
Abstract
The records of 204 cats entering the intensive care unit (ICU) at the University of Edinburgh Small Animal Hospital between December 2002 and October 2006 were retrospectively analysed. Of these, 37 cats over 12 months of age had a systolic blood pressure recorded on entry into the ICU, and this group comprised our study population. Of these 37 cats, 36 had both heart rate and respiratory rate recorded on entry into the ICU, whilst 24 of these cats also had body temperature recorded. The relationship between (i) survival to discharge and (ii) survival until 21 days after admission to the ICU was analysed using univariate generalised linear models with binomial errors. The robustness of any significant relationship was assessed using multivariate analysis methods. In addition, receiver operator curves (ROC) were generated for any of the significant predictors of mortality and from these curves the threshold values, optimal sensitivity and specificity were calculated. Using these values survival curves were generated for any significant prognostic indexes. A decreased blood pressure at the time of admission to the ICU was found to be a significant negative predictor of survival until discharge from the hospital. Overall, a systolic blood pressure of 124 mmHg or higher at the time of admission to the ICU has a sensitivity of 47.8% and a specificity of 85.7% for predicting that a cat will survive until discharge from the hospital.
In human beings different prognostic indexes have been developed for the assessment of a patient's disease severity and to predict their likely mortality while in intensive care. The application of such indexes aims at identifying patients with a higher recovery potential. Several such indexes exist, including the Acute Physiology and Chronic Health Evaluation (Knaus et al 1985) and Simplified Acute Physiology Score models (Kvåle and Flaatten 2002). These indexes have highlighted the importance of systolic blood pressure, heart rate, respiratory rate and body temperature in predicting the short term outcome after admission to an ICU (Kellett and Deane 2006). In addition, it has been demonstrated that, in people, blood pressure can act as both a short and medium term predictor of outcome (Low et al 1993, Jones et al 2004, 2006, Kellett and Deane 2006). The poor short and medium term outcomes associated with hypotension, bradycardia, hypothermia and respiratory failure are proposed to occur in conjunction with circulatory failure. Untreated this can result in inadequate tissue perfusion, decreased oxygen supply to cells and eventual organ dysfunction.
Such prognostic indicators have not been studied extensively in small animals. In one study by Toll et al (2002) it was found that the survival to discharge of hospitalised cats with abnormal total serum magnesium levels was significantly decreased compared to cats with normomagnesaemia. Canine studies have demonstrated that a survival prediction index, incorporating measurements of mean arterial pressure, respiratory rate, creatinine, packed cell volume, albumin, age and medical versus surgical status, could objectively stratify ICU patients according to the severity of disease (King et al 2001) and outcome (Prittie et al 2002). Research on dogs that had undergone extrahepatic biliary surgery found that the lowest postoperative blood pressures were significantly lower in the dogs that did not survive compared to surviving dogs (Mehler et al 2004).
We hypothesised that systolic blood pressure, heart rate, respiratory rate and body temperature could act as predictors of mortality in critically ill cats.
Materials and methods
The records of all cats entering the intensive care unit (ICU) at the University of Edinburgh Small Animal Hospital, between December 2002 and October 2006, were retrospectively analysed. The study population comprised only the adult cats (>1 year of age) that had a systolic blood pressure recorded on entry into the ICU. The systolic blood pressure was measured using an indirect Doppler flow-meter (Parks Electronic Doppler Flow-meter; model B-811, Perimed, Bury St Edmunds, UK) in accordance with guidelines set out by with the hypertension consensus panel (Stepien 2004).
The cat's signalment, respiratory rate, heart rate and body temperature at the time of entry into ICU were also recorded. Whenever possible, the primary diagnosis was recorded.
The length of time until discharge from the hospital was recorded in all cats that survived. In those that died or were euthanased, the time until death was recorded. In addition, the number of cats surviving for 21 days from the time of admission to the ICU was recorded. The primary outcome was determined as cats that survived until discharge from the hospital, the secondary outcome was determined as cats that were still alive at 21 days post-admission to the ICU.
Statistical analysis
The relationship between (i) survival to discharge and (ii) survival until 21 days after admission to the ICU, and four putative prognostic predictors (systolic blood pressure, body temperature, heart rate or respiratory rate) was analysed using univariate generalised linear models with binomial errors. Statistical significance was set at a value of P < 0.05. If any of the four parameters were significant then additional multivariate analyses were carried out to test whether the observed difference was still present after the influence of the other three parameters had been taken into account first within the statistical model.
Preliminary analyses indicated that the most common condition observed in the study population was a diagnosis of cardiac disease. Therefore, whether the cats in the study population had this condition was included in a multivariate statistical model to investigate whether or not the presence of cardiac disease had a significant confounding effect on any of the four predictors of survival that had been established above. Likewise, age and gender were included in the model in order to assess any significant confounding effects.
Receiver operator curves (ROC) were generated for any of the significant four potential predictors of mortality and from these curves the threshold value for optimal sensitivity and specificity was calculated. Using these established threshold values, Kaplan–Meier survival plots were generated for any significant prognostic indicators. Cox-proportion hazard models were used to test the significance of any differences in survival curves. Survival analysis excludes all cases once they were discharged from the hospital, irrespective of outcome. Therefore, cats discharged soon after admission to the ICU were ‘lost to follow-up’ at least in terms of this analysis. The statistical analysis was carried out using R (R version 2.4.1 copyright 2006 The R Foundation for Statistical Computing) and S-Plus Statistical analysis packages (S-Plus version 6.2.1, 1988, 2003 Insightful Corp. S: Copyright Lucent Technologies, Inc.)
Results
Our records demonstrated that a total 204 cats had entered the ICU between December 2002 and October 2006. Of these, 37 cats over the age of 12 months had a systolic blood pressure recorded on entry into the ICU. This group comprised our study population; 36 cats of these cats had both heart rate and respiratory rate recorded on entry into the ICU, whilst 24 of these cats also had a body temperature recorded (Table 1).
Characteristics of cats entering the ICU
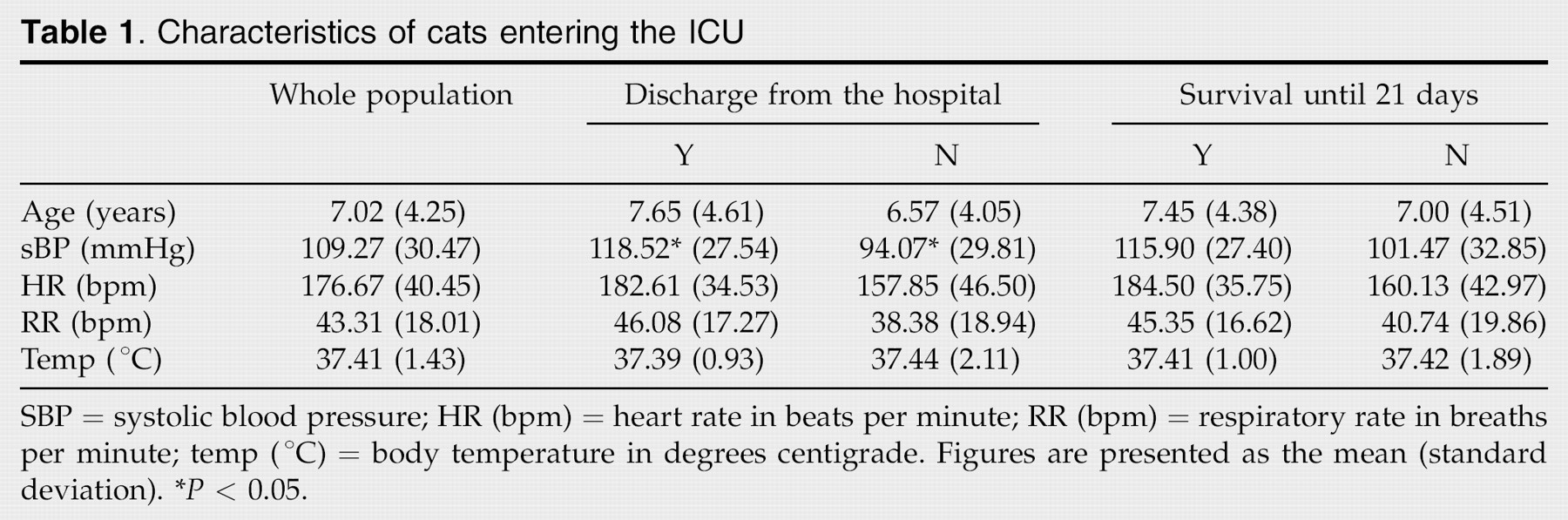
SBP = systolic blood pressure; HR (bpm) = heart rate in beats per minute; RR (bpm) = respiratory rate in breaths per minute; temp (°C) = body temperature in degrees centigrade. Figures are presented as the mean (standard deviation).
P < 0.05.
Within the study population there were seven different breeds of cat; 27 cats were domestic short- or longhair cats (DSH/DLH), three Siamese cats, two Maine Coon cats, two Persian cats, one Sphinx cat, one Devon Rex cat and one Bengal cat. The majority of the cats were neutered; the group comprised 23 male neutered cats, 13 female neutered cats and one entire female cat. A variety of conditions were represented; the presenting complaint/diagnosis was that of a cardiac disorder (n = 14), followed by trauma (n = 6; two of these cats had concomitant cardiac disease), renal failure (n = 4), neoplasia (n = 4), seizure (n = 2), pneumonia (n = 2), hepatopathy (n = 2), anaemia (n = 2), pancreatitis (n = 1), septic peritonitis (n = 1), and duodenal obstruction with concurrent seizure activity (n = 1). None of the cats had had surgery prior to the measurement of the systolic blood pressure. Of the 14 cats admitted for cardiac diseases, 10 were male and four were female.
Twenty-three of the cats were discharged from the hospital, the remaining 14 were either euthanased or died whilst hospitalised. The mean duration of hospitalisation, for all cats, was 5.86 days (range 0.25–17 days). The respiratory rate and body temperature were not significantly different in cats that survived hospitalisation, compared to those that died or were euthanased in the hospital. The heart rate at the time of admission to the ICU tended to be higher in the cats that survived until discharge from the hospital, however, this did not reach statistical significance (P = 0.07). The systolic blood pressure at the time of admission to the ICU was significantly lower in those cats that died prior to discharge from the hospital (P = 0.013).
The remaining putative predictors were then built into the model to assess whether or not the relationship between systolic blood pressure and survival was confounded by any of the other variables. These variables did not have any significant effect on the relationship between blood pressure and survival.
The age and gender were then built into the model in order to assess whether or not the signalment of the cats imposed a significant effect on the relationship between the systolic blood pressure and the outcome (discharge from the hospital). Neither age nor gender significantly altered the relationship between systolic blood pressure and discharge from the hospital.
The majority of the cases included in this study were suffering from cardiac complaints. Therefore, a diagnosis of cardiac disease was included in another model to assess whether or not the relationship between the systolic blood pressure and discharge from the hospital was different in the cats with cardiac disease compared to those with non-cardiac disease. It was found that a diagnosis of cardiac disease did not alter the relationship between the systolic blood pressure and survival to discharge from the hospital.
ROCs were generated in order to examine the trade-off between sensitivity and specificity when systolic blood pressure at the time of entry into the ICU was used as a predictor of survival to discharge from the hospital. From this it was calculated that a cut-off of 124 mmHg or greater predicted survival to discharge with a sensitivity of 47.8% and a specificity of 85.7%. The area under the curve (AUC) was 0.71.
Using the cut-off of 124 mmHg generated from the ROC curves, a survival curve for cats surviving until discharge from the hospital was generated (Fig 1). The survival of cats with systolic blood pressure equal to or greater than 124 mmHg tended to be greater than that of cats with a systolic blood pressure of less than 124 mmHg, however, this did not reach statistical significance (P = 0.06). Of the 23 cats that were discharged from the hospital, 20 were still alive at 21 days; with the three remaining cats dying at 2 days, 5 days and 20 days after admission to the ICU. The heart rate, respiratory rate, body temperature and systolic blood pressure at the time of entry into the ICU were not significantly different in those cats surviving until 21 days post-admission to the ICU compared to those that did not survive.

Cox-proportion hazard model of survival until discharge from the hospital in cats with systolic blood pressure of greater then 124 mmHg compared to cats with a systolic blood pressure of less than 124 mmHg.
Discussion
This study demonstrates that cats with a decreased systolic blood pressure at the time of entry into the ICU were less likely to survive until discharge from the hospital compared to cats with higher systolic blood pressures. This relationship was not altered significantly by the effects of heart rate, respiratory rate, body temperature, signalment (assessed by the age and gender of the cat) or the presence of cardiac disease. Heart rate, respiratory rate and body temperature were not significantly different in the cats that survived until discharge, compared to those that died or were euthanased within the hospital. Although the heart rate at the time of admission to the ICU tended to be higher in the cats that survived until discharge from the hospital, this did not reach statistical significance. Interestingly, none of the putative predictors were significantly different in the cats that survived until 21 days post-admission to the ICU compared to those that did not survive.
The human literature contains several reports of prognostic indicators for a favourable outcome after admission to the ICU (Knaus et al 1985, Kvåle and Flaatten 2002, Kellett and Deane 2006). Amongst these, one of the strongest indicators of survival is systolic blood pressure (Jones et al 2006). However, whilst it is generally accepted that some sick cats will demonstrate a decreased blood pressure, to the authors’ knowledge, this is the first report of systolic blood pressure serving as a significant prognostic indicator in this species. Other potential predictors (heart rate, respiratory rate and body temperature) were not found to be significantly different in cats that were discharged from the hospital compared to those that did not survive until discharge.
An ROC was generated to assess the trade-off between the sensitivity and specificity of systolic blood pressure as a predictor of survival to discharge. The AUC was 0.71, suggesting that blood pressure is a fair predictor of survival. This curve demonstrated that a blood pressure of 124 mmHg predicted survival with a sensitivity of 47.8% and a specificity of 85.7%. This cut-off was chosen in order to optimise specificity, whilst maintaining an adequate sensitivity. Interestingly, it has previously been reported that the lower end of the ‘reference range’ for feline systolic blood pressure is 120 mmHg (Stepien 2004). Therefore, our findings would suggest that cats diagnosed as hypotensive at the time of entry into the ICU are less likely to be successfully discharged from the hospital. Whilst the sensitivity of this predictor was not high, there were multiple treatments instigated after admission to the ICU, and this will impact this statistic. When assessing a prognostic indicator of mortality the specificity is clinically of use in advising owners of potential outcome. In this study, systolic blood pressure on entry into the ICU was found to predict mortality in a group of cats with various disease states, with a specificity of 85.7%. This high specificity for a single parameter indicates the importance of blood pressure in critically ill cats. Furthermore, the survival analysis curves demonstrated a marked divergence, with cats having a blood pressure of less than 124 mmHg demonstrating a decreased survival, whilst this was not statistically significant, it may be considered to be of clinical significance.
The secondary outcome (21 days post-admission to the ICU) was also investigated. All the cats that survived until discharge had been discharged from the hospital by day 17; therefore, this time point represented the outcome post discharge from the hospital. The outcome at day 21 was not predicated by any of the putative predictors. This may suggest that other factors other than the blood pressure may predict the medium term outcome in these cases. However, this study did not include any follow-up measures of blood pressure, and therefore, alterations occurring at any time point after admission to ICU were not accounted for.
Our study population comprised 37 cats, all over 1 year of age that had their systolic blood pressure recorded at the time of admission to the ICU. During the study period 204 cats were admitted to the ICU; the systolic blood pressure being measured at the time of entry into the ICU in only 1/6 of the cats. Cats that had their blood pressure recorded either before entry into ICU or those cats that had blood pressure measured after the first day of admission to the ICU were excluded from the analysis. It is unfortunate that more of the cats entering the ICU did not have their blood pressure recorded. Nevertheless, in the relatively small number of cats that were evaluated, this parameter appears to be significantly related to survival.
Study limitations
This study was performed by retrospective analysis of the records of 204 cats that entered the ICU at the University of Edinburgh Small Animal Hospital between December 2002 and October 2006. Unfortunately, not all of the cases included had all of the putative prognostic indicators recorded. Furthermore, only 18% of the cats that entered the ICU during that period fulfilled our inclusion criteria (that of being adult cats that had their systolic blood pressure measured upon admission to the ICU) and therefore, only a relatively small number of cases were included in this study. Had more cats been included in the study, the relationship between the putative prognostic indicators and survival may have been altered. In addition, the retrospective nature of this study may have introduced sampling bias to the population studied. Not all cats entering the ICU had their blood pressure measured and information pertaining to the non-sampled cats was not included in this analysis. Thus, clinicians may have selectively measured blood pressure in animals that were clinically thought likely to be hypotensive. Furthermore, whilst this study highlights the importance of assessing systolic blood pressure as a prognostic indicator after entry to the ICU, it provides no information on whether or not the prognosis could have been altered if the blood pressure was pharmacologically manipulated. In future, a large, prospective study is needed to attempt to verify the results of the current study.
Conclusions
In the cat a decreased systolic blood pressure at the time of admission to the ICU is a strong negative prognostic indicator for predicting survival to discharge. Furthermore, a systolic blood pressure of 124 mmHg at the time of admission in the ICU has a sensitivity of 47.8% and a specificity of 85.7% for predicting whether or not a cat will survive until discharge from the hospital.
Footnotes
Acknowledgments
The authors would like to thank Dr D.J. Shaw for his guidance in the preparation of this manuscript. In addition, we would like to thank all the members of the University of Edinburgh Small Animal Hospital who helped in this study.