
Abstract
The analgesic efficacy of tramadol and/or vedaprofen was evaluated in cats submitted for elective ovariohysterectomy, using a randomised double blind placebo controlled design. Forty adult female cats (3.0±0.32 kg; 1.8±0.7 years) were distributed into four groups. Vedaprofen PO (0.5 mg/kg), tramadol SC (2 mg/kg), both, or placebo was administered 1 h before surgery and every 24 and 8 h, respectively, for 72 h after surgery. Pain score evaluated by interactive visual analogue and composite pain score and hyperalgesia by the von Frey filament test were recorded at 1, 2, 4, 6, 8, 12, 24, 28, 32, 48, 52, 56, 72, 96 h and on the 7th day after surgery. Animals treated with combined vedaprofen and tramadol treatment did not need rescue analgesia, did not develop hyperalgesia, and their serum cortisol concentrations and pain scores were lower than placebo until 24 and 72 h after surgery, respectively. Combined vedaprofen and tramadol treatment provided more effective postoperative analgesia and prevented hyperalgesia than when used on their own. Multimodal technique is a superior method of treating pain after feline ovariohysterectomy. This work also provides evidence for the benefits of analgesia for up to 3 days following ovariohysterectomy.
Preventive analgesia impedes the development of central and peripheral sensitisation caused by incisional and inflammatory injuries. 1 Although the multimodal technique maximises analgesic efficacy, 2 most of the clinical pain studies in cats have investigated a single administration of an analgesic drug before 3–5 or after 6–9 surgery, or comparing pre- and postoperative treatment. 10,11 Few studies have looked at prolonged postoperative analgesic treatment. 12,13
Vedaprofen is a preferential cyclo-oxygenase-2 non-steroidal anti-inflammatory drug (NSAID) inhibitor in dogs. 14 It is an effective anti-inflammatory and analgesic in this species for treating musculoskeletal pain. 15,16 Although it has not been approved for use in cats, some studies have already evaluated its efficacy in this species. 13,17
Tramadol is a central analgesic with a dual mechanism of effect resulting from two enantiomers which form a racemic therapeutic mixture. 18,19 Dextro-tramadol inhibits serotonin reuptake 20 and is also responsible for opioid action, produced the metabolite O-desmethyltramadol or M1 (+). 19 Levo-tramadol inhibits noradrenaline reuptake, 20 acts indirectly on postsynaptic α2 adrenoreceptors. 21
The aim of this study was to evaluate the analgesic efficacy of vedaprofen and/or tramadol in treating pain after elective ovariohysterectomy in cats. The benefit of postoperative analgesia to prevent sensitisation from the inflammatory phase was investigated. As vedaprofen and tramadol have different action mechanisms, it was hypothesised that their association would result in better analgesic efficacy with significant reductions in pain score, the need for rescue analgesia, and serum cortisol concentrations compared to independent use or placebo.
Materials and Methods
This study was approved by the animal owners and the Institutional Animal Research Ethics Committee under protocol number of 123/2003. Forty mixed breed cats were used (1.8±0.7 years; 3.0±0.32 kg). They were docile, not pregnant, and considered healthy by physical examination and haematological, hepatic and renal function tests.
Cats were randomly and equally distributed into four groups: V, T, VT and P. Vedaprofen (Quadrisol; Intervet) at 0.5 mg/kg (V and VT) or the same volume of placebo gel (T and P) were administered orally using a 1 ml syringe 1 h before anaesthesia induction and 24 and 48 h after first treatment. Tramadol (Tramadon; Cristália) at 2 mg/kg, diluted in sterile saline solution to 0.3 ml (T and VT) or 0.3 ml sterile saline solution (V and P) were administered subcutaneously 1 h before anaesthesia induction and every 8 h up to 72 h after surgery. Drug administration and evaluations were blind.
After 60 h adaptation period and 24 h before surgery cats were anaesthetised with propofol (Propovan; Cristália) (8 mg/kg, IV) for insertion of a 20-gauge catheter into the jugular vein for later drug administration and blood sampling. For surgery, anaesthesia was induced with propofol (8 mg/kg, IV), and 10 ml/kg/h of lactated Ringers solution were administered. Anaesthesia was maintained by isoflurane (Isoforine; Cristália) 1.8%±0.35 expired (Datex Engstrom AS/3) in 100% oxygen (500 ml/kg/min) using a non-rebreathing system. Animals underwent ovariohysterectomy through midline incision performed by the same experienced surgeon.
Animal pain score was evaluated preoperatively (2, 12, and 24 h) and postoperatively (1, 2, 4, 6, 8, 12, 24, 28, 32, 48, 52, 56, 72, 96 h, and on the 7th day). A visual interactive analogue scale (IVAS) was used consisting of a 100 mm line where the extreme left (=0) represented an animal without signs of pain, and the extreme right (=100) maximum pain, and an composite pain score (CPS) was developed from small animal pain evaluation scales described in the literature and using behaviours suggested as indicative of pain in cats (Table 1). 22–26 The external signs were observed, followed by the respiratory rate monitored by observing thoracic expansion, heart rate (HR) and systolic arterial blood pressure (SABP) measured using Doppler ultrasonic (Model 811-B, Parks Medical Electronics) with a sensor placed on the metacarpal artery on the medial face of the front leg, and rectal temperature by digital thermometer recorded in this order. The cats were then encouraged to move around the environment and interact with the researcher. After returning the cat to its cage, abdominal, flank and surgical wound palpation was performed. Appetite was evaluated by CPS and by measuring dry and moist food consumption from 60 h before surgery to the 7th day after surgery. Body weight was also monitored before and 7 days after surgery.
CPS used to assess severity of pain in cats undergoing ovariohysterectomy


The maximum possible score (greatest pain) was 34. Additional analgesics were given to cats scoring 11 or more.
Animals scoring 11 or higher on the CPS (33% of total score) received rescue analgesia with morphine (Dimorf; Cristália) IM at 0.5 mg/kg. Morphine rescued cats were re-evaluated 3 and 6 h later, and then returned to their regular evaluation schedule. When the rescue limit of CPS was achieved due to increased body temperature and/or pupil dilation, rescue analgesia was not performed, because opioids may produce hyperthermia and mydriasis, and pain scores might have been overestimated.
Mechanical nociceptive thresholds were determined 2 h before surgery and at the same times as postoperative score pain except for 2 and 6 h. It was determined by calibrated von Frey filaments (Semmes–Weinstein monofilaments) with progressively ascending force (0.5; 2.0; 20.0; 39.0; 98.0 mN), used in postoperative pain models in rats 27 and dogs. 28 Cats were evaluated when lying down, after leg abduction to expose the surgical wound. Each nylon filament was applied perpendicularly to the surface of the skin until it began to bend, at six different lateral points 1 to 3 mm from the wound. A positive response was defined by a strong movement, vocalisation, or attempt to bite. The threshold was indicated by a positive response from at least two of the points evaluated. If there was no response, the next size filament was used, and so on, until the last filament. The mechanical nociceptive threshold was determined considering the filament prior to the one producing a positive response. 28 Hyperalgesia was indicated by decreased thresholds relative to baseline.
Serum cortisol concentration was measured before surgery and anaesthesia, during surgery (between clipping first and second ovarian pedicle), and 1, 4, 8, 24, and 48 h after surgery. Blood samples (1 ml) were collected by jugular catheter and centrifuged for 10 min at 3000 rpm. Resulting serum was stored and frozen at −20°C until analysis using solid phase radioimmunoassay (Coat-A-Count Cortisol; Diagnostic Products).
Parametric data were analysed by repeated measures two-way analysis of variance (ANOVA) with multiple comparisons by the Tukey test, or Bonferroni correction. Data were recorded as means and standard deviations. Pain scores and mechanical nociceptive thresholds were evaluated by non-parametric analysis of variance for two factors (group and time) and repeated measurements with respective multiple comparison tests, 29 and results were presented as medians and semi-ranges. Spearman coefficient was used to evaluate correlation between pain scores, cortisol concentration, and physiological variables. The total number of analgesia rescues was analysed by the Kruskal–Wallis test according to Dunn. Significance level was considered as 5% (P<0.05). Analyses were performed using SigmaStat (Version 3.1; Systat Software). To perform statistical analysis at times when animals were not evaluated due to rescue analgesia design, values were calculated by averaging the value before and after those times.
Results
Mean anaesthesia duration and surgery time were 36±18 and 22±6 min, respectively. There were no significant differences among the groups in terms of preoperative body weight, age, intervals between administering analgesic and the induction of anaesthesia and the beginning of surgery, and the duration of surgery and anaesthesia.
Pain scores higher than the pre-surgical value were seen in VT and T up to 4 h, in V up to 32 h, and in P up to 32 and 56 h postoperatively by CPS and IVAS evaluation, respectively. Pain scores in P were higher than T 1 h after surgery and than VT from 1 to 72 h after surgery. Pain scores in V were higher than T 1 h after surgery, and higher than VT 1 to 56 h after surgery (Figs 1 and 2).

Interactive visual analogue scale pain scores (median and semi-range) for cats undergoing ovariohysterectomy and treated with tramadol (n=10) or vedaprofen (n=10) or vedaprofen and tramadol combination (n=10) or placebo (n=10). Basal value – preoperative assessment mean (2, 12 and 24 h). Significant differences among groups are indicated by the presence of letters, where the value of ‘a’ is greater than ‘b’ which is greater than ‘c’.
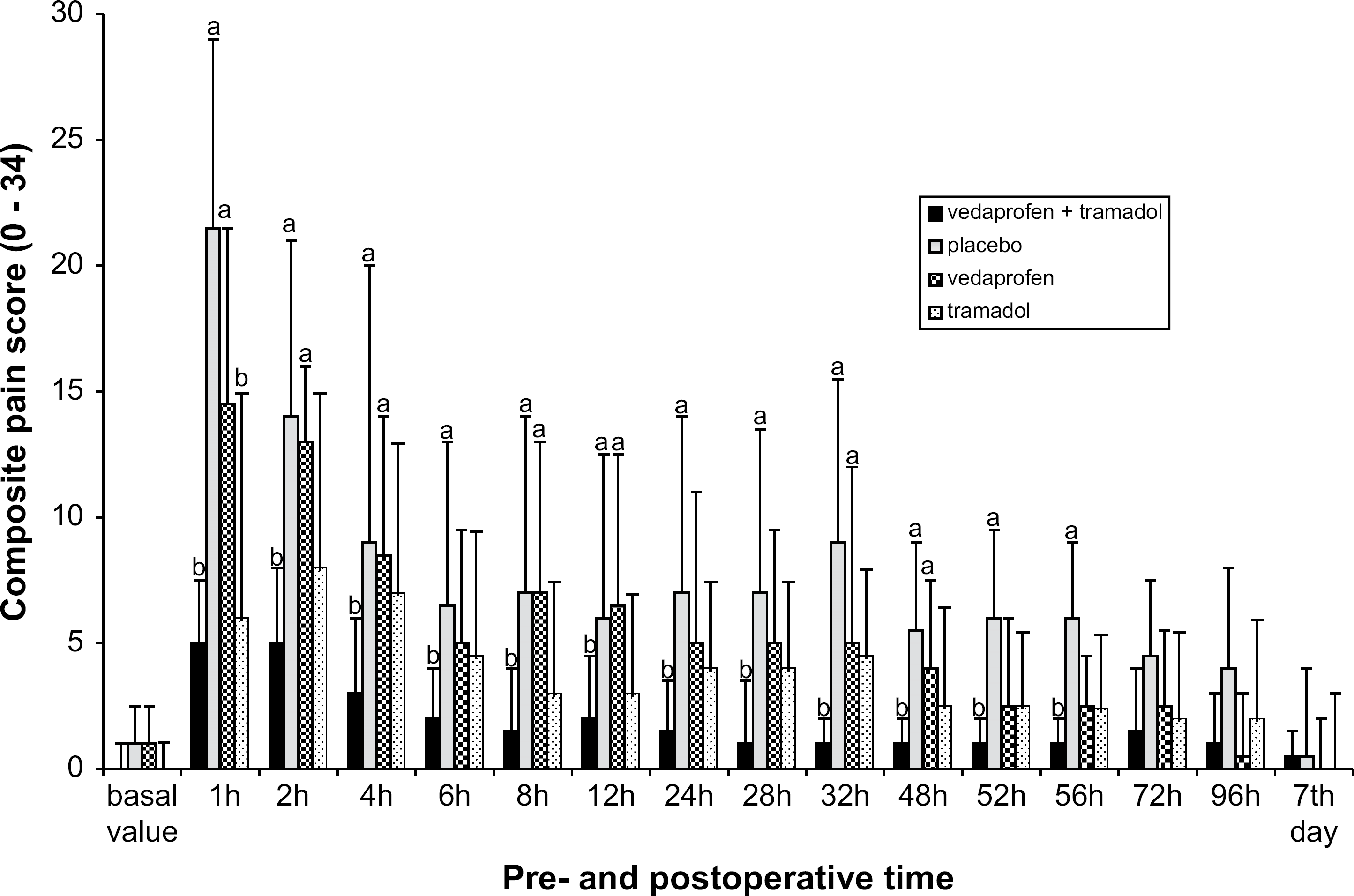
CPS (median and semi-range) for cats undergoing ovariohysterectomy and treated with tramadol (n=10) or vedaprofen (n=10) or vedaprofen and tramadol combination (n=10) or placebo (n=10). Basal value – preoperative assessment mean (2, 12 and 24 h). Significant differences among groups are indicated by the presence of letters, where the value of ‘a’ is greater than ‘b’.
Mechanical nociceptive threshold was significantly reduced 1 h after surgery in P and 1, 4, and 32 h after surgery in V, thresholds did not reduce in VT and T. P presented lower mechanical nociceptive threshold than VT and T up to 4 h after surgery. V presented lower mechanical nociceptive threshold than T up to 4 h after surgery, and than VT up to 32 h after surgery (Table 2).
Mechanical nociceptive threshold (median±semi-range, mN) for cats undergoing ovariohysterectomy and treated with tramadol (T: n=10) or vedaprofen (V: n=10) or vedaprofen and tramadol combination (VT: n=10) or placebo (P: n=10)

Significant differences among groups are indicated by the presence of letters, where the value of ‘a’ is greater than ‘b’.
Significant differences compared with pre-surgical values.
Increased serum cortisol levels compared to before surgery were seen 1 and 4 h after surgery in P and 1 h after surgery in V and T. Cortisol in P was higher than V at 4 h, than T at 1 and 4 h, and higher than VT from 1 to 24 h after surgery. During surgery cortisol was higher in V than VT and T (Fig 3).

Serum cortisol concentration (mean±SD; nmol/l) for cats undergoing ovariohysterectomy and treated with tramadol (n=10) or vedaprofen (n=10) or vedaprofen and tramadol combination (n=10) or placebo (n=10). Significant differences among groups are indicated by the presence of letters, where the value of ‘a’ is greater than ‘b’ which is greater than ‘c’. * Significant differences compared with pre-surgical value.
SABP increased over basal value 1 h after surgery in T and VT, and 1 and 2 h after surgery in P and V. One hour after surgery the SABP in P (169±16 mmHg) and V (168±19 mmHg) was higher than VT (149±24 mmHg) and T (148±20 mmHg). HR was higher at 1 and 2 h after surgery compared to base value in all groups. HR in VT 2 h before (187±20 beats/min) and 72 h after surgery (201±27 beats/min) were higher than P (158±20 beats/min; 171±25 beats/min). Respiratory rate was not significantly different among groups.
Temperature was higher than basal values from 2 to 8 h after surgery in VT, from 2 to 12 h in T, and from 4 to 12 h in P and V. Postoperative maximum temperature was 39.4±0.6°C at 4 h in VT, 39.4±0.4°C at 6 h in T, 39.0±0.6°C at 6 h in P and 39.2±0.4°C at 8 h in V. Temperature was higher in T (38.9±0.4°C) and VT (39.0±0.8) than P (38.4±0.6°C) at 2 h after surgery.
There was strong correlation between CPS and IVAS scores (r=0.955; P=0.000), moderate correlation between CPS/IVAS and cortisol (r=0.424 and 0.423 respectively; P=0.000), and weak correlation between CPS/IVAS and SABP (r=0.307 and 0.315 respectively; P=0.000). Cortisol had moderate correlation with SABP (r=0.405; P=0.000). Heart and respiratory rates and T did not correlate significantly with the other variables.
Rescue analgesia was administered to all P and V animals, and 50% of T animals. No VT animal needed rescue analgesia (Table 3).
Number of rescue analgesia (morphine) after ovariohysterectomy and the timing of the intervention

Significant differences among groups in the total number of rescue analgesia indicated by the presence of letters, where the value of ‘a’ is greater than ‘b’ which is greater than ‘c’.
Total moist food consumption in the postoperative period was significantly lower in P (720±93.8 g) compared to V (927±142.2 g), T (924±168.4 g), and VT (918±197.5 g). Dry food consumption in the first 12 h after surgery was significantly lower in P (19.5±10.1 g) than VT (45.0±14 g), T (40.5±17.4 g), and V (36.0±19 g). Unlike P, treated groups showed significant weight gain 7 days after surgery compared to before surgery. Mean weight gains were 120±113 g (VT), 110±99 g (V and T), and 40±69 g (P).
Discussion
Using vedaprofen in association with tramadol, compared to their independent use, produced lower cortisol concentrations and pain scores than placebo up to 24 and 72 h after surgery, respectively, without the need for rescue analgesia. This demonstrates that preventive multimodal analgesic treatment is more effective than individual drug use in controlling acute pain after ovariohysterectomy in cats and that a good way to approach preventive analgesia is to administer combined analgesics which have action on different nociceptive sites for a prolonged period after surgery. 30,31 NSAIDs inhibit peripheral and central nervous system prostaglandin synthesis, 32 and tramadol as well as presenting opioid action sites, activates the central monoaminergic inhibitory system. 18 The increased analgesic efficacy of tramadol associated with NSAIDs has already been described in man. 19 This association apparently produces a satisfactory nociceptive block, minimising the stress related to anaesthesia and surgery. 33 Additionally, only the combination of these drugs prevented hyperalgesia; recommending the multimodal technique for preventing central and peripheral sensitisation. 31,34
Regarding the ethical implications of including a placebo group, to evaluate the clinical benefits of preventive analgesia versus no treatment, 35 a rigid design of analgesic intervention was adopted using the highest dose of morphine recommended in literature for this species 36 and low pain score for rescue analgesic. This protocol was adopted because pain evaluation in cats may be underestimated due to their reserved behaviour and the use of subjective non-validated scales. This procedure differs from studies which adopted animal discomfort, 3,8,9 or point scales for pain (IVAS or CPS) at about 50% of the total. 4,5,7,10,11 It was presumed that a subjective criteria or high score for rescue analgesia would not benefit all animals with pain, especially those manifesting discomfort from subtle changes which do not cause a significant increase in score. As P animals needed significantly more rescue analgesia than T and VT, the CPS for analgesic intervention was considered a sensitive guide for identifying pain after ovariohysterectomy in cats. The presence of body temperature and pupil diameter items in CPS can lead to overestimated pain scores when opioids are used in cats, so rescue analgesia was not administered in animals which reached the score limit due to changes in these variables.
Due to the prolonged postoperative evaluation time and regular administration of drugs during this period, evaluations after rescue analgesia were included in the study; this is not a routine procedure, 4,5,9,11 because it can compromise the significance of statistical analysis. However, it was assumed that after the development of peripheral or central sensitisation, rescue with morphine had a limited effectiveness. 37 Placebo group animals had significantly higher pain scores than basal at 32 and 56 h after surgery by CPS and IVAS, respectively. Additionally, there was a significant difference between placebo and drug combination groups at 56 and 72 h after surgery by CPS and IVAS, respectively. According to the results ideally analgesia should continue for 56 to 72 h after ovariohysterectomy in cats.
The interaction between animal and researcher and the prior knowledge of each animal's specific behaviour were indispensible for adequately evaluating pain. Signs suggesting pain in cats were confirmed; these were squinted eyes, licking or biting the wound area, 38,39 and frequently changing position or reluctance to move. 40 Behaviour like retracting and extending the rear paws and tail wagging were also linked to postoperative pain. Response to pain after wound palpation was greater, as shown by vocalisation and attempts to bite, in P animals, followed by V, T and VT. This confirms that surgical wound palpation is important in pain evaluation. 41,42 The low food consumption and less weight gain in P compared to the treated groups, agrees that reduced food ingestion is related to postoperative pain. 40,43
The higher cortisol concentrations in P when compared to treated groups confirms previous studies. 12,26,44 The moderate correlation between cortisol and pain score, as reported after orthopaedic surgery in cats, 45 suggests that cortisol is a good indicator of postoperative pain, providing that an adaptation period is performed to acclimatise the animals.
Conflicting results have been reported for SABP as a pain indicator in cats, 44–46 SABP moderately correlated with cortisol concentration, as observed before, 44 but correlation with pain scores was weak. Rescue analgesia with morphine is presumed to reduce SABP and might influence statistical significance. The importance of SABP in evaluation pain in cats is still unclear. On the other hand, heart and respiratory rates do not correlate with postoperative pain in cats as observed elsewhere. 44–47 Body temperature was increased by the use of tramadol in T and VT and after rescue analgesia with morphine in P and V. Cats are susceptible to developing hyperthermia after receiving μ opioid agonists, 38 even after clinical doses. 48–50
Isolated vedaprofen use did not produce effective preventive analgesia. Contrary to our results, previous studies showed the isolated use of vedaprofen or other NSAIDs was considered effective in controlling pain after ovariohysterectomy in cats. 3–8,10,11,13,17 In our study, the cats were acclimatised to the environment and according to that they might have exhibited more signs of pain than cats in previous studies. As there are still no reports evaluating the pharmacokinetics of vedaprofen in cats, this was administered orally approximately 1 h before surgery, because maximum plasma concentration was reached within this period in a study on dogs. 51 This period, however, may have been insufficient to allow an adequate concentration to build up in target tissues during and immediately after surgery. Slow absorption or late starting action due to oral administration has already been suggested by the negative effect of NSAIDs on cortisol block in cats. 5
Otherwise the lack of effectiveness of isolated vedaprofen might not be due to inadequate concentrations, but because the analgesic effects of NSAIDs when used as primary analgesics for acute postoperative pain is modest. 32 The design of previous studies, which included the use of sedatives such as acepromazine, 3–8,10,11 anaesthetics with an analgesic effect, such as ketamine, 4,5,11 high threshold for rescue analgesia, 4,5,7,10,11 subjective criteria, 3,8 or not using rescue analgesia, 6,13 associated to the inherent difficulties in evaluating pain in cats, could have overestimated the effectiveness of NSAIDs as unique analgesics in ovariohysterectomy in cats. The skill of the surgeon and duration of surgery can also affect the level of expected pain, however, in this study the surgeon was experienced and surgery time was short. The animals treated with vedaprofen received less rescue analgesia than placebo group after 8 h postoperative. This might have produced a major variability of mechanical nociceptive threshold in the former group.
The better analgesia produced by tramadol in this study when compared to P is a different finding to those presented for the antinociceptive evaluation of tramadol in cats. 52 However, in the previous study 52 a local nociceptive stimulus and only 1 mg/kg tramadol dose was used which might explain the conflicting results. Studies in man show that analgesia from tramadol has a significant dose response effect, 53 but no such studies have yet been performed in cats.
Of the five animals in the T group needing rescue analgesia, three were on the threshold (12 points) and two had elevated pain scores (15 and 20 points). One should consider that if a 50% analgesic threshold had been used, only one animal would have received rescue analgesia, cats with pain would have been deprived analgesia and the drug's effectiveness overestimated. The two animals from T with high pain scores also had hyperalgesia and high cortisol levels, which differentiated them from the rest of the group. Perhaps this less effective response to tramadol was not just related to its isolated use, but due to interindividual variability in tramadol's analgesic efficacy. An individual cat's response to opioids is extremely variable and genetically determined. 38,41,54,55
Tramadol O-demethylation to form M1 (+) metabolite is dependent on sparteine oxygenase (CYP2D6). 56 The genetic interethnic polymorphism of this enzyme has been well documented in man. 57 Poor metabolisers individuals have low M1 (+) concentrations and a reduced analgesic effect from tramadol. 58 Despite cats having a lower M1 (+) formation rate than dogs, low metabolic clearance of tramadol in cats allows higher M1 (+) concentrations in this species. 59 Additionally, M1 (+) could be the main tramadol metabolite in cats, 59 different from dogs. 60 As in man, cats might also be subject to interindividual variability in M1 (+) production. Our results highlight that as with any other opioid in cats, analgesia with tramadol must be monitored and if necessary, the dose and/or the administration interval should be individually adjusted, as well as thinking about rescue analgesia with another drug.
In conclusion, combined administration of vedaprofen and tramadol before surgery and regularly for up to 72 h after surgery prevents hyperalgesia and results in lower cortisol concentrations, pain scores, and less need of rescue analgesia than using isolated drugs. The clinical benefits of preventive analgesia were demonstrated, as well as the advantages of the multimodal technique in controlling pain after ovariohysterectomy in cats. Analgesia should also be provided after ovariohysterectomy for a minimum of 72 h.
Footnotes
Acknowledgements
This research was supported by the National Council of Technological and Scientific Development (CNPq). The authors thank Masterfoods South America (Effem Brazil) for supplying cat food.