
Abstract
Primary lung neoplasia is a rare condition of older cats. This report describes a case of left-sided pulmonary collapse, secondary to pulmonary adenocarcinoma in an 11-year-old cat. Left sided pneumonectomy was performed, and adjuvant chemotherapy with mitoxantrone (Novantrone; Lederle) was administered every 3 to 5 weeks, for 10 doses after surgery. Thirty-four months after surgery, the cat remains well and has no radiographic evidence of pulmonary metastasis.
Case report
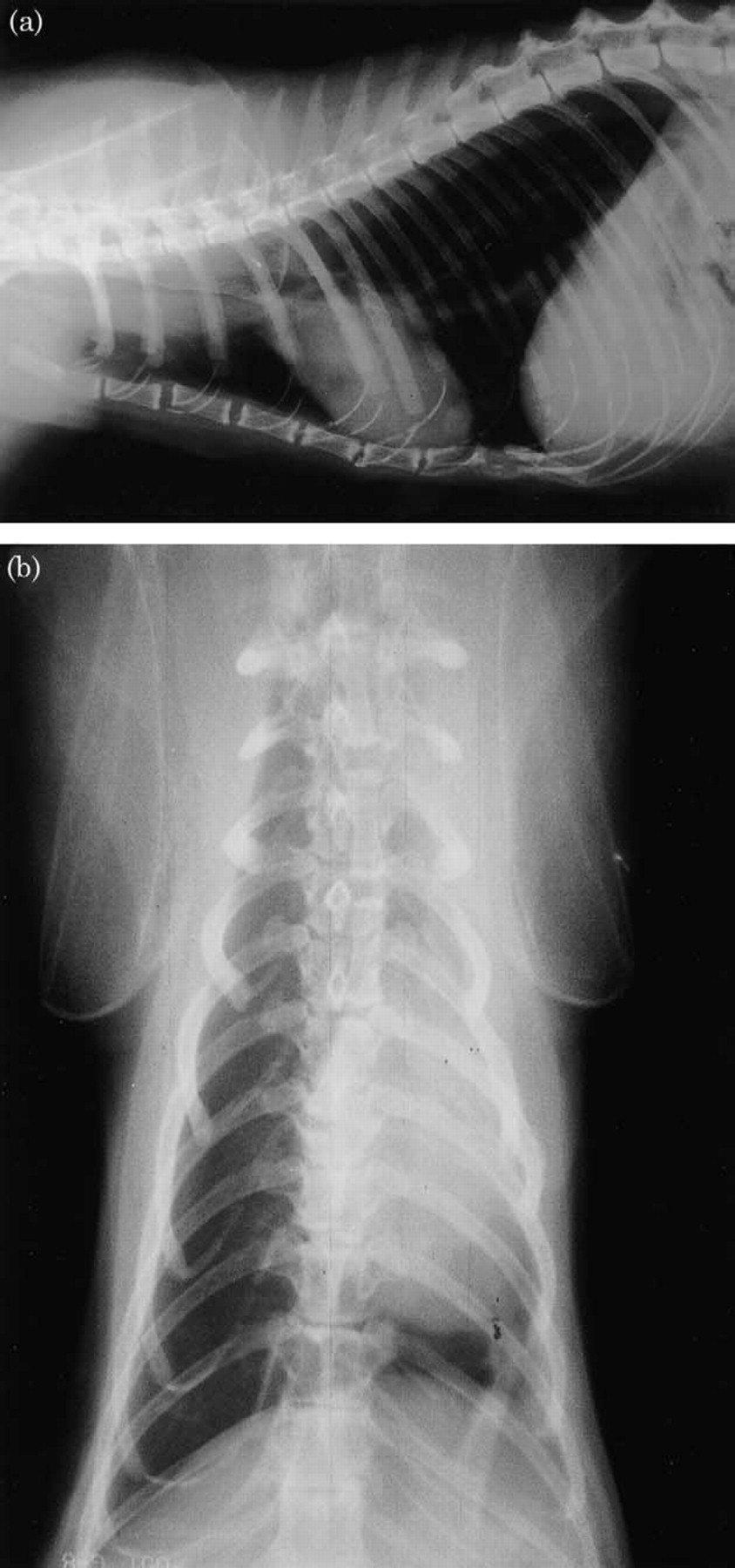
An 11-year-old, female neutered, domestic shorthair cat (3.5 kg) presented to the referring veterinary surgeon with a 5-day history of inappetence and coughing. The cat was slightly underweight and the coat was in poor condition. An elevated respiratory rate (40 breaths per min) and an occasional productive cough were observed. Thoracic radiography, under sedation, identified left-sided pulmonary collapse, compensatory hyperinflation of the right lung lobes, and an irregular mixed (alveolar and interstitial) pattern in the right lung lobes (Fig. 1). Amoxicillin-clavulanate (Synulox; Pfizer) (15 mg/kg, SC) and dexamethasone (Duphacort; Azium) (0.1 mg/kg, SC) wereadministered and the cat was referred for further diagnostic investigation.

(a) Pre-operative dorsoventral thoracic radiograph. The left lung lobes appear consolidated, and there is shifting of the mediastinum and cardiac silhouette to the left. The right caudal lung lobes are hyper-inflated consistent with the chronicity of the left pulmonary collapse. A patchy mixed (alveolar and interstitial) infiltrate is observed in the right cranial and middle lung lobes. (b) Pre-operative lateral thoracic radiograph demonstrating diffuse cranial thoracic opacity can be seen cranial to the cardiac silhouette.
At presentation, 7 days after the onset of clinical signs, similar findings were identified on clinical examination, and repeat conscious thoracic radiography. In addition the cat appeared mildly dehydrated. Abdominal radiography was unremarkable. Results of complete blood count and serum biochemistry are shown in Table 1. The only haematological abnormalities identified were a leukocytosis, characterised by a neutrophilia with left shift and a small number showing toxic changes, and lymphopenia, suggestive of an inflammatory process. Serum biochemistry changes included elevation of chloride, albumin and total protein levels, suggestive of dehydration. Intravenous fluid therapy with a balanced electrolyte solution (Hartmann's Solution; Aquapharm No. 11) (10 ml/kg/h IV) was initiated.
Haematology abnormalities associated with mitoxantrone administration following pneumonectomy for treatment of a pulmonary adenocarcinoma (chemotherapy dose given after haematology results obtained)

An ultrasound scan and ultrasound guided fine needle aspirate of the left cranial lung was performed at the fourth intercostal space, midway between the dorsum and ventrum. Consolidation of both left lung lobes, with no evidence of torsion or pleural effusion, was observed on the ultrasound scan. Microscopic examination of the smear identified a mixed population of inflammatory cells, and clumps of ciliated epithelial cells (Mayer-Grunwald Giemsa). No mycobacteria were identified with Ziehl-Neilson staining. The primary differential diagnoses for the left-sided pulmonary collapse at this point were primary neoplasia, bacterial pneumonia, foreign body inhalation and lung lobe torsion.
Anaesthesia was induced with intravenous propofol (Rapinovet; Schering-Plough Animal Health) (7 mg/kg, IV) and maintained with isoflurane (Isoflurane-RM; Rhone Merieux) administered via a cuffed endotracheal tube and Ayres T-piece circuit. Analgesia was maintained by the administration of fentanyl (Sublimaze; Jansen Ltd) (2 μg/kg, IM) at induction and every 20 min for 2 h thereafter, and bupivicaine (Marcain; Astra Pharmaceuticals) (0.5 mg/kg, per site) at the fourth, fifth and sixth intercostal spaces, after anaesthetic induction. Antibiosis was provided by enrofloxacin (Baytril; Bayer) (5 mg/kg, SC) administration at induction.
The endotracheal tube was removed and a 3.0 mm flexible bronchoscope introduced into the trachea. Effective visualisation was prevented by mucopurulent exudate at the level of the carina, so the cat was re-intubated. The aetiology of the left lung lobe consolidation could not be determined, but given the likely chronicity (as indicated by the compensatory hyperinflation of the right lung lobes) and irreversibility of the collapse, a left-sided pneumonectomy was performed to treat the cat's symptoms and allow diagnostic histopathology.
An exploratory intercostal thoracotomy was performed at the left fifth intercostal space. Manual positive pressure ventilation was initiated from the start of the thoracotomy procedure, until the end of surgery. No effusion was observed in the left thoracic cavity. The left cranial and caudal lung lobes were collapsed, with patchy irregular surfaces. Left pneumonectomy was performed by individually ligating the pulmonary artery, veins and bronchus with doubled simple interrupted 1.5 M polypropylene (Prolene; Ethicon) sutures. The tracheobronchial lymph nodes were not detected at surgery. The lung lobes were submitted for histopathology and bacteriology.
The thorax was lavaged with 1l of sterile saline (0.9%). A French 12-gauge thoracotomy tube (12G PCV chest drain; SIMS Portex), was placed through the left 10th intercostal space, and the thoracotomy was closed in a standard manner. Suction of the thoracotomy tube was performed every 2 h for 20 h. Between 1.5 and 4 ml of serosanginous fluid was obtained each time. Although the rate of fluid production was greater than that usually associated with the presence of a thoracic drain (2–4 ml/kg/24 h) the tube was removed as there was no active haemorrhage or air leakage.
Intrapleural analgesia was provided by bupivicaine (5 mg) instillation in the left pleural cavity through the thoracotomy tube, every 8 h. Further analgesia was provided with morphine (Morphine; Martindale Pharmaceuticals) (0.35 mg, IM, every 6 h for 24 h) from 6 h postoperatively. Oral enrofloxacin (5 mg/kg, sid for 14 days) and meloxicam (0.1 mg/kg, sid for 5 days) were administered from 24 h postoperatively. The cat made an unremarkable recovery from surgery, and was discharged 3 days postoperatively.
Histological sections of the affected lungs identified a well-differentiated acinar adenocarcinoma. The acini were filled with degenerate inflammatory and epithelial cells. Surgical margins were not obtained on the histological sections evaluated. No bacteria were cultured from the lung sections. Adjuvant chemotherapy with mitoxantrone (5 mg/m2, every 3 weeks) was initiated 16 days postoperatively. Complete blood counts were performed before the administration of each chemotherapy cycle.
On day 58 postoperatively (3 weeks after the second dose of mitoxantrone), a reduction in the neutrophil count (though within normal limits) was identified (Table 1), so the dose of mitoxantrone was reduced (3.75 mg/m2, IV). On day 79 the cat developed leukopenia and a further reduction in the neutrophil count (Table 1), so chemotherapy was temporarily stopped. A complete blood count on day 98 was normal (Table 1), so mitoxantrone therapy was restarted at the original dose (5 mg/m2, every 3 weeks). A reduction in the neutrophil count (though within normal limits) was observed on day 140, 3 weeks after the fifth injection(Table 1), so the dose of mitoxantrone was again reduced (3.75 mg/m2, IV). Subsequent complete blood counts were normal, so normal dosage levels and intervals were resumed.
At no point during chemotherapy was any toxicity, other than mild myelosuppression, detected. Chemotherapy was stopped after the 10th dose. No abnormalities of the right lung lobes were observed on conscious thoracic radiographs performed 2 weeks after surgery, and no changes were observed on further thoracic radiographs 5, 8, 11, 14, 17, 23 and 29 (Fig. 2) months postoperatively. Four small (<4 mm) peripheral round radiodense pulmonary opacities were identified onradiographs taken 17 months postoperatively. The cat was anaesthetised as described earlier and a computerised tomography scan of the thoracic cavity performed. No lesions were identified within the pulmonary parenchyma, and the perihilar lymph nodes could not de identified, suggesting that lymphadenopathy was not present. The nodules were assumed to be temporary obstruction of bronchi secondary to mucus plugging, which spontaneously resolved without treatment.
(a) Twenty-four month postoperative lateral thoracic radiograph. The lung appears hyperinflated. (b) Twenty-four month postoperative dorsoventral thoracic radiograph. The cardiac shadow is deviated to the left. Both the cranial and caudal right lung lobes appear hyper-inflated, and have further expanded to encompass the left thoracic dead space. The right cranial and middle lung lobes appear normal.
Discussion
Primary lung tumours are rare in the cat, with an estimated annual incidence of 2.2 per 100,000 cats (Theilen and Madewell, 1979). Primary pulmonary neoplasia is a disease of older cats, with a mean age of 11 to 12 years (Barr et al., 1987). The most common presenting signs are coughing, exercise intolerance, tachypnoea and/or dyspnoea (Hahn and McEntree, 1997). Although not present in this case, hypertrophic osteodystrophy has been noted in between 5% and 25% of cases (Barr et al., 1987; Hahn and McEntree, 1997). In previous case series most commonly all lung lobes are infiltrated with tumours (as assessed radiographically) and pleural effusion may be present in between 35%–65% of cases (Barr et al., 1987; Mehlhaff and Mooney, 1985). Digital metastasis of bronchial carcinomas is also recognised as an uncommon cause of lameness in older cats, also known as ‘lung-digit syndrome’, which carries an extremely poor prognosis (Gottfried et al., 2000).
Definitive diagnosis was made on histological examination of the neoplastic tissue, but was indicated by cytological examination of samples obtained by needle aspiration and tracheoscopy. The presence of clumps of ciliated epithelial cells was strongly suggestive of a well differentiated pulmonary carcinoma, in view of the pre-operative radiological findings. Proper staging of the tumour (lymph node staging) was not performed as they were not identified during surgery. Histological classification of the tumour in this case was a well-differentiated pulmonary adenocarcinoma. Further classification was made on the site of origin (bronchial or alveolar) or histological features(pillary, acinar, alveolar or solid) (Dungworthet al., 2000; Moulton et al., 1981). The adenocarcinoma was acinar in appearance, and alveolar in origin. Bronchial adenocarcinomas are the most commonly diagnosed primary lung tumour in cats in the series published by Hahn and McEntree (1997), where as alveolar adenocarcinomas were most commonly diagnosed in a series by Carpenter et al. (1987).
Radiography demonstrated an increase in pulmonary interstitial markings and pulmonary consolidation. The mixed pattern in the right lung lobes could have represented tumour spread. The owner was warned of this pre-operatively, and elected for surgery. The disappearance of this pattern 2 weeks postoperatively suggests it may have represented secondary bacterial infection, or consolidation secondary to exudate aspiration.
The longstanding appearance of the left lung collapse indicated that re-inflation was unlikely, regardless of the cause, so pneumonectomy was chosen as the method of diagnosis and treatment. Tumour staging should have been performed in this case, by the needle aspiration or biopsy of the bronchial lymph nodes, and abdominal ultrasonography. Between 50 and 75% of feline patients presenting with primary pulmonary neoplasia were not candidates for surgical resection, either because of extensive pulmonary disease or the presence of metastatic disease (Hahn and McEntree, 1997; Mehlhaff and Mooney, 1985).
Mitoxantrone is an antitumour antibiotic. Mitoxantone has shown anti-proliferative affects against mammary adenocarcinoma lines in vitro (Muleya et al., 1999), and against a limited number of feline carcinomas in vivo (Ogilvie et al., 1993). A number of toxic effects have been observed such as vomiting, diarrhoea, anorexia, and myelosuppression in cats given mitoxantrone (Ogilvie et al., 1993). In this case, only mild myelosuppression occurred, and resolved with a temporary reduction in dose or dosing interval, and no clinical effects were associated. The dosing regime changes were undertaken to minimise the risk of complications, however, the dosing reductions and delays were probably unwarranted in this case on the basis of low, but normal, neutrophil counts. This may have reduced the effectiveness of the chemotherapeutic regime.
In one study, all cases of feline pulmonarycarcinoma's which underwent surgical removal of the primary tumour died of metastasis (Hahn and McEntree, 1998). Mitoxantrone was used as an adjuvant to surgical resection in this case to provide long-term control of residual local disease and any distant metastasis.
The prognosis for long-term survival with pulmonary adenocarcinoma has been reported to be poor (Barr et al., 1987). The only prognostic factor associated with survival in cats with primary pulmonary neoplasia was the degree of differentiation of the tumour (Hahn and McEntree, 1998). Cats with moderately differentiated tumours survived a median 698 days (19–1526 days) compared to cats with poorly differentiated tumours 75 days (13–634 days), though all cats eventually died of metastatic disease. The overall median survival time in cats (115 days, Hahn and McEntree, 1998) is similar to that in dogs (120 days, Ogilvie et al., 1989).
In humans with non-small cell lung carcinoma surgery has provided the best chance of cure. When patients have been unable to tolerate surgicalresection primary radiotherapy has been offered to patients with limited locoregional disease. Radiotherapy has also been used as an adjuvant to surgery where local disease control has not been achieved. Historically the role of chemotherapy had been to treat metastasis but it is now also used adjuvantly and in a palliative setting with or without radiotherapy (Ginsberg et al., 2001).
Combination chemotherapy has generally been associated with higher response rates than single agent therapy but it is less clear if this translates to prolonged survival. Platinum cytotoxics such as cisplatin or carboplatin have been the most frequently used agents and as single agents have about a 10% response rate but response rates to single agent epirubicin have been comparible. Mitoxantrone has not been extensively evaluated for human non-small cell lung carcinoma but Suga et al. (1986)failed to identify any responses in 24 patients treated with mitoxantrone as a single agent. Newer agents including taxanes, gemcitabine, irinotecan, and vinorelbine have reproducible single-agent activity of 15% to 25% and are now involved in most ongoing clinical trials (Ginsberg et al., 2001)
Therapeutic improvements achieved with these newer cytotoxics appear to have now reached a plateau. New therapeutic strategies for human non-small cell lung carcinoma include drugs targeted against epidermal growth factor receptor, signal transduction, angiogenesis, and cyclo-oxygenase-2 as well as gene therapy (Cappuzzoet al., 2003).
In veterinary medicine the treatment of choice for both canine (Mehlhaff et al., 1984; Ogilvieet al., 1989) and feline (Hahn and McEntree, 1998) pulmonary carcinoma has been surgical resection.
To the authors' knowledge there are no reports of radiotherapy in any therapeutic setting for feline pulmonary carcinoma. The best results with radiotherapy for human non-small cell lung carcinoma are achieved with three-dimensional conformal radiotherapy with a high fractionation schedule. Use of suboptimal radiotherapy carries an increased risk of pulmonary, oesophageal, cardiac, and neurologic toxicity (Ginsberg et al., 2001). Veterinary radiotherapy facilities are geographically limited in the United Kingdom, fractionation schedules are by necessity coarse in comparison to those used in humans, three-dimensional conformal radiotherapy is unavailable, and the risks of toxicity were considered unacceptable by the cat's owners. For all of these reasons, adjuvant radiotherapy was not pursued in this case.
There is only one report of the use of chemotherapy in any clinical setting to treat pulmonary adenocarcinoma in cats, to the authors' knowledge (Ogilvie et al., 1993). Chemotherapy with vindesine and/or cisplatin has been described in a small number of dogs with pulmonary carcinoma(Mehlhaff et al., 1984). Vinorelbine is currently being evaluated as a single agent in dogs with pulmonary carcinoma (Argyle, D.J. personal communication 2003). Inhalation chemotherapy with paclitaxel or doxorubicin has also been reported in dogs (Hershey et al., 1999).
The lack of published information in cats, and in particular, a complete lack of phase II or III clinical trials, makes it impossible to draw firm conclusions as to the effectiveness of chemotherapy against feline pulmonary carcinoma generally or to recommend any individual cytotoxics. However, the high risk of eventual postoperative tumour recurrence in published feline studies (Hahn and McEntree, 1998) and, in this particular case, the intra-operative extent of tumour and the histopathological findings prompted us to recommend some form of adjuvant chemotherapy.
In cats, there have been no peer reviewed reports of the use of taxanes, gemcitabine, irinotecan, or vinorelbine for the treatment of tumours (Moore and Kitchell, 2003), and their use was not considered further. Cytotoxics consideredincluded: mitoxantrone, epirubicin, and carboplatin. Epirubicin is a potent vesicant if injected perivascularly and has been associated with severe loss of appetite in up to a quarter of cats at recommended dosages (Kristal et al., 2001; O'Keefeet al., 1993). The dose-limiting toxicity of carboplatin in cats is neutropenia, which can be profound (<1×109/l) in a third of cats at the recommended dose of 200 mg/m2(Bailey et al., 2003; Hahn et al., 1997). Mitoxantrone is not a vesicant and is associated with less clinical toxicity than epirubicin or carboplatin (Ogilvie et al., 1993).
The owner's concerns centred on the cat's quality of life whilst receiving chemotherapy. An additional consideration was that much of theongoing care, including cytotoxic administration, was to be carried out by the referring veterinary surgeon rather than at GUVS, for geographical reasons. As a result we decided to pursue single agent therapy mitoxantrone therapy in this case despite the poor response rate reported in humans with non-small cell lung carcinoma.
The cat in this case had survived 1040 days at the time of writing, with no evidence of metastatic disease. Pneumonectomy resolved the signs associated with pulmonary neoplasia in this case. Tumour recurrence may still occur with further follow up, and a single case report cannot assess the value of adjuvant chemotherapy. However, no clinically significant side effects occurred and further evaluation of its use in cats with pulmonary adenocarcinoma is warranted. Additionally, left-sided pneumonectomy was straightforwardly performed through an intercostal approach, avoiding the morbidity associated with median sternotomy (Hahn and McEntree, 1998).