
Abstract
Thymolipomas are rare benign thymic neoplasms recognised in humans, composed of mature adipose tissue and thymic tissue. An 8-year-old male domestic shorthair cat presented with anorexia, lethargy and vomiting secondary to the development of a thoracic effusion and an anterior mediastinal tumoral mass with fatty appearance. Histologically, the mass consisted of adipose tissue containing numerous cords and nests of cortical and medullary thymic tissue. No signs of thymic epithelial or lymphoid neoplastic proliferation were detected. The findings in this case are remarkably similar to the macroscopic and histological features of thymolipoma in humans.
Tumours arising from the thymus in domestic animals include thymomas and lymphomas (Vali 1993). Thymic lymphomas are high grade, lymphoblastic or immunoblastic true lymphoid tumours, whereas the term thymoma is restricted to define those neoplasms arising from thymic epithelial cells regardless of the degree of lymphoid proliferation. Based on the proportion of proliferating epithelial cells and lymphocytes, as well as the atypia of the epithelial cell component, thymomas have been further classified as predominantly lymphocytic, mixed (lymphoepithelial), or predominantly epithelial (Vali 1993).
Besides the aforementioned tumours, thymic neoplasms in humans include germ cell tumours, carcinoids and thymolipomas (Rosai and Levine 1976). Thymolipomas are unusual benign neoplasms composed of mature adipose and thymic tissue. They represent less than 10% of all thymic neoplasms in man. In this paper, we present a case of thymic tumour in a cat with features of the human thymolipoma.
An 8-year-old male castrated domestic shorthair cat, weighing 7 kg, was presented for anorexia, lethargy and vomiting of 1 week duration. The cat had no previous history of illness. On physical examination the cat was depressed and mildly dehydrated. Rectal temperature was 37.3 °C, respiration was rapid and shallow (40 breaths/min), pulse was weak and the heart rate was 150 beats/min. The lungs and heart sounds were muffled. Supportive therapy was provided while further investigation was performed. Initial laboratory abnormalities included mild anaemia (packed cell volume 32%; reference 37–55), increase in total protein (80 g/l; reference range 5.4–7.8) and elevated urea (78.89 mmol/l urea; reference range 5–11). The cat was given a balanced electrolyte solution intravenously (Ringer solution at 15 ml/kg/h). A thoracic radiograph was undertaken but during the procedure the cat begun with dyspnoea as evidenced by open-mouth breathing, and died.
At the owner's request, a restricted post mortem examination was performed examining only the thoracic cavity. A bilateral thoracic white opaque pleural effusion and an anterior mediastinal mass that did not invade adjacent structures were detected. A sample of the milky fluid from the thorax had a specific gravity of 1027 and a protein content of 3.6 g/dl. The predominant cell type in the sediment was lymphocytes with a few segmented neutrophils. Because the milkiness did not clear when the fluid was centrifuged, a tentative diagnosis of chylous or pseudochylous effusion was made.
The anterior mediastinal mass had the appearance of an enlarged thymus displacing caudally the lungs. It was well-circumscribed, encapsulated, about 20 cm long, with no adhesions to the surrounding tissues. On cut section, it had a homogenous, yellowish and soft appearance, resembling normal adipose tissue divided into lobules by thin trabeculae. In spite of its normal fatty appearance, the mass gave the impression of a tissue of higher consistency than normal fat, because of the presence of multifocal solid areas. No other gross lesions were observed, and tissue samples of the mass were routinely processed for histopathological examinations.
On low-power view, the mass was composed of multiple lobules consisting of mature adipose tissue and thymic tissue. The former represented approximately 30% and the latter 70% of the tumour. Both components could be clearly recognised even if they were haphazardly admixed (Fig 1). Thymic tissue consisted of randomly distributed, multiple foci of normal cortical and medullary thymic zones. Medullary areas predominated over cortical areas. The former contained numerous Hassall's corpuscles, few loosely arranged lymphocytes, and epithelial cells with irregular nuclei and inconspicuous nucleoli (Fig 2). The latter showed a predominance of numerous tightly packed lymphocytes with a few intermingled epithelial cells displaying oval nuclei and prominent nucleoli. Germinal centres were not observed. Some islands of thymic tissue were connected by cords of lymphocytes, adopting a strand-like disposition. The rest of the tumour was composed of normal mature adipose tissue, surrounding these islands of thymic tissue. Adipocytes were arranged in lobules separated by vascularised fibrous septa. The margins of the tumour were limited by a thin fibrous capsule, with adhered strands of lymphoid cells, representing probably remnants of thymic tissue. In some cases, these areas also contained variable numbers of tangible body macrophages. No necrosis, haemorrhages or signs of cellular atypia were observed. According to these findings, a diagnosis of thymolipoma was made.
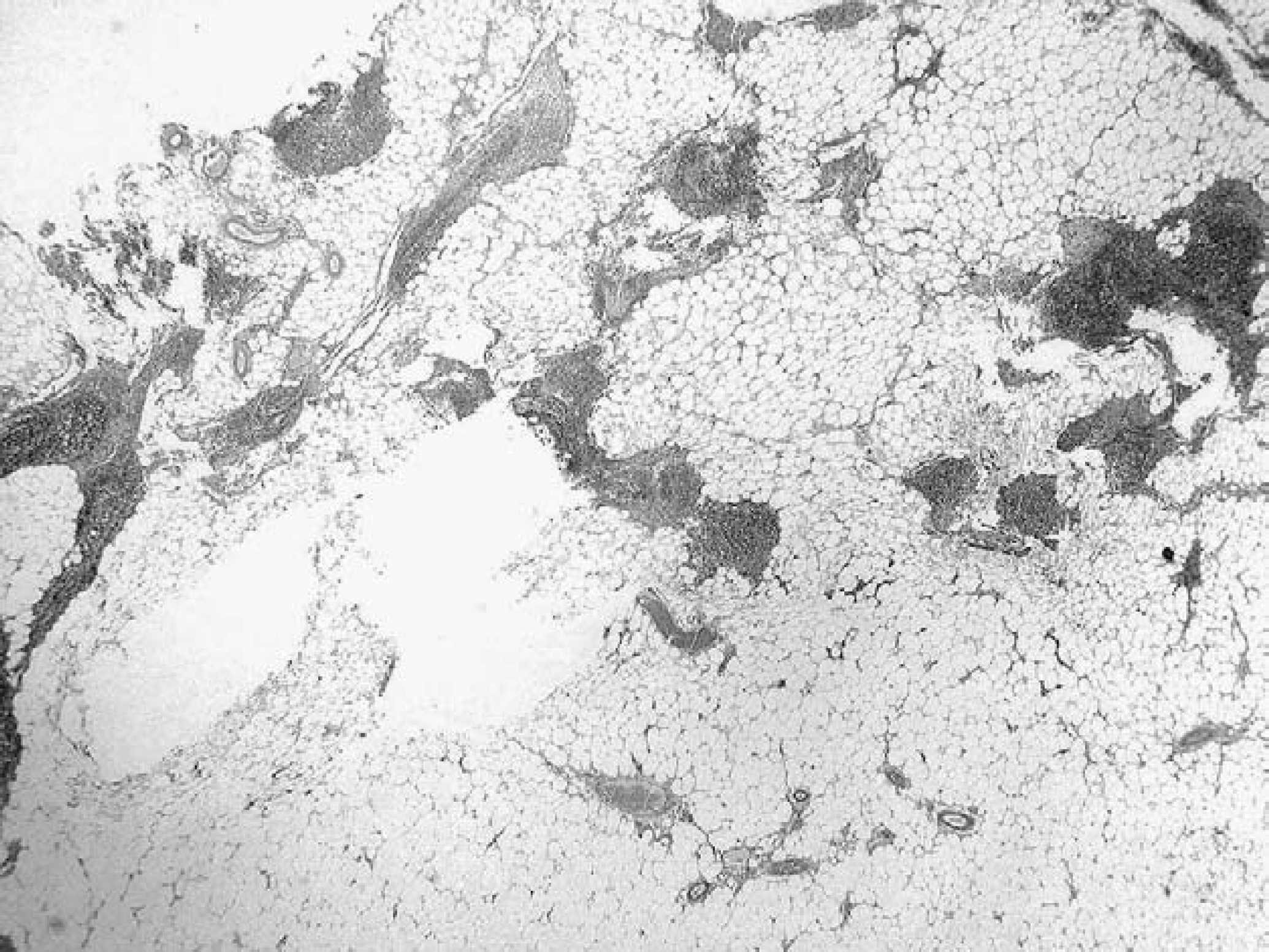
Thymolipoma; cat. Cords and nests of thymic tissue embedded in mature adipose elements (haematoxylin and eosin, magnification ×20).

Thymolipoma; cat. Hassall's corpuscles within a medullary area of thymic tissue (haematoxylin and eosin, magnification ×200).
Thymolipoma in humans is a very rare benign mesenchymal neoplasm of the thymus occurring at any age and without sex predilection (Moran et al 1995). It was first described by Lange in 1916, and since then only a few single cases have been reported (Lange 1916). The pathogenesis of this tumour is uncertain, and subject of speculation in human medicine. The peculiar composition of normal fat interspersed with thymic tissue has given rise to different theories about its origin (Le Marc'hadour et al 1991). One hypothesis suggests that thymolipomas represent a hyperplastic or neoplastic process of the adipose tissue, with incidental engulfment of the thymic gland. Another explanation would be the mixed tumour hypothesis which presupposes that thymolipomas arise from a synchronous proliferation of both endodermal (thymic) and mesenchymal (adipose) tissue. Other investigators hypothesise that thymolipomas are true thymomas undergoing fatty change in a similar manner to fatty replacement of the normal ageing thymus. Finally, it has also been suggested that the lesion represents the involution of a previously hyperplastic thymus, with the consequent fatty replacement.
The diagnosis of thymolipoma in the case presented here is supported by its macroscopic and microscopic characteristics identical to those of previously reported tumours in man (Moran et al 1995). Because of the lack of malignancy, the importance of the diagnosis of thymolipomas in humans lies in the differential diagnosis from other thymic processes. Previously reported proliferative thymic lesions in the cat include lymphoma, thymoma, thymic hyperplasia and thymic cyst formation (Day 1997). In this case, no signs of epithelial or lymphoid neoplastic proliferation were observed. Further, signs of hyperplasia or cyst formation were also not present. Moreover, thymic hyperplasia could be distinguished from thymolipoma by the presence of thymic tissue with a normal architecture, as opposed to the tumour presented here in which the proportion of fatty to thymic elements is markedly distorted. The possibility that the lesion could represent a mediastinal lipoma does not seem plausible as well, because lipomas are not expected to display thymic epithelial elements as an integral component of the tumour.
Thymolipomas in man are usually asymptomatic, although instances associated with signs related to the presence of a space-occupying mass within the anterior mediastinum, such as a cough or dyspnoea (Moran et al 1995). The cat presented here developed a thoracic effusion, probably of chylous nature although serum and pleural fluid cholesterol and triglyceride concentrations were not determined. Although not reported in human thymolipomas, pleural effusion is a frequent finding in cats with thymoma and other types of mediastinal lesion (Dru Forrester et al 1991, Day 1997). The origin of the effusion in this case could result from increased thoracic duct pressure, secondary to compression of the cranial vena cava or thoracic duct by the thymolipoma, as suggested in cases of mediastinal lymphoma (Dru Forrester et al 1991).
Because of the soft and malleable nature of thymolipomas, these tumours have the ability to conform to the shape of adjacent structures, making it difficult to detect them on chest radiographs (Rosado-de-Christenson et al 1994). This difficulty is further emphasised by the fact that some thymolipomas may reach a very small size. Computerised tomography (CT) and magnetic resonance imaging (MRI) have considerably improved the diagnosis of this tumour in man. On CT scans, the thymic tissue is recognised as islands of soft tissue density within a fatty mass, whereas MRI is helpful in demonstrating the predominant fatty nature of the tumour (Rosado-de-Christenson et al 1994). In view of the fact that most cases of feline chylotorax remain an enigma, with no apparent underlying abnormality (Fossum et al 1991), CT or MRI studies could be indicated in animals with idiopathic chylotorax, to look for thymolipomas which could have been overlooked on radiographic examinations. A definitive diagnosis, however, can only be reached through histopathological evaluation.
To the authors' knowledge, this is the first report of a thymolipoma in an animal species. Thymolipoma should be included in the differential diagnosis of thymic tumours; the tumour can easily be misdiagnosed because of its normal fat content. Histological evaluation of the mediastinal mass with extensive sampling to identify all tissue components makes a diagnosis because of the demonstration of thymic tissue within the adipose tissue mass.