defined on the basis of observing loss of balance, typical ataxia, presence of head tilt, spontaneous/positional nystagmus and/or positional strabismus. Cats with these neurological signs alone were classified as having peripheral vestibular signs. Cats with markedly depressed mental status, proprioceptive deficits and cranial nerve deficits (affecting nerves other than VII or VIII) were classified as having central vestibular signs, according to established practice. 1 Cats were classified as having paradoxical vestibular syndrome when neurological deficits typical of a CVD were observed with a contralateral head tilt and/or circling towards the lesion. Bilateral peripheral vestibular syndrome was defined by observing typical oscillating (side to side) movements of the head and a lack of head tilt in cats with other signs of peripheral vestibular localisation.
MRI protocol and review
MRI (Gyroscan 1.5 Testla, Philips) was performed using a 1.5 T magnet. In all cats, T1- and T2-weighted images, T1-weighted images post contrast administration (intravenous administration of 27.9 mg/kg gadoteric acid [Dotarem; Guebert Laboratories]) were acquired in three different planes (dorsal, sagital and transverse planes). Fluid attenuated inversion recovery (FLAIR) and/or T2* (gradient echo) images were also acquired in selected cases. MR images were reviewed by two board-certified radiologists who reached a consensus on the image findings. Anatomic site, distribution (focal/multifocal/diffuse, intra/extra axial), margins, ventricle enlargement and cerebrum/cerebellum herniation were recorded. Signal intensity of lesions and presence of any increase in signal intensity after gadolinium administration were also noted.
Statistical analysis
Survival analysis was performed using Kaplan–Meier estimates of mean survival time and Cox proportional hazards regression. Cross tabulations and Fisher's exact tests were used to look for associations between disease localisation (central or peripheral) and outcome. Cross tabulations were repeated to determine the effect of the coding of outcome on the association with disease localisation. Results were expressed as hazard ratios (HRs) and mean survival times (MST). Differences with P<0.05 were considered significant.
Results
A total of 77 cats with clinical signs of vestibular disease were included in this study. No specific breed was over-represented compared to the hospital population; males were more commonly affected than females (46 vs 31) and the median age of the affected cats was 7 years old (range 6 months to 15 years). On the basis of the neurological examination, 40 cats (52%) were classified as having unilateral CVD, one cat had a paradoxical vestibular syndrome and the remaining 36 (47%) cats had PVD, of which five (14%) had bilateral clinical signs. Cats with CVD reportedly had an equal distribution of acute or gradual onset of signs, whereas an acute onset of clinical signs was reported by owners of 27 (75%) cats with PVD. Most cats (86% those with CVD and 88% those with PVD) had progressive clinical signs, with median duration of 19 days (1–34 days) between the owner first noticing an abnormality and diagnosis.
A MRI scan was performed in all cases and lesions were detected in a total of 55 cats. Within the group of cats with evident MRI lesions, imaged lesions correlated with clinical classification of either PVD or CVD in 52 (95%) cats.
Cats with CVD
Of the 40 cats with central vestibular signs, 37 (93%) appeared to have a depressed mental state, 36 (90%) had cranial nerve deficits other than VII and VIII and 34 cats (85%) had hemi/tetraparesis and/or proprioceptive deficits. Twenty-three (58%) of the cats with CVD had detectable nystagmus, which was positional in 19 cases (49%). Nystagmus was horizontal in 19 cats (49%) and vertical or rotatory in the remainder.
Six cats (15%) with clinical signs consistent with CVD did not have any detectable MRI lesions, with most of them (four cats; 66%) having a focal clinical localisation. In these cats, CSF analysis was normal and necropsy, available in three cases, revealed a diffuse central nervous system lymphoma (one cat), multifocal lymphocytic meningoencephalitis (one cat) and an ischaemic midbrain lesion (one cat).
Of the 34 cats with CVD and detectable MRI lesions (85%), 18 (53%) had a focal lesion and the remaining 16 (47%) had multifocal lesions (Fig. 1). One cat with multifocal lesions had no evidence of brainstem involvement on MRI. Interestingly, MRI detected multifocal lesions in 6/24 cats clinically suspected of a focal central vestibular system lesion, while 4/16 cats with a clinical multifocal localisation had a focal lesion detected, as reported in Table 1. The location of lesions (focal vs multifocal) on MR images agreed with the clinical classification of vestibular signs in 60% of CVD cats. In the 18 CVD cats with focal MRI lesions (53%), involvement of the brainstem was due to either primary or secondary disease (ie, mass effect or hydrocephalus) in 83% of cases, while one cat had a peripheral bulla lesion with no detectable intracranial extension and one cat had a focal vascular lesion affecting the contralateral thalamus.
Transverse MR images of histologically confirmed pyogranulomatous meningitis in a cat with multifocal neurological signs (CVD and forebrain). In T1-weighted images there is a midline shift to the left and obliteration of the right lateral ventricle compatible with a mass effect. Marked thickening, enhancement following administration of contrast medium and hyperintensity on T2-weighted images is evident affecting the pachymeninges over the right temporal lobe. Left side of the picture corresponds to right side of the cranium.
Correlation between neurolocalisation and location of lesions in MR images on cats with CVD is 60%. Kappa=0.30 (95% CI 0.05–0.55).

The most frequent cause of CVD based on the results of all the tests available was inflammation (18 cats; 45%). This group of cats, with mean age of 4 years 3 months (range 7 months to 8 years), included five cases with meningoencephalitis from otogenic intracranial extension (Fig. 2), confirmed by CSF analysis compatible with a mixed predominantly neutrophilic pleocytosis in all cases and a positive bacterial culture of material collected by myringotomy in two cases; three cats with feline infectious peritonitis (FIP), two confirmed using histopathology and one through serology in CSF and blood samples and two cases with toxoplasmosis confirmed at necropsy. Specific aetiology in the other eight cats was unknown; in these cats histopathology detected mononuclear multifocal meningoencephalitis/encephalitis. Viral or immune-mediated origin cannot be ruled out.

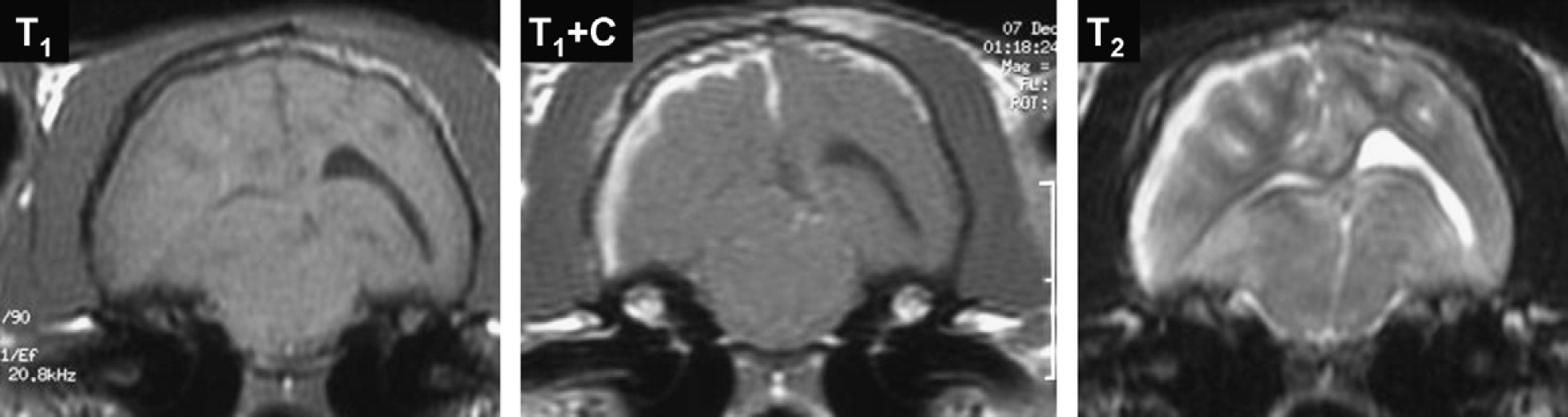
Transverse MR images of a cat with central vestibular signs on the left side, as a result of meningoencephalitis due to intracranial extension of otitis. Tissue in the dorsal part of the left tympanic cavity is associated with a diffuse meningeal lesion on the left/dorsal aspect of the cerebellum (arrows) characterised by hypointensity on T1-weighted images, enhancement of a peripheral narrow rim of tissue following administration of contrast medium (T1+C) and hyperintensity on T2-weighted images. Left side of the picture corresponds to right side of the cranium.
Of the five cats with otogenic intracranial extension, neurological signs compatible with a focal CVD were recorded in three cases, while two cats, despite the moderate pyogranulomatous intracranial inflammation, were clinically localised as PVD (Fig. 3). Broad-spectrum antimicrobial therapy was instituted in all five cats with otogenic bacterial meningoencephalitis using amoxicillin and clavulanic acid (22 mg/kg bid) and metronidazole (15 mg/kg bid). The two cats with milder neurological signs (localised as PVD) showed marked improvement; one other cat showed mild improvement and was euthanased a month after the diagnosis, while the remaining two cats were euthanased within a week of diagnosis for poor condition. Cats with FIP (three) and toxoplasmosis (two) had multifocal neurological signs; specifically, central vestibular signs and seizures. Corticosteroid treatment was initially instituted in all cats with FIP; however, euthanasia was performed within 10 days of diagnosis due to neurological deterioration.

Transverse MR images of a cat with peripheral vestibular signs on the right side associated with chronic otitis media/interna with intracranial extension. The right tympanic bulla is diffusely thickened (arrow) and filled with tissue characterised by isointensity on T1-weighted images, uneven peripheral enhancement following administration of contrast medium (T1+C) and hyperintensity on T2-weighted images. The perilymph in the right inner ear has slightly increased signal intensity in T1-weighted images and reduced signal in T2-weighted images. Contrast accumulation on the right/ventral aspect of the brainstem is compatible with meningitis. Left side of the picture corresponds to right side of the cranium.
Neoplasia (12 cats; 30%) was the second most frequent cause of CVD. Mean age of cats with CVS due to neoplasia was 7 years 9 months (range 5–10 years). Tumour type included meningioma (n=4) (Fig. 4), lymphoma (n=3), squamous cell carcinoma (n=1), schwannoma (n=1) and metastasis of a carcinoma (n=2). Two of the cats with lymphoma had focal clinical localisation and detectable lesions on MRI in the caudal brainstem, while in 2/4 cats with meningioma at the level of caudal brainstem, neurological signs were compatible with multifocal localisation, although no signs of cerebellar herniation or severe hydrocephalus were detected. The cat with squamous cell carcinoma was clinically compatible with a focal lesion of the brainstem and MRI was able to detect the primary lesion site (latero-rostral-retrobulbar part of the calvarium).
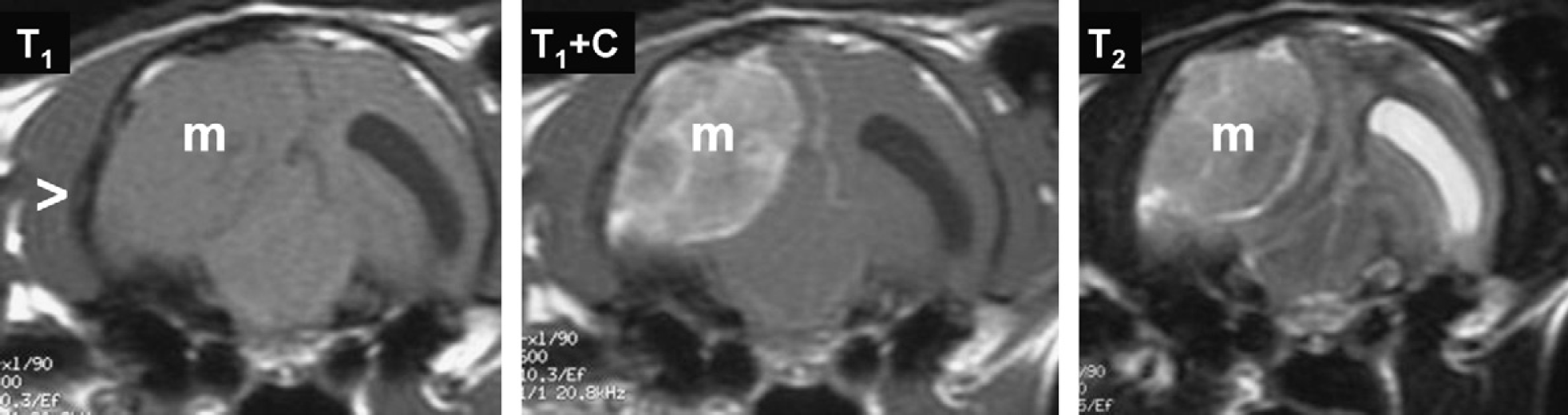
Transverse MR images of a large meningioma impinging on the right temporal lobe in a cat with multifocal central nervous system (CNS) localisation (CVD and forebrain). The mass (m) is characterised by isointensity on T1-weighted images, moderate heterogeneous enhancement following administration of contrast medium (T1+C) and heterogeneous intensity on T2-weighted images. The medial aspect of the mass is delineated by CSF compatible with an extra-axial origin of the mass. The temporal bone adjacent to the lateral aspect of the mass is slightly thickened (arrowhead) suggestive of hyperostosis. The left lateral ventricle is dilated. The thalamic lesion observed in this cat may explain the vestibular signs considering the thalamic functioning as a relay station of afferent vestibular inputs to cortex. Left side of the picture corresponds to right side of the cranium.
A vascular disease was suspected in four cats (10%) (Fig. 5), while one cat (1.3%) was suspected of thiamine deficiency based upon characteristic MRI findings and improvement following vitamin B1 supplementation. Of the six cats with multifocal MR lesions and clinically focal localisation, three had an inflammatory disease, two a vascular condition (haemorrhagic infarct) while in one cat a metastatic neoplasia was suspected on the basis of MRI findings and biopsy of a pulmonary mass consistent with adenocarcinoma. In cats suspected of a vascular condition, systemic blood pressure was monitored and in all cases was within normal limits.

Transverse MR images of acute haemorrhage in a cat with central vestibular signs on the right side. A focal lesion in the region of the right vestibular nuclei (arrow) is hyperintense on both T1- and T2-weighted images. Left side of the picture corresponds to right side of the cranium.
Cats with PVD
Thirty-seven cats (48%) were clinically suspected to have disease affecting the peripheral vestibular system; 32 cats (87%) presented with signs of unilateral peripheral vestibular system lesion while five cats (13%) had bilateral peripheral vestibular syndrome. Acute and progressive clinical signs, over a 3 week-period, were reported in most of the cats, with both unilateral (75%) and bilateral (80%) PVD. Obtunded mental status was observed in 15/37 cats (40%), the majority of them had otitis media/interna (12/15), without intracranial extension of infection, one cat was affected by aural neoplasia and one cat suspected to have atypical IVS. Pain and sense of disorientation was considered a likely explanation for the depressed mental status. None of the cats with bilateral peripheral vestibular syndrome had nystagmus, which was present in 46% of cats with unilateral PVD. Nystagmus was horizontal in 70% of these cases and rotatory in the remainder, while positional was recorded in 42% of the cats with nystagmus.
Visible lesions were observed on the MR images of 21 cats (57%) with clinical PVD. The most common lesion site was the middle-inner ear (18 cats; 86%), which was suggestive of otitis media/interna in 16 cats (76%), while aural neoplasia (Fig. 6) and an inflammatory polyp were each suspected in one cat, respectively. Diagnosis of otitis media/interna was confirmed in 10/16 by cytological evaluation and bacterial aerobic/anaerobic culture of material collected by myringotomy. Mean age of cats affected by otitis media/interna was 6 years 1 month (range 1–11 years). Staphylococcus intermedius was the most frequent pathogen isolated (five cats); less frequently, Staphylococcus aureus (one cat), Escherichia coli (one cat), Enterococcus species (one cat), Pseudomonas aeruginosa (one cat) were isolated from material collected through myringotomy. In one cat, aerobic and anaerobic culture from the tympanic cavity content was negative while cytology of the same material was compatible with a chronic inflammation. The cat, however, responded well to treatment with amoxicillin and clavulanic acid (22 mg/kg/bid for 8 weeks). Cats with otitis media/interna were medically treated with a broad-spectrum antibiotic therapy, including amoxicillin and clavulanic acid (22 mg/kg bid) combined with metronidazole (15 mg/kg bid) or clindamycin (15 mg/kg bid) until specific bacterial sensitivity was available from the culture and sensitivity. Initial protocol was continued for a minimum of 8 weeks where antimicrobial susceptibility testing was not available or was negative. No cats with otitis media/interna were surgically treated due complete resolution of clinical signs with medical therapy.

Transverse MR images of aural neoplasia in a cat with left peripheral vestibular signs. A large mass (m) obliterates the left tympanic bulla and is characterised by isointensity on T1-weighted images, peripheral enhancement following administration of contrast medium (T1+C) and heterogeneous intensity on T2-weighted images. There is a fluid air interface evident in the right tympanic cavity (arrow) (cat was in dorsal recumbency). Left side of the picture corresponds to right side of the cranium.
Of the remainder of cats with PVD and evident MRI lesions (3/21), focal brain lesions (one in the brainstem and one in the cerebrum, respectively) both compatible with vascular accidents were recorded in two cats (5%), and focal meningitis with suspected VIII cranial nerve neuritis diagnosed by MRI and CSF analysis in one cat. Of the five cats (14%) with bilateral peripheral vestibular syndrome, presumed bilateral otitis media/interna was recorded in four cats, while no lesions were detected on MRI in one cat. In the four cats with MRI lesions compatible with otitis media/interna, myringotomy was performed in one cat and chronic inflammation was observed on cytology, while bacterial culture was negative. However, presumptive diagnosis of bacterial otitis media/interna was based on complete resolution of clinical signs and, in two cases, of the MRI lesions observed in a second MRI after broad-spectrum antibiotic therapy of long duration, as reported above.
Of the cats with evident MRI lesions (n=21), agreement between clinical localisation and MRI lesion site was present in 19/21 cats (90%). Two cats with vascular brain lesions were misdiagnosed as having a peripheral localisation. In both these cats, systemic blood pressure measurement, blood tests, coagulation profile, abdominal ultrasound and thoracic radiographs did not establish an underlying cause.
In 16 (43%) of the 37 PVD cats, MRI could not detect any abnormalities. The mean age of these cats was 5 years 2 months (range 6 months to 13 years); according to the owners, 11 of 16 cats (69%) had acute progressive clinical signs over a mean period of 3 weeks time; three cats (19%) had acute non-progressive signs and chronic progressive signs were reported in two cases (12%). Ancillary diagnostic tests, including complete blood count, serum biochemistry, chest radiographs, abdominal ultrasound and CSF analysis were normal in all of these cats, which were classed as having a atypical IVS. No treatment was instituted for these cats. Most of these cats (eight; 50%) with atypical IVS had a complete recovery within 3 months and no recurrences were reported by the owners over a mean period of 13.6 months (5–21 months). Of the remaining cats, head tilt persisted in two cases (12%), one showing acute progressive signs and the other with chronic onset and progression of the signs over 2 weeks. One cat, originally presented with chronic and progressive signs, did not improve and was euthanased soon after the diagnosis, without necropsy. Five of the atypical IVS cats were lost to follow-up. Recurrence was recorded in one cat (6%), which had experienced a residual head tilt. No treatment was instituted for the three cats affected by typical IVS and complete recovery was observed in two of them within 3 months, while a mild intermittent head tilt was reported by an owner of one cat.
Outcome analysis
Follow-up was obtained in 64 cases (83%). Thirty-eight cats had died at the time of follow-up collection. Twenty-six cats died due to cause of the vestibular while unrelated to vestibular disease in nine cases and of unknown causes in three cases. Mean survival time (MST) was 1301 days, independent of the cause of death; in fact, changing the coding of cats as events or censored cases did not change the results. For example, classifying only those cats that died due to their vestibular disease as events (n=14) simply increased the hazard ratio (HR=6.5, 95% confidence interval [CI]: 1.8–23.9, P=0.005).
Of the cats which died due cause of their vestibular disease, most of them (23; 88%) presented with a lesion of the central vestibular system; therefore unsurprisingly, cats with CVD were more likely to die when compared to cats with PVD (HR=3.2, 95% CI: 1.5–6.8, P=0.004). Censoring cases with unknown outcomes did not change the results, confirming the lesion site rather than the nature of lesion had a direct association with prognosis.
Age was a significant predictor of survival in all models with older cats being more likely to die (P≤0.05). Gender was also significant with males being more likely to die (P≤0.03). There was no difference in survival between cats with atypical IVS or cats with PVD due to otitis media/interna or typical IVS.
Discussion
The most common causes of peripheral vestibular signs in cats in this study were the atypical form of IVS and otitis media/interna. Both were commonly associated with a good prognosis and potential for complete resolution of clinical signs, as reported previously. 1,3,6 These data are similar to those recently reported by Garosi 3 who detected high incidence of idiopathic peripheral vestibular syndrome (IVS), in almost a third of dogs with peripheral vestibular signs. Traditionally, inflammation (otitis media/interna) and neoplasia were considered the main causes of PVD 5,6 while IVS was supposed to occur sporadically and more commonly in geriatric dogs. 3
In the group of cats affected by atypical IVS, signalment, history, neurologic findings, MRI scan of the brain, and follow-up data were reviewed. In all of these cats, a normal MRI and ancillary diagnostic work-up suggested an idiopathic vestibular disease. However, classically, the literature describes IVS in cats as an acute onset disease with no progression of clinical signs, which frequently improves to a normal status within 2–4 weeks, 3 however, mild residual head tilt and ataxia may remain permanently. In the present study, most cats with IVS had progressive clinical signs (atypical form), which may represent a novel form of IVS in cats or mild structural causes of PVD not detectable on MRI such as early otitis media/interna. However, improvement of clinical signs without treatment were observed in all cases of atypical IVS, without any therapeutic attempts, except for one cat which only demonstrated mild improvement after 10 months from the time of diagnosis. In the USA, a seasonal and geographic influence on the occurrence of IVS has been reported, which has increased prevalence in spring and autumn seasons in the north eastern states 3 ; however, similar data on seasonal associations are not available in Europe, 3 and were not evaluated in the present study. The possibility of damage to the middle and inner ear structures secondary to Cuterebra larval migration was recently suggested 15,16 as a possible explanation for cats affected by ‘seasonal’ IVD in the USA.
Some of the idiopathic vestibular diseases may actually represent a self-limiting inflammatory lesion of the peripheral vestibular apparatus, not identified on MRI, similar to that described in human beings. 17 Idiopathic vestibular neuritis in humans is characterised by an absence of evident lesions on MRI and absence of underlying systemic diseases. 17–19 The aetiology of this acute idiopathic vestibular neuritis is still unclear. Reactivation of human herpes virus simplex 1 has been suggested as the most likely cause, 17,20 as variable contrast enhancement has been observed using 3 T MRI and a high dose of gadolinium contrast, 20 resembling herpes zoster neuritis/labyrinthitis and Cogan's syndrome. 17 Lower resolution MRI (1.5 T MRI), similar to the one used in the present study, could not detect any lesions in human patients with these diseases, even when high doses of gadolinium were used. 17 In humans, although neurological signs associated with vestibular neuritis tend to improve spontaneously, different treatment protocols with steroids alone (prednisone, methylprednisolone – MP) or associated with antiviral agents (valacyclovir – VLC) have been reported. 21,22 In Strupp's study 22 on efficacy of different therapeutic protocols for vestibular neuritis, monotherapy with MP, VLC and combination of MP and VLC were compared to a placebo treatment. On long-term follow-up (12 months), significant improvement of neurological signs was associated with MP monotherapy but not with VLC monotherapy; moreover, the combination of MP and VLC was not superior to corticosteroid monotherapy. On the other hand, in a more recent study, 21 high-dose prednisone therapy was associated with an earlier recovery, based on 1–3 months follow-up, but not an improved long-term prognosis. In cats affected by IVS, no studies on the efficacy of different treatment protocols have been reported and based on the good prognosis reported in this study, the utility of a specific treatment protocol is unclear.
Despite the good prognosis for most cats with otitis media/interna, MRI detected intracranial extension of an inflammatory process originally affecting the ear in five cats in this study; two of these cats did not show any neurological signs of CNS involvement and were clinically localised to the peripheral vestibular system. While, historically, the diagnosis of otitis media/interna can be based on clinical signs and confirmed by radiographic or CT, the presence of subtle forms of intracranial extension of the inflammatory process into the caudal brainstem, cannot be easily detected using these imaging techniques. 10 Such extension may not be accompanied by any clinical signs until it evolves into brain abscessation 11 ; therefore, MRI evaluation of the bullae, inner ear and brainstem structures is particularly important in cases of suspected otitis media/interna, to rapidly confirm a lesion localisation, suggest a diagnosis and start specific treatment.
Inflammation was the most frequent cause of central vestibular signs (45%) in this study. In almost half of these cases (44%), an aetiological diagnosis for the inflammation could not be ascertained. Neoplasia appeared to be the second most frequent condition affecting the central vestibular system of cats in this study, while it is a quite infrequent cause of PVD. Meningioma and multicentric lymphoma were identified as the most frequent types of neoplasia responsible for CVD in this study, confirming data previously reported in the literature. 1,3,4
Based on the outcome analysis in this study, prognosis is associated with lesion site rather than the aetiology and it was not surprising that CVD was associated with a poorer prognosis than PVD in cats. Moreover, in the group of diseases affecting the peripheral vestibular system, otitis media/interna and idiopathic vestibular conditions have a similar good prognosis, if appropriate treatment with specific antibiotics is completed in cases of the former.
High quality, multiplanar MRI of the peripheral vestibular system and brain is invaluable in comparison to other diagnostic imaging techniques, such as CT. In this study, MRI detected multifocal brain lesions in four cats which presented with focal clinical signs; this is a similar experience to that documented in dogs by Garosi et al. 5 However, concerns arising in this study result from the potential lack of sensitivity of MRI in detecting lesions as three cats of this study with CVD had no observable MRI lesion despite being histologically documented with inflammatory, vascular and neoplastic (lymphoma) disease, respectively. Based on the retrospective nature of this study, lack of specific sequences such as FLAIR or T2* images, may have affected the rate of MRI sensitivity, increasing the false negative cases.
In the present study, MRI findings corresponded to clinical localisation in 95% of cases (Table 2). In particular, cats affected by PVD had higher (94.6%) agreement between MR images and clinical localisation than cats with CVD localisation (82.5%), as reported in Table 2. However, in cats with CSN diseases, the accuracy in determining the presence of focal vs multifocal lesions based on clinical or imaging findings is estimated to be 60%, as presented in Table 1. Multifocal lesions observed on MRI were not clinically suspected in six cats with focal caudal brainstem localisation. On the other hand, multifocal neurolocalisation was not supported by MRI findings, consistent with focal CNS lesion, in other four cats. Similarly, in Garosi's study in dogs, 5 although MRI could detect lesions in all cases with a central vestibular localisation, correlation with clinical localisation was only present in 62% of the cases.
Comparison between clinical classification of vestibular dysfunction and MRI lesion site. Agreement was calculated considering those cats (55) with visible lesions on MRI, was 95% (52/55). Kappa=0.49 (95% CI 0.35–0.63).

Regarding clinical localisation, in this study, one cat with neurological signs of CVD had a focal thalamic lesion on MRI and no other MRI abnormalities explaining the vestibular signs. The hypothesis that the thalamus is involved in vestibular control has recently been suggested. In both dogs and humans, some case reports of forebrain diseases causing vestibular signs have allowed the identification of thalamic areas which may function as a relay station for vestibular input to the cortex. 23–25 In this study, however, primary thalamic lesions were not considered as part of the vestibular system.
The results of this study suggest a most equal distribution between cats showing clinical signs compatible with a peripheral vestibular condition and cats with a central vestibular disorder. The most frequent causes of CVD were respectively inflammatory (45%), neoplastic (28%) and vascular (10%), while in cats with clinical peripheral vestibular signs, idiopathic conditions and otitis media/interna were equally represented (43%). Most of the cats (69%) affected by presumed IVS showed progressive clinical signs, which has not been typical in previous reports and as such a diagnosis of atypical IVS was made. Percentage of MRI agreement with the clinical localisation of lesion was higher in PVD (94.6%) than CVD (82.5%) underlining the difficulties in detecting early or mild intracranial lesions through the neurological examination, especially in subtle forms of otogenic intracranial infections. No correlation between age and specific diseases, such as FIP and otitis media/interna, were observed in this study, which could have helped to more accurately predict differential diagnoses.
In the present study, MRI was very useful in the diagnosis of both peripheral and central vestibular disease. Ideally, specific MRI sequences, including FLAIR and T2* should be routinely performed to increase MRI sensitivity for inflammatory, vascular and infiltrative neoplastic (lymphoma) diseases. Prognosis appears to be directly associated with site (intracranial vs extracranial) rather than the nature of lesion and MRI in this study was also instrumental in the early detection of intracranial extension otogenic infection. MRI did not, however, detect abnormalities in three cats with clinical signs of intracranial disease confirmed at necropsy.
Footnotes
Acknowledgments
We thank Ms Julia Freeman for her technical support.