
Abstract
Three immature cats with growth abnormalities of the distal radius secondary to trauma were presented between July 2001 and July 2003. Initial injuries included a Salter–Harris type II fracture of the distal radial physis in one cat, fractures of the styloid process of the ulna in two cats, and metacarpal fractures in one cat. The cats were between 3.5 and 4.5 months of age at the time of injury. Damage to the distal radial physis resulted in a variable degree of shortening of the radius in all cats. Asymmetrical closure caused widening of the lateral aspect of the radiocarpal joint space in two cats. Elbow incongruity was not observed. One cat was treated with osteotomies of the radius and ulna and realignment of the radius, stabilised with external skeletal fixation. Another was treated by ulnar ostectomy alone. Radius and ulna osteotomies and distraction osteogenesis of the radius were performed in the third cat. Clinical outcome was satisfactory in all three cases.
Premature physeal closure following trauma, a common and well-described condition in growing dogs, is infrequently encountered in cats. In dogs, premature closure of the distal ulnar physis is the most common cause of growth deformity (Fox 1984, Johnson and Hulse 2002, Boudrieau 2003). Premature closure of the distal radial physis is encountered less frequently and may be symmetrical or asymmetrical (Carrig 1983, Vandewater and Olmstead 1983, Fox 1984, Shields Henney and Gambardella 1990).
Symmetrical premature closure of the distal radial physis results in radial shortening associated with an enlarged humero-radial joint space in dogs (Carrig 1983, Shields Henney and Gambardella 1990). Internal rotation and varus angulation of the paw may also result from continued distal growth of the ulna (Shields Henney and Gambardella 1990). Asymmetrical closure of the distal radial physis typically involves the lateral aspect of the physis, causing valgus deformity of the distal radius (Vandewater and Olmstead 1983, Fox 1984, Shields Henney and Gambardella 1990).
Surgical options to correct growth abnormalities following premature closure of the distal radial physis depend on type and severity of the lesion, and age of the animal. In general, the aims are to restore joint congruity, correct angulation or rotational deformity of the radius, and prevent or treat radial shortening.
The clinical and radiological features of three cats with growth abnormalities of the distal radial physis are described in this report. Treatment options are discussed, and comparisons to the dog are made.
Case histories
Case 1
A 1.9 kg, 3.5-month-old, male domestic shorthair presented with a non-weight-bearing left forelimb lameness after a single storey fall. Physical examination revealed pain and swelling of the distal antebrachium. A mildly displaced Salter–Harris type II fracture (Salter and Harris 1963) of the distal radius was diagnosed (Fig 1a) and a splinted bandage applied for 18 days. At the time of splint removal, the fracture had healed, but the radial physis was narrowed and slightly deformed on the mediolateral radiograph (Fig 1b). These early signs of premature physeal closure were not appreciated then. Three months later, the cat represented with a progressive left forelimb lameness. Radiography revealed an almost complete premature closure of the distal radial growth plate with deformity of the radial epiphysis (Fig 1c and d). The radiocarpal joint space was significantly widened dorsally and laterally, valgus deformity of the distal radius was present, and the affected radius was 13 mm (15.5%) shorter compared to the opposite side (Table 1).
Age of the cats at the time of trauma and surgery, and decrease of radial length at follow-up examinations
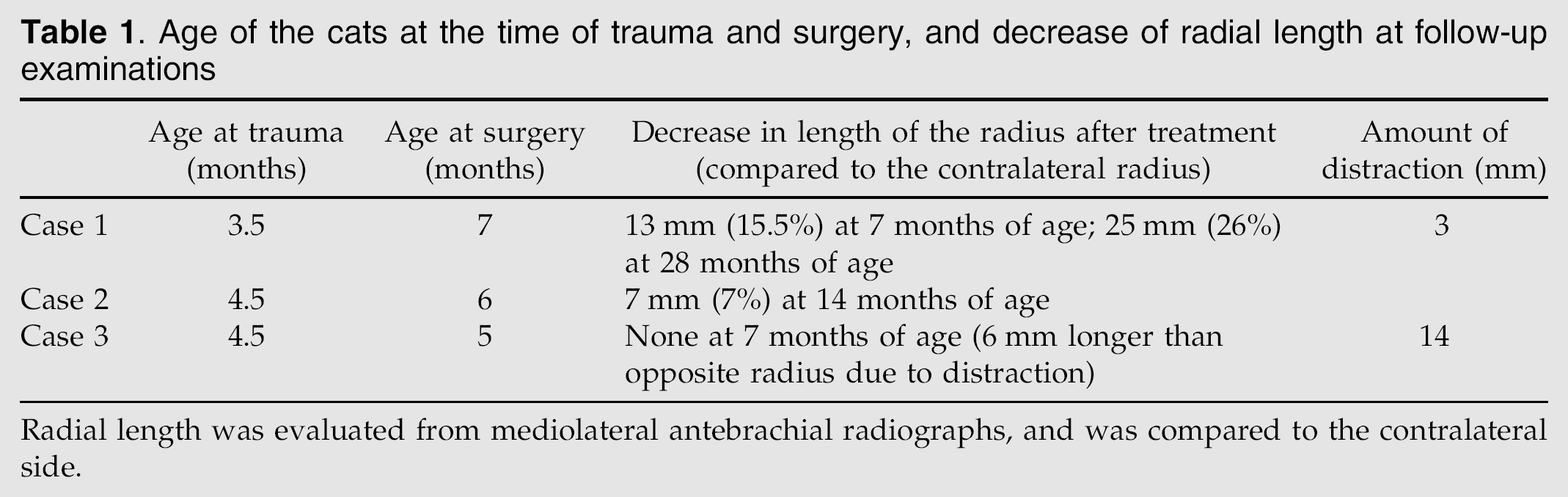
Radial length was evaluated from mediolateral antebrachial radiographs, and was compared to the contralateral side.

Pre-treatment radiographs of case 1. (a) Radiographs of the left and right carpus of the 14-week-old cat at admission. A mildly displaced Salter-Harris type II fracture of the left distal radial physis is visible. (b) Mediolateral radiographs 18 days after the injury. The fracture has healed, but the physes seem narrowed, and the distal radial physis is inclined cranioproximal to caudodistal. (c) Mediolateral radiograph 3.5 months after the initial injury. The distal radial physis is almost completely closed, the distal ulnar physis is still open. Cranial bowing of the distal ulna is evident. (d) Craniocaudal radiograph 3.5 months after the initial injury. There is significant widening of the lateral aspect of the radiocarpal joint.
A distal oblique metaphyseal radial osteotomy and a 2 mm wide transverse ulnar ostectomy were performed, and the distal radius was realigned in order to improve carpal joint congruity. The radial osteotomy site was acutely distracted 3 mm to increase radial length. A type I external fixator (Meynard external fixator, Eickemeyer, Tuttlingen, Germany) was applied to the medial aspect of the bone (Fig 2a). The osteotomies healed uneventfully and the external device was removed after 10 weeks. Final follow-up examination was performed when the cat was 28 months of age. Neither lameness nor limb deformity was noted on clinical examination, but flexion of the antebrachiocarpal joint was reduced to 50°. Degenerative changes of the carpometacarpal joint were noted radiographically (Fig 2b). The affected radius was 25 mm (26%) shorter than the contralateral unaffected side (Table 1).

Post-treatment radiographs of case 1. (a) The postoperative craniocaudal radiograph shows the appearance after radial osteotomy and ulnar ostectomy, followed by stabilisation of the radius with a type I external skeletal fixator. Realignment of the distal part of the radius improved congruity of the carpal joint. (b) The joint surfaces of the antebrachiocarpal joint are still congruent on craniocaudal radiographs taken 21 months after removal of the external fixator, but a mild medial subluxation and carpal osteoarthritis are present.
Case 2
A 2.7 kg, 4.5-month-old, male castrated domestic shorthair presented after a fall from the fourth floor. On initial examination the cat was in shock requiring cardiovascular stabilisation. Orthopaedic examination revealed crepitation and swelling in both metacarpi. Bilateral metacarpal fractures and a fracture of the left ulnar styloid process were diagnosed on radiographs (Fig 3a). The metacarpal fractures were stabilised with intramedullary pins and splinted bandages. Seven weeks later, the metacarpal fractures had healed and the pins were removed. Radiographs at this stage revealed an irregular distal radial physis of the left thoracic limb, with widening of the lateral aspect of the radiocarpal joint space, and a mild valgoid deformity of the distal radius (Fig 3b). The ulnar physis was located more distally when compared to the contralateral normal side (Fig 3c). Widening of the lateral radiocarpal joint was thought to be the result of asymmetrical lateral growth retardation, combined with continuous growth of the distal ulna.

Pre-treatment radiographs of case 2. (a) Dorsopalmar radiograph of the left foot of the 4.5-month-old cat showing metacarpal fractures, and a fracture at the distal end of the ulnar styloid process. (b) Dorsopalmar radiograph of the left foot obtained 7 weeks after the injury. A valgoid deformity of the distal radius and widening of the lateral aspect of the radiocarpal joint are visible. The distal ulnar physis is located at the level of the distal radial physis. (c) Dorsopalmar radiograph of the right foot for comparison. The carpal joint is congruent, the physes are regular, and the distal ulnar physis is located proximal to the distal radial physis.
An 8 mm wide transverse ulna ostectomy was performed proximal to the growth plate to allow the distal part of the ulna to shift proximally and to prevent further lengthening of the ulna (Fig 4a and b). At clinical re-examination 8 months after surgery the cat was walking normally, but flexion in the antebrachiocarpal joint was reduced to about 30°. Radiocarpal joint congruity was improved when compared to the pre-operative radiographs. The distal radial and ulnar growth plates were still open bilaterally (Fig 4c), but the affected left radius was 7 mm (7%) than on the contralateral side (Table 1).

Post-treatment radiographs of case 2. (a) Mediolateral radiograph after ostectomy of the ulna just proximal to the distal metaphyseal area. Note the irregular appearance of the distal radial physis. (b) Craniocaudal radiograph after ostectomy of the ulna. (c) Craniocaudal radiograph of the left antebrachium 8 months after ulnar ostectomy. The antebrachiocarpal joint is congruent and the ulnar ostectomy has healed. The distal radial and ulnar physes have a normal appearance and the ulnar physis is now located proximal to the radial physis.
Case 3
A 1.2 kg, 4.5-month-old, female Persian cat presented after a fall from the third floor. The cat was non-weight bearing on the left thoracic limb. The left carpal area was swollen and painful on manipulation. A fracture of the styloid process of the ulna was diagnosed on radiographs (Fig 5a). The antebrachiocarpal joint appeared stable. Further radiographs obtained 12 days later revealed widening and a cranioproximal to caudodistal tilting of the distal radial growth plate, which was interpreted as an early sign of premature closure (Fig 5b). Distraction osteogenesis of the affected antebrachium was planned because of the growth potential of the cat and the experience gained with the first case. Because commercially available distraction devices were considered too large, a small linear distractor was built, using components from the IMEXtm Miniature Circular External Skeletal Fixation System, (Texas, USA) and the tubular external fixator system (FESSA; Medical Solution GmbH, Steinhausen, Switzerland). A 4 mm threaded rod with a thread pitch of 0.7 mm (IMEXtm) was inserted proximally and distally into 6 mm tubes (FESSA), and secured with a corresponding screw distally. A nylon nut (IMEXtm) was placed on the proximal end of the threaded rod to allow distraction.

Pre-treatment radiographs of case 3. (a) Mediolateral radiographs of the carpus of the 4.5-month-old cat showing a non-displaced fracture at the distal part of the ulnar styloid process. (b) Widening and cranioproximal to caudodistal tilting of the distal radial physis is evident on the mediolateral radiograph obtained 12 days after the injury.
A transverse diaphyseal radial osteotomy was performed and the linear distractor applied to the medial aspect of the radius. The ulna was also osteotomised to allow unrestricted distraction and prevent carpal incongruity. Distraction was started on the second day after surgery with a distraction rate of 0.35 mm per day (0.175 mm twice daily) for 1 week. After 1 week resistance was encountered during distraction. On radiography the osteotomy gaps had filled in with new bone and were reduced to a width of 1 mm. The proximal pins showed signs of loosening. The loose pins were replaced and the distraction rate increased to 0.7 mm per day (0.35 mm twice daily) for another 14 days (Fig 6a). Mild contraction of the antebrachial flexor muscles occurred during the distraction period, but resolved with physiotherapy. Measurements at the end of distraction showed an increase in length of the radius of 14 mm. The affected radius was 6 mm longer than the contralateral one (Table 1). The osteotomy gap healed within 5 weeks and the external fixation device was removed (Fig 6b). The cat was using the leg well at this time, but carpal flexion was markedly reduced to about 10°. Unfortunately, the cat was not available for follow-up when fully grown.

Post-treatment radiographs of case 3. (a) Mediolateral radiograph of the antebrachium at the end of the distraction period shows new bone formation at both the proximal and distal osteotomy ends of the radius and ulna. (b) The osteotomy gaps had filled with bone and the external fixator was removed 5 weeks after stopping distraction. Both physes are almost closed. Degenerative changes are present within the carpal joint.
Discussion
Three cats with premature closure of the distal radial physis were seen over a period of 2 years. During that time no cats were diagnosed with premature closure of the distal ulnar physis. This is in contrast to dogs, where premature closure of the distal ulnar physis is the most common form of antebrachial limb deformity (Fox 1984, Johnson and Hulse 2002, Boudrieau 2003). The distal growth plate of the ulna has a conical shape in dogs, which means that any laterally directed force to the distal limb results in a compression injury of the physis (Fox 1984). The distal ulnar physis in cats does not have a conical shape, but is orientated perpendicular to the long axis of the ulna. It may, therefore, be less prone to compression injury and subsequent premature physeal closure.
In all three cats the injuries resulted from fall from a height. Only one cat had a radiographically detectable fracture through the distal radial physis on initial examination. Fractures of the ulnar styloid process and metacarpal fractures were present in the other two cats. Falls from a height could possibly have caused compression injury to the growth plate that was not clearly visible on initial radiographs. Immature cats with any kind of distal forelimb injury, especially fractures of the ulnar styloid process, should therefore have follow-up radiographs after 2 or 3 weeks to detect early signs of premature physeal closure.
Carpal joint incongruity was seen in all three cats in this report. This is in contrast to dogs, in which premature closure of the distal radial physis often causes elbow incongruity (Carrig 1983, Shields Henney and Gambardella 1990). Growth cessation tended to be asymmetric, being more pronounced at the dorsal (cases 1 and 3) and/or lateral aspect (cases 1 and 2) of the distal radial physis. In dogs, asymmetrical closure of the distal radial physis results in valgus deformity of the distal limb (Vandewater and Olmstead 1983, Fox 1984, Shields Henney and Gambardella 1990). No clinically visible valgus deformity was present in the cats, but cases 1 and 2 showed a valgoid deviation of the distal radius radiographically, with an enlarged joint space in the lateral area of the radiocarpal joint. This was most likely caused by asymmetrical physeal closure and exaggerated by continued growth of the ulna.
The use of an ulnar ostectomy has been described to correct elbow incongruity in dogs with premature closure of the distal radial physis (Shields Henney and Gambardella 1990). Distal ulnar ostectomy improved radiocarpal joint congruity by allowing the distal part of the ulna to shift proximally in case 2. A wide ulnar ostectomy was not performed in the other two cases, but would possibly have been beneficial to reduce the ulnar length to match the radial length. Cats are lacking a strong interosseous ligament between radius and ulna (Vollmerhaus et al 1994), which may allow some degree of motion of the ulna in relation to the radius.
The distal radial physis closes between 14 and 20 months of age in intact cats (Smith 1969) and even later in neutered cats (May et al 1991, Houlton and McGlennon 1992, Root et al 1997). The mean length of the feline radius was approximately 70 mm in 5-month-old cats and 85–100 mm in 20-month-old cats. Neutered cats had the longest radii (Root et al 1997). These measurements indicate that if premature physeal closure occurs at 5 months of age, loss of radial length until maturity could approach 15–30%. This is consistent with case 1 of the present report, which had a 26% decrease of radial length when compared to the contralateral side at 28 months of age (Table 1). The affected radius was only 7% shorter than the contralateral radius in case 2 when the cat was 14 months old, with a normal radiographical appearance of the distal radial physis. The most likely explanation is that continuous growth was possible due to incomplete or reversible physeal damage in this case. The percentage of growth retardation could not be evaluated in case 3 because the cat was not available for follow-up. In any event, the cat would have lost 8 mm (12%) of radial length between 4.5 and 7 months of age if no distraction had been performed.
Loss of bone length exceeding 15–20% is generally considered significant for the forelimb. Premature closure of the distal radius in a dog less than 5 months of age leads to significant loss of bone length, rendering distraction osteogenesis likely to be necessary (Boudrieau 2003). The low case number and the inconsistency in the amount of radial shortening does not allow any conclusions regarding the indications for limb lengthening procedures in cats with premature closure of the distal radial growth plate, but the authors feel that distraction osteogenesis should be considered in cats younger than 4–5 months with complete closure of the distal radial physis. A daily distraction rate of 0.7 mm per day allowed uncomplicated distraction and new bone formation in case 3. The cat tolerated the procedure well and was using the leg throughout the distraction period.
Overall, clinical outcome was good in all three cats with no obvious lameness at the final examination. The range of carpal flexion remained reduced during the observation period in all of the patients. Prolonged immobilisation of the carpus with a splinted bandage in cases 1 and 2, cranioproximal to caudodistal deviation of the physis with subsequent hyperextension of the radiocarpal joint in cases 1 and 3, and limb shortening in case 1 could have contributed to the reduction in antebrachiocarpal range of motion.
Conclusion
The possibility of premature closure of the distal radial physis should be considered in immature cats with trauma to the distal forelimb, especially after falls from a height. Clinically significant losses of radial length are likely to occur in cats younger than 4–5 months. Joint incongruity is more likely to develop in the carpal joint than in the elbow joint. Carpal incongruity can be corrected in some cases by distal ulnar ostectomy, allowing the joint subluxation to reduce when the distal part of the ulna shifts proximally. Distraction osteogenesis is feasible in cats and may be indicated in cases of premature closure of the distal radial physis in cats younger than 4–5 months.