
Abstract
This prospective observational study evaluated client-reported recurrence of lower urinary tract signs (LUTS) and other signs of abnormalities in cats with idiopathic cystitis after institution of multimodal environmental modification (MEMO). Forty-six client-owned indoor-housed cats with idiopathic cystitis, diagnosed based on a history of recurrent LUTS and evidence of absence of urolithiasis or bacterial urinary tract infection were studied. In addition to their usual care, clients were offered recommendations for MEMO based on a detailed environmental history. Cases were followed for 10 months by client contact to determine the effect of MEMO on LUTS and other signs. Significant (P<0.05) reductions in LUTS, fearfulness, nervousness, signs referable to the respiratory tract, and a trend (P<0.1) toward reduced aggressive behavior and signs referable to the lower intestinal tract were identified. These results suggest that MEMO is a promising adjunctive therapy for indoor-housed cats with LUTS, and should be followed up with prospective controlled clinical trials.
Lower urinary tract signs (LUTS; hematuria, dysuria, pollakiuria, urination in inappropriate places in the client's home, with or without urethral obstruction) affect some 1.5% of cats presented to primary care veterinarians (Lund et al 1999). Moreover, abnormal elimination is a common cause of surrender of cats to animal shelters (Patronek et al 1996). Much veterinary interest has focused on inappropriate elimination behavior, urolithiasis and urethral plugs as major causes of LUTS, although a variety of reports have concluded that no specific cause could be identified in the majority of cases (reviewed in Westropp et al 2005).
LUTS may be associated with disorders affecting the bladder or urethra from within the lumen such as urolithiasis and urinary tract infection, from intrinsic abnormalities such as transitional cell carcinoma, and from disorders of other organ systems, such as behavioral elimination disorders (Neilson 2004) and idiopathic cystitis (Buffington 2004). Cats with interstitial cystitis (a subset of cats with idiopathic cystitis), for example, appear to have increased activity of their stress response system and decreased adrenocortical function in response to stressful circumstances (Westropp et al 2003, Buffington 2004).
Some cats with LUTS appear to be unusually sensitive to their surroundings, which could affect disease expression (Buffington et al 2006). The sensitivity of cats to their surroundings has long been recognized (Darwin 1872, Cannon 1929). Recent ethological studies in zoos (Carlstead et al 1992), research laboratories (Carlstead et al 1993) and boarding facilities (Kessler and Turner 1999) have documented that cats subjected to impoverished (lacking in appropriate novelty and complexity) or unpredictable environments have decreased activity levels and increased hiding behaviors.
The indoor environment of some house cats also may be monotonous and predictable, which could be stressful (Van Rooijen 1991). The success of adaptation of cats to indoor environments may thus depend on the quality of the environment and the adaptive capacity of the cat (Koolhaas et al 1999).
Modifications of the environment may benefit indoor-housed cats. Environmental enrichment has been documented to improve animal health and welfare in most (Widman et al 1992, Carlstead and Shepherdson 2000, Buffington 2002, Van de Weerd et al 2003), but not all circumstances (Newberry 1995). We define multimodal environmental modification (MEMO) as institution of changes in the cat's environment to attempt to reduce LUTS by decreasing the likelihood of activation of the stress response system. These changes include client education, and variable combinations of changes in the cat's inanimate physical environment and diet, as well as its interactions with other cats, other animals, and humans in the cat's environment (Westropp and Buffington 2004). We agree with van Praag et al (2000) that, given our current state of knowledge, the relative importance of single contributing factors cannot be easily isolated in any particular case. This may be because an individual's responses (both positive and negative) to its environment depend on its unique life history, expectations and the context (environment) in which it lives. The role of single variables on environmental enrichment have been studied, particularly the effects of socialization and general activity (Bernstein 1973, Rosenzweig et al 1978), but results generally have revealed that no single variable can account for all consequences of enrichment (van Praag et al 2000). Thus, MEMO attempts to include and extend the concept of environmental enrichment to include as many features of the cat's environment as possible (Buffington 2002, Rochlitz 2005).
Based on the potential role of environment on LUTS, provisional recommendations for MEMO of indoor-housed cats have been suggested (Buffington 2002). The present study was designed to begin to investigate the effects of MEMO on recurrence of LUTS in indoor-housed cats with idiopathic cystitis.
Materials and Methods
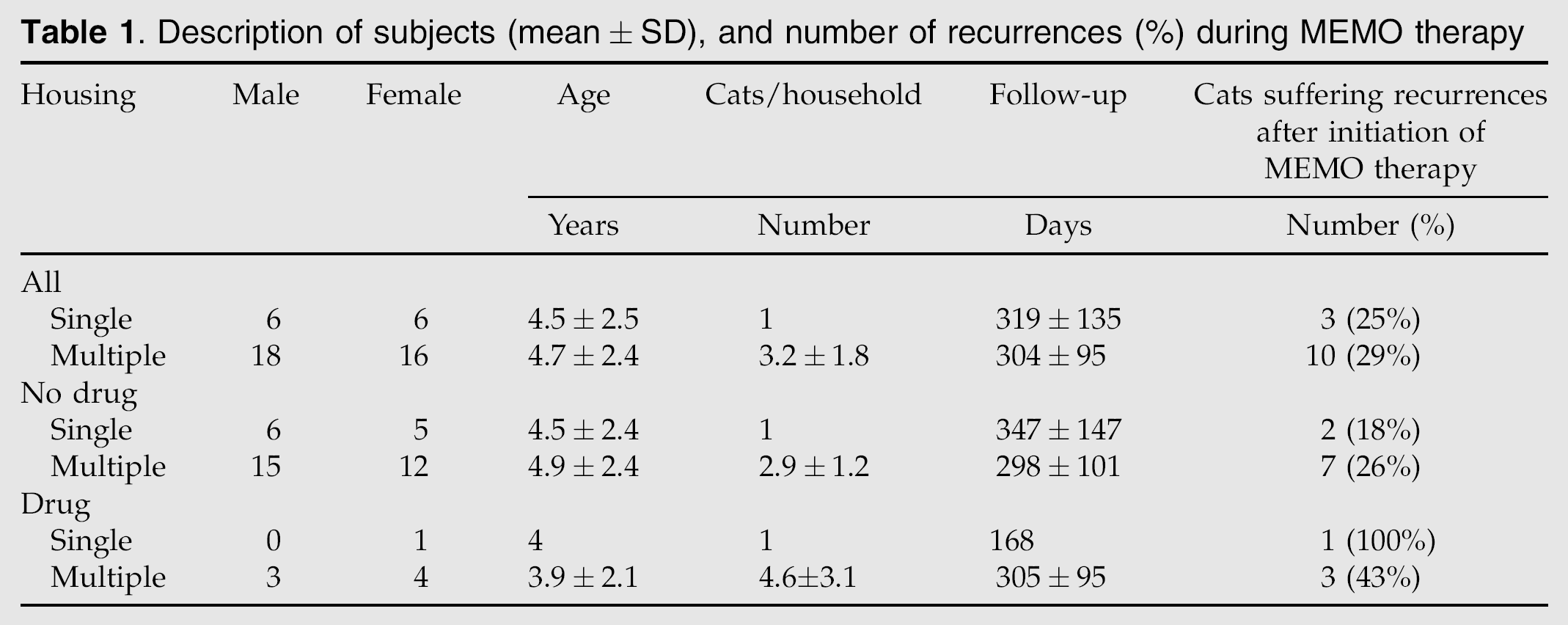
Male and female cats between 1 and 10 years of age evaluated by clinicians at The Ohio State University Veterinary Hospital or primary care practices in the Columbus, OH area for recurrent LUTS were referred for inclusion (Table 1). Clients were offered entry into this study if their cat had suffered at least two bouts of LUTS in the 10 months preceding the study, although the median frequency (weekly) was much higher (Table 2, Fig 1).

Effects of 10 months of environmental enrichment on abnormal signs in cats with idiopathic cystitis (median, 25th, 75th percentage quartiles). I=initial, F=final, LUTS=lower urinary tract signs.
Description of subjects (mean±SD), and number of recurrences (%) during MEMO therapy
Effect of environmental enrichment on client-reported signs of abnormalities in cats with idiopathic cystitis (median, 25th, 75th percentage quartile)
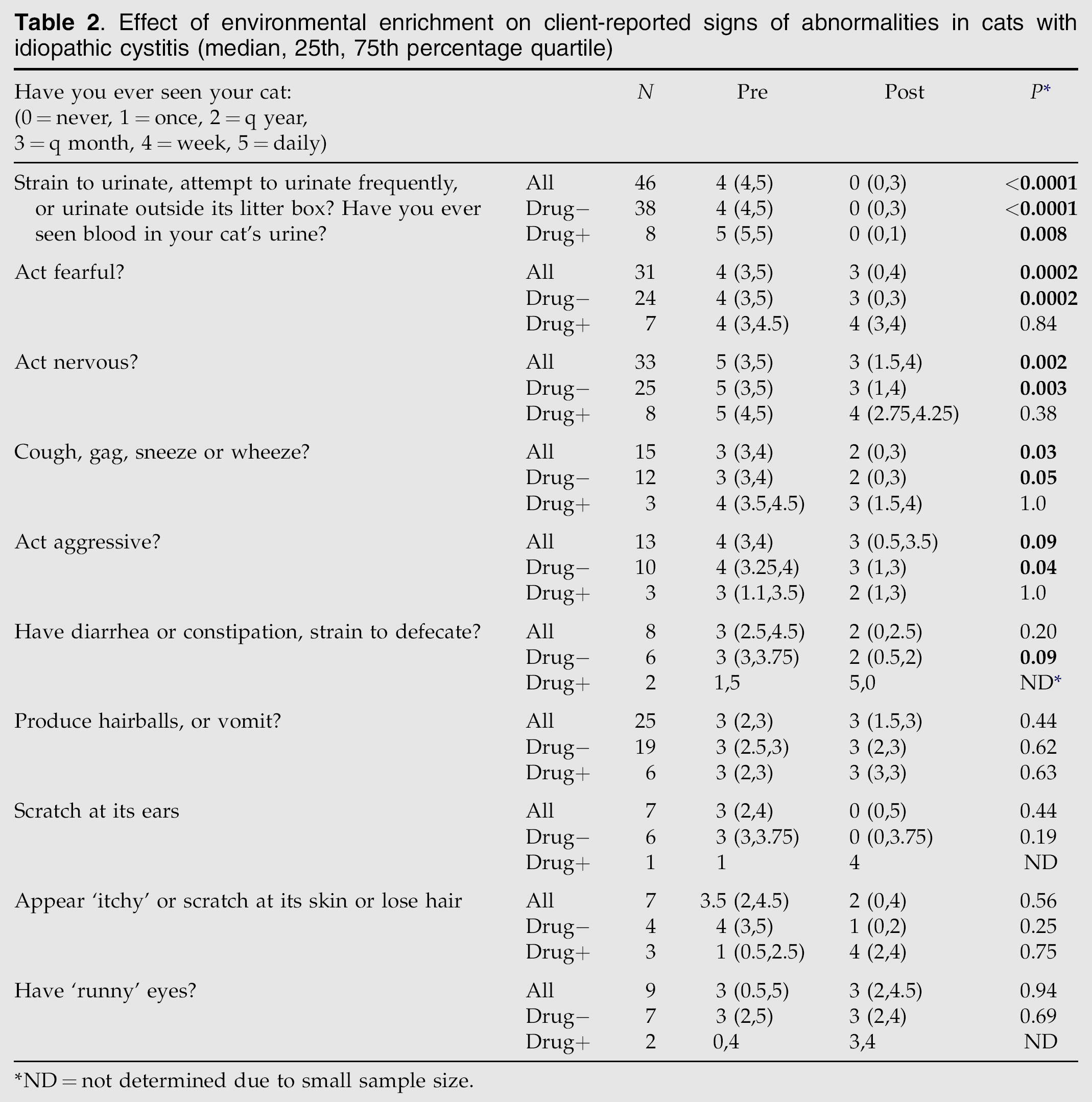
ND=not determined due to small sample size.
Clinical signs included variable combinations of hematuria, dysuria, stranguria, urination in inappropriate places in the client's house, and pollakiuria. Although clinical evaluation varied by practice, absence of evidence of both bacterial urinary tract infection (based on presence of concentrated urine, and absence of pyuria or observable microorganisms) by urinalysis and radiodense uroliths by plain radiological imaging was required of all patients for inclusion (Buffington et al 1997). Due to the severity of disease in these cats, prior therapy had included a variety of treatments, including variable combinations of drug and individual environmental interventions (diet, litter box) before referral for inclusion into the study. Based on client report, a specific regimen of MEMO had not been prescribed for any of the cats before referral for potential inclusion into the study.
Informed consent for inclusion in the MEMO study was obtained from clients with cats meeting the inclusion criteria. An interview with the client was conducted either in person or by telephone to obtain a review of systems and environmental history (Westropp and Buffington 2004). The history included a standardized questionnaire that each client completed in its entirety. Questions were asked about LUTS and a variety of clinical signs pertaining to various other organ systems, and about the cat's current environment (questionnaire available at www.indoorcat.org). Clients also were questioned about aspects of their cat's behavior including the frequency of observed nervous, fearful or aggressive behavior. These terms were not defined for the client unless asked; if asked, terms were defined according to standard dictionary definitions: nervous generally means easily excited or irritated, jumpy, timid, or apprehensive; fearful generally means fleeing, hiding or withdrawing from stimuli that would not be thought to affect cats in this way, and aggressive generally means hostile, injurious, or destructive.
Based on the interview, a MEMO plan was developed in collaboration with the client based on environmental factors identified during the interview. The objectives of the plan were to: 1) empower clients to understand how their efforts would contribute to the cat's recovery and remission of LUTS, 2) help the client manage the cat's environment, and 3) help reduce the cat's perception of environmental threat, whatever the potential source(s).
Recommendations included variable combinations of provision of information concerning the physiological abnormalities underlying the disease and explanation of the futility of ‘blaming the patient’ for the client's frustration associated with occurrence of LUTS. Clients also were assured that the indoor environment they provided had not caused a disease in a previously healthy cat, but rather had unmasked an underlying abnormality that may have been congenital (Buffington 2004). Suggestions for reducing the effect of environmental and/or social stressors included avoiding punishing the cat, diet change to a canned food if acceptable to the client and the cat (offering a canned food in addition to current diet was recommended; if accepted, the dry food was gradually removed), increasing water intake, change to an unscented, clumping litter if acceptable to the client and the cat, institution of improved litter box management, provision of climbing structures, viewing and resting perches, scratching posts, and audio and video sensory stimulation when the client was absent from the home as appropriate, increased client interaction with the cat, and identification and resolution of conflict in multiple cat households (Westropp and Buffington 2004). Clients were encouraged to identify changes they believed to be most relevant to their particular circumstances, and instructed to make changes to the environment sequentially and slowly (over several days) to permit the cat to adapt to the changes made.
The plan was provided to the client and reviewed with them in person, or over the phone if mailed. A copy of ‘From the Cat's Point of View’ by Gwen Bohnenkamp was provided to each client to be sure clients had a specific information resource to consult during the change process. Clients also were provided with the address of The Indoor Cat Initiative website (http://www.indoorcat.org), and encouraged to visit it to review recommendations provided for specific areas for MEMO identified during the interview. Printed recommendations were provided to clients without Internet access.
Eight cats, which had not previously been exposed to medication, were started on drug therapy by the attending clinician in addition to referral for MEMO. Drug therapy was not considered to be a component of MEMO, but to be a separate therapy to which MEMO was added, so both overall results and results from the cats that had ‘drug+’ and had not ‘drug−’ received drug therapy in addition to MEMO were determined.
Follow-up telephone or electronic mail contacts were made to determine the progress and success of the recommended interventions on an approximately monthly basis. Clients also were encouraged to request assistance whenever questions or concerns arose. When problems implementing the MEMO recommendations arose, the plan was modified as appropriate in collaboration with the client. Information concerning the effects of MEMO on other clinical signs that may have been present along with the LUTS was obtained at the start and end of the interaction with each client.
Statistical Evaluation
Initial and final client-reported frequencies of LUTS and other signs were compared using the Wilcoxon signed rank test using statistical software (Prism, Version 4, GraphPad Software, San Diego, CA). For each sign, only cases that reported a frequency greater than once at the start or end of the study were included, so number of cases analyzed differed between signs (Table 2).
Results
Participation in the study was offered to 73 clients with cats having idiopathic cystitis. Of these, owners of 27 cats did not participate after initial contact for the following reasons. Four did not meet inclusionary criteria (two for age, and two for the presence of stones in the urinary tract). Two were euthanased and four withdrawn when clients decided that the cat's disease was too severe to treat. Thirteen clients were extremely hard to reach, and were dropped from the study after repeated attempts to contact them over a 3 month period failed; sporadic contact was maintained with the other four for 6–12 months, during which no signs of recurrence were reported. Data are thus reported for a total of 46 cats. Descriptive data for these cats and LUTS recurrences during the study are presented in Table 1. Effects of MEMO on client-reported signs of abnormalities are presented in Table 2 for all cats having the sign greater than once before or after the study as a group, and with cats divided into ‘drug−’ and ‘drug+’ groups.
In addition to initial client education, the most commonly followed MEMO recommendations were to read the information provided (additional client education), increase the amount of time interacting with the cat, change to a canned diet, and add another litter box. In the multiple cat households, clients with two cats made a total of four changes, nine made three, six made two, eight made one, and details of specific changes were unavailable from nine clients. Specifically, clients reported making variable combinations of changes in the cat's physical environment (12), increases in time spent interacting with the cat (10), change to a canned food (10), increases in litter box number, location and cleaning frequency (nine), and specific efforts to reduce inter-cat conflict (three). In addition to these changes, pharmacological therapy was prescribed for seven cats; amitriptyline for five and acepromazine for two.
In the single cat households, owners of three cats made a total of three changes, one made two, five made one, and details of specific changes were unavailable from one client. Specifically, clients reported making changes in the cat's physical environment (four), change to a canned food (four), increases in litter box number, location and cleaning frequency (three), and in time spent interacting with the cat (two). Pharmacological therapy (clomipramine) was prescribed for one cat.
During the approximately 10 month average time of follow-up, no signs referable to the lower urinary tract were observed in 70–75% of the cats, resulting in a highly statistically significant decrease in frequency of LUTS (Table 2, Fig 1), regardless of inclusion of drug therapy into the treatment plan (Table 2). In cats suffering recurrent episodes, the clients reported that the LUTS resolved spontaneously without additional veterinary intervention. Significant reductions in fearfulness, nervousness and upper respiratory signs, as well as trends toward reductions in aggressiveness and lower intestinal tract signs, also were reported by clients (Table 2).
Discussion
The most important result of this study was the highly clinically and statistically significant reduction in LUTS by addition of MEMO to usual therapy. Moreover, MEMO was found to have a positive effect on some aspects of the cat's behavior, and on signs referable to some other body systems. These changes are consistent with reductions in the output of the stress response system of cats, which has been found to be abnormal in cats with feline interstitial cystitis, a cystoscopically defined subset of idiopathic cystitis (Buffington 2004).
Other studies of cats with LUTS also have proposed a role for the external environment in recurrence of signs. A 1925 description of cats with LUTS suggested that confinement to the house played a role in the development of the signs (Kirk 1925). In 1971, Caston reported an increased number of cases of cats with LUTS during a period of earthquake aftershocks in California after the Sylmar-San Fernando earthquake. He recommended, among other things, that treatment include, “An effort…to determine the stress, and, where possible, remove it” (Caston 1973). More recently, Cameron et al (2004) found several stress factors associated with idiopathic cystitis, including inter-cat conflict.
Descriptions of a variety of other approaches to therapy for cats with LUTS have reported rates of recurrence that may be compared with the frequency of recurrence of LUTS we observed during the 10 months of the study. In one study, clinical signs recurred in 13 of 33 cats (39%) within 1 year regardless of treatment (Barsanti et al 1982). Recurrence of LUTS in cats provided only diet therapy also has been reported (Markwell et al 1999). In this study, recurrence of LUTS occurred in 11% of cats fed the canned, and 39% of cats fed the dry form of a commercial diet designed to result in production of an acidic urine. Fourteen cats in the present study were switched from a dry to a canned food as part of MEMO. Ten of these lived in multiple cat households and four experienced a recurrence, whereas none of the four singly housed cats suffered a recurrence. Thus, the overall rate of recurrence of LUTS in cats in the present study was intermediate between that identified in our previous study, in which no specific MEMO recommendations were made (Markwell et al 1999). Because of the nature of the intervention in the diet study, however, the study was biased toward subjects in single cat households to reduce the availability of alternative food sources. The severity of disease in the subjects in the diet study, 71% had suffered two or fewer episodes of LUTS in the preceding 12 months, also was not as great as in the subjects of the present study. Moreover, modification of other features of the environment was not recorded or considered in the analysis. Although the diet of too few cats in the present study was changed to permit statistical analysis of these data, the data suggest that provision of canned food may have different effects depending on the number of cats in the household.
Diet may affect outcome for a variety of reasons. Nutrient content (including water), constancy vs. novelty of the diet presented, the form (dry vs. canned) of the diet and the method of feeding all may play variably important (and relatively unstudied) roles in MEMO. For example, the method of food delivery may contribute to MEMO by variable combinations of stimulation of exploratory behavior, provision of contingencies, incorporation of variation into the animal's schedule, and enabling invention (Overall and Dyer 2005, Overall et al 2005). More recently, Gunn-Moore and Shenoy reported a placebo-controlled study of oral glucosamine in the management of idiopathic cystitis in 40 cats (Gunn-Moore and Shenoy 2004). In this study, LUTS recurred in 26 of 40 (65%) patients within 6 months, despite the fact that the owners of 90% of the cats also started feeding more canned cat food. Thus, diet change alone may not be sufficient to effect remission in cats with more severe cases of idiopathic cystitis.
Pharmacological therapy was incorporated into the treatment of eight cats in the present study. Pharmacological approaches to the treatment of various causes of LUTS in cats have been reported previously (Marder 1991, Buffington et al 1997, Chew et al 1998, Kruger et al 2003). Administering oral medications can be stressful for some cats and clients, so it is recommended that pharmacotherapy be reserved for recurrent, severe cases, and only after MEMO approaches have proven inadequate to control signs.
The results of the current study need to be considered in the light of the biological behavior of idiopathic cystitis to determine whether they represent a real clinical benefit. Inclusion of an unmanaged comparison group in the study was considered, but for this exploratory study was rejected in favor of comparison to historical results. The dearth of published studies of environmental therapy for idiopathic cystitis suggested that a preliminary trial of the approach was indicated to determine if any beneficial effects could be identified. Although observational studies provide weaker empirical evidence than do experimental studies, they can provide useful preliminary evidence to inform decisions concerning the advisability of subjecting a therapeutic approach to prospective randomized controlled trials. Because potentially relevant and durable clinical results were identified in this study, further prospective controlled trials seem indicated.
The mechanism(s) of the clinical benefit was not determined by the study. Based on our other studies of cats with severe cystitis, one possibility is that MEMO resulted in decreased activation of the stress response system (Buffington 2004). Our observation that there were reductions in abnormalities in other systems is consistent with this possibility; beneficial behavioral changes also have been observed by others during therapeutic trials of cats with idiopathic cystitis (Gunn-Moore and Cameron 2004). Psychosocial stress (Harhaj and Antonetti 2004) has been shown to increase epithelial permeability (as we have identified in the urothelium; Lavelle et al submitted for publication) by reducing tight junction integrity (Apodaca 2004) in a variety of tissues (Bredy et al 2004, Ma et al 2004) by complex mechanisms, which may activate peripheral nociceptive and inflammatory responses. Additionally, experimental studies of rodents subjected to early adverse experience have documented psychoneuroendocrine abnormalities, which may be compensated for, if not repaired by, MEMO (Newberry 1995, van Praag et al 2000, Laviola et al 2004). These studies may be pertinent to cats with idiopathic cystitis, as the psychoneuroendocrine abnormalities identified in some of these cats may be the result of early adverse experience (Westropp and Buffington 2004). The form that the MEMO takes in any particular case, however, must be carefully considered to assure that it results in an improvement in the biological functioning of the animal (Widman et al 1992, Newberry 1995, Hart 1996).
In conclusion, MEMO resulted in significant improvement of LUTS in cats with idiopathic cystitis, as well as improvement of signs referable to some other organ systems. Indoor housing and stress have been associated with a number of common disorders of cats, including behavioral problems (Heidenberger 1997), diabetes (Rand et al 2004), dental disease, hyperthyroidism, obesity, separation anxiety disorder, and urolithiasis (Buffington 2002). Given the increased disease in indoor-housed cats, and the ease and safety associated with MEMO, we recommend that this approach be offered to all clients with indoor-housed cats as part of preventative health care. As has been advocated by behaviorists for behavioral inappropriate urination and urine marking (Hart 1996), we recommend institution of MEMO for cats with idiopathic cystitis before institution of drug therapy, as in our clinical experience, such therapy is more likely to be effective in enriched environments. To the authors' knowledge, studies of the effects of MEMO on indoor-housed cats with disorders other than idiopathic cystitis have not been reported, but given the present results it may be worthy of investigation. This is not to say that stress causes any of these disorders, only that stress reduction may play an adjunctive role in the therapy of some chronic feline disorders, as it may in humans (Barrows and Jacobs 2002).
Footnotes
Acknowledgments
The expert technical assistance of N.R. Baldwin is gratefully acknowledged. Supported by a grant from the Kenneth A. Scott Charitable Trust, and NIH DK64539 (Center for Neurovisceral Sciences and Women's Health).