
Abstract
In this retrospective study of 22 cats with lower airway disease of either intermittent (23%) or persistent nature (77%), the Siamese breed (55%) was significantly over-represented. Females (68%) were slightly but not significantly over-represented. No significant association was found between the clinical stage of disease and the physical findings, thoracic radiographic changes or the response to treatment. Cough, the most common presenting complaint, was the only symptom detected in the cats with intermittent disease, yet the two most severely affected animals did not show it. Thoracic auscultation did not reveal any abnormality in 41% of the cats. Haematology revealed eosinophilia in 46% of the cats. A bronchial pattern was the most common radiographic abnormality (73%), followed by alveolar (32%) and interstitial patterns (23%). Interestingly, thoracic radiographs were normal in 23% of the cats. The combination of short-term corticosteroids and bronchodilators resulted in complete and long-term remission of symptoms in nine cats, while the other 11 required ongoing medication because of relatively frequent relapses. One of the remaining two cats died during an asthmatic crisis, while the other was lost to follow up.
Introduction
Chronic bronchitis, asthmatic bronchitis, bronchial asthma, allergic bronchitis (Henik and Yeager, 1994) and acute bronchitis (Moise et al., 1989) are terms that have been used interchangeably to describe feline lower airway disease (FLAD) (Dye, 1992; Dye and Moise, 1992). This is an encompassing term representing a group of respiratory disorders of different aetiologies (Corcoran et al., 1995; Henik and Yeager, 1994), of which the most important is chronic bronchitis. However, its differentiation from true asthma is at best difficult, even with the aid of bronchoscopy, bronchoalveolar lavage cytology, bacterial culture and pulmonary function testing (Sparkes, 2002). Feline asthma, also reported in captive African lions (Mukherjee et al., 1999), shares many similarities with the relevant human disease (Padrid, 2000a). Clinically, FLAD is characterized by persistent, intermittent or episodic coughing, wheezing or respiratory distress of sudden or gradual onset (Corcoran et al., 1995; Dye et al., 1996; Moise et al., 1989). In some cats, predominance of coughing over wheezing, and visa versa, is regularly seen (Sparkes, 2002). Current treatment protocols include bronchodilators and corticosteroids appearing in various formulations (metered dose inhalers, oral, parenteral) and dosages (Padrid, 2000a).
The primary purpose of this study was to investigate any possible correlation between the clinical stage of the natural disease and its clinical picture, associated thoracic radiographic changes and the response to treatment. Moreover, our intention was to provide additional clinically relevant information on FLAD by retrospectively reviewing 22 naturally occurring cases.
Materials and methods
Twenty-two cats were selected from a total of 188, which had been admitted to the Clinic of Companion Animal Medicine, School of Veterinary Medicine, Aristotle University of Thessaloniki, Greece, with various respiratory problems between February 1992 and 1999. The criteria for entry into the study included coughing, dyspnoea or wheezing, which responded promptly to corticosteroids and bronchodilators, absence of concurrent upper respiratory tract disease, cardiovascular, pleural space or mediastinal disease and current vaccinations against herpesvirus, calicivirus or chlamydophila infections.
On admission a thorough physical and cardiopulmonary examination followed history taking. The clinical staging of disease was based first on the intermittent or persistent appearance of the signs; the latter were further characterized as mild, moderate or severe (Padrid, 2000a).
In all 22 cats, faecal examination for respiratory tract pulmonary parasites was performed by direct smear and flotation techniques (Baermann, Teleman, Faust). Also, a complete blood count with an electronic cell counter (MS9, Rhône Mérieux, France) and a manual differential leukocyte count were carried out. Plasma total solids were measured by refractometry (American Optical Refractometer). Right lateral and ventrodorsal thoracic radiographs were blindly evaluated by one of the authors (MP). Changes in the pulmonary parenchyma, as well as in the cardiovascular structures were evaluated. Treatment was instituted in all 22 cats, with follow-up possible in 21.
Statistical analysis
The homogeneity of the breed and gender distribution was compared between the cats of the study and those of the general hospital population, for the same period of time, by Pearson's χ2 test. Fisher's exact test was used for the comparisons between the clinical stage of FLAD and the respiratory signs, thoracic radiographic changes and the outcome of the disease. In every instance, a P value ≤ 0.05 was considered to be significant.
Results
Historical and clinical findings
Nine cats were DSH (41%), 12 were Siamese (55%) and 1 was Persian (4%). This population included 15 female (68%) and 7 male cats (32%), of which 10 (46%) had been neutered. On admission, the age of the animals ranged from 1.5 to 11 years (median: 5.5 years) and their body weight from 2 to 6 kg (median: 4.15 kg). Two cats (9%) were overweight and only 6 (27%) were dewormed on a regular basis. The animals were fed commercial diets (11/22, 50%), homemade diets (1/22, 4%) or a combination of commercial and homemade diets (10/22, 46%). Thirteen of the cats (59%) had an exclusively indoor lifestyle, while the rest (9/22, 41%) were indoor/outdoor cats.
Statistical analysis showed that only the Siamese breed were at increased risk (P = 0.018) for developing FLAD. There was a trend of female cats to be over-represented, but this just failed to reach statistical significance (P = 0.08).
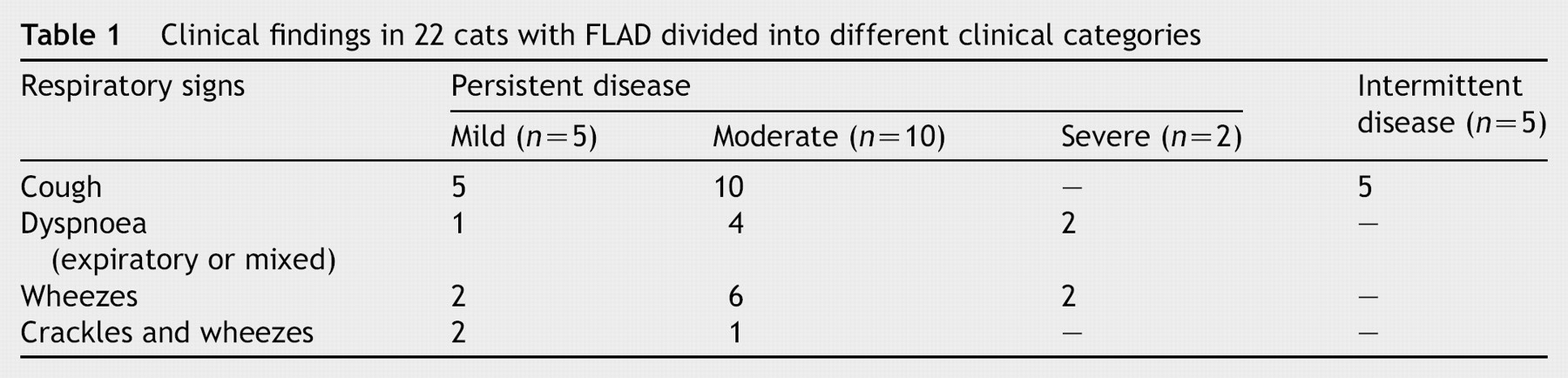
According to the history and the results of the clinical examination 5/22 (23%) of the animals had intermittent and 17/22 (77%) had persistent symptoms; the latter were further characterized as mild, moderate or severe in 5/17 (29%), 10/17 (59%) and 2/17 (12%) cats, respectively. Coughing was reported in 20 cats (91%), dyspnoea, mainly expiratory, in 7 cats (32%) of which 5 also experienced coughing paroxysms. On thoracic auscultation, wheezing was detected in 10 animals (46%), while only in 3 (14%) could a mixture of wheezing and crackling sounds be heard. Interestingly, in 9/22 cats (41%) thoracic auscultation revealed no abnormalities. Two of the animals were presented in a state of severe respiratory distress exhibiting an anxious expression, open mouth breathing, hypersalivation, orthopnoeic stance and cyanosis. No significant association was found in any of the possible statistical comparisons made between the respiratory symptoms and clinical stage of the disease (Table 1).
Clinical findings in 22 cats with FLAD divided into different clinical categories
Laboratory findings
No ova or larvae of respiratory or any other kind of endoparasites were found in the faecal examination of any of the 22 cats. Haematology, on the other hand, revealed mild polycythemia (PCV: 47%) in 1/22 cat (4%), eosinophilia (>1500/μl) in 10/22 (46%) and hyperproteinaemia (>8 g/dl) in 3 cats (14%).
Radiographic findings
A bronchial pattern was recognized in 16/22 cats (73%), an alveolar pattern in 7/22 animals (32%), and an interstitial pattern in 5/22 cats (23%) (Fig. 1). Flattening of the diaphragm together with lung overinflation (4/22, 18%) and atelectasis of the right middle lung lobe (1/22, 4%) were additional findings (Fig. 2). Right-sided cardiomegaly or bronchiectasis could not be detected in any of the cats. Interestingly, the thoracic radiographs appeared normal in 5/22 cats (23%). When analyzed statistically, all the comparisons made between the radiographic appearance of the thorax and the clinical stage of disease were not correlated (Table 2).

Right lateral thoracic radiograph of an 11-year-old Siamese cat admitted with severe lower airway disease (asthmatic crisis). Note the widespread, mild to moderate bronchial markings in the pulmonary parenchyma and the flattening of the diaphragm attributable to lung overinflation and aerophagia.

Ventrodorsal thoracic radiograph of a 2-year-old DSH cat also admitted with severe lower airway disease (asthmatic crisis), showing a moderate bronchial and interstitial pattern in the cranial and middle lung lobes, as well as consolidation (atelectasis) of the right middle lung lobe.
Thoracic radiographic findings in 22 cats with FLAD divided into different clinical categories

Response to therapy
The two cats with severe respiratory distress were immediately put into an oxygen cage (60% inspired concentration), following administration of methylprednisolone sodium succinate (Solu-Medrol inj, Upjohn; 30 mg/kg, im) and aminophylline (Aminophylline inj, Cooper; 4 mg/kg, im). One cat initially responded satisfactorily within the 30 min only to relapse 2 h later. The same protocol was again applied, with the same results. Soon after the stabilization of the animal's condition, it was discharged on oral prednisolone (Prezolon tab, Nycomed; 2 mg/kg, divided BID) and sustained-release theophylline (Theo-Dur s.r. tab, Lavipharm Hellas; 25 mg/kg SID, in the evening) for the next 3 weeks. Since then, this animal has relapsed every 2 to 3 months but with milder symptoms. The other severely affected cat, did not respond, and was therefore given atropine sulphate (Atropine Sulphate inj, Elvipi; 0.04 mg/kg, im) and adrenaline (Adrenaline inj, Elvipi; 20 μg/kg, im) with dramatic improvement evident within 15 min. Methylprednisolone sodium succinate and atropine sulphate were continued every 6 to 8 h for the next 3 days, when medication was changed to oral prednisolone and theophylline. Fifteen days later, however, it was readmitted in a critical condition and died very soon thereafter.
Treatment was also attempted in the remaining 20 cats with follow-up available for 19. Therapy was based on corticosteroids, either oral (prednisolone; 2 mg/kg, divided BID and tapered gradually) or parenteral (methylprednisolone acetate; Depo-medrol inj, Upjohn; 20 mg/cat/2–3 weeks, im), and oral bronchodilators such as slow-releasing theophylline or terbutaline (Dracanyl tab, Astra; 1.25 mg/cat BID) given for a period extending from 2 to 4 weeks, at least from the outset. Nine of the 19 cats (47%) have subsequently become asymptomatic, while the rest (10/19, 53%) continue to relapse every 3 to 6 months. No prediction could be made on outcome based on clinical staging (Table 3).
Outcome in 21 cats with FLAD

Discussion
Today, the term “feline asthma” is accepted broadly (Padrid, 2000a) as it has been established that cats develop asthma similar to that of humans (Padrid, 2000a; Sparkes, 2002). However, the terms FLAD and chronic bronchial disease appear more appropriate since they can include both asthma and chronic bronchitis (Sparkes, 2002). These two conditions may demand a different therapeutic approach and have different prognoses (Padrid, 2000b). As it was impossible to make a clear distinction between them, the collective term FLAD has been used instead. Ideally, bronchoscopy, cultures for Mycoplasma spp., anaerobes and other bacteria, pulmonary function tests, allergy testing, and provocative airway challenge exposure should have been pursued in an attempt to differentiate these two conditions (Dye and Moise, 1992; Moise et al., 1989; Padrid, 2000a). The main underlying pathology of this airway obstructive syndrome is bronchial mucosa inflammation, excessive mucus secretion and smooth muscle hypertrophy and constriction (Dye and Moise, 1992; Henik and Yeager, 1994; Padrid, 2000b), which explains the characteristic clinical triad of coughing, expiratory wheezing and dyspnoea, all appearing in various combinations and degrees as seen in our case series.
Siamese (Moise et al., 1989) and Himalayan cats (Noone, 1986) are at increased risk for developing FLAD, most likely due to a genetic susceptibility (Padrid, 2000a). This observation was further confirmed in this study by comparing the number of Siamese cats (12/22) with that (284/957) of our feline hospital population admitted over the same period of time. Siamese cats may also present a more protracted form of FLAD (Dye et al., 1996; Moise et al., 1989), albeit this could not be confirmed in this study since only 5 out of 12 cats (42%) belonging to this breed were actually relapsing cases.
Although, the majority of our cats (68%) were female, as it had been witnessed in a similar study (Moise et al., 1989), taking into consideration the general hospital population a significant predisposition could not be found. In contrast, while Corcoran et al. (1995) did not find any gender predisposition, Dye et al. (1996)noticed an over-representation of male cats. Since almost half of the cats (46%) were either spayed or castrated, it is difficult to attribute neutering as a predisposing factor in contrast to what was suggested in a similar study (Corcoran et al., 1995). The age range of the cats was similar to that of other reports (Corcoran et al., 1995; Dye et al., 1996; Moise et al., 1989), emphasizing that FLAD is an age-independent disease. Cats with FLAD tend to limit their activity, which may result in obesity (Johnson, 1997), so it is not necessarily considered a predisposing factor. However, our two overweight cats had been overweight long before the appearance of respiratory symptoms.
Since feline lung parasites (Paragonimus kellicotti, Aelurostrongylus abstrusus, Eucoleus aerophilla) and Dirofilaria immitis infestation may mimic feline asthma, faecal examinations were performed (Dye, 1992; Forrester, 1990; Johnson, 1997; Noone, 1986) and showed that lung parasites were not implicated. Unfortunately, none of the animals was parasitologically checked for D. immitis infestation, but their thoracic radiography did not show vascular changes indicative of heartworm disease (Snyder et al., 2000).
None of the cats was fed exclusively with fish-based diets (commercial or homemade), dispelling the theory that the high histamine levels of these diets would initiate or exacerbate the clinical disease (Henik and Yeager, 1994) in these patients.
In this study, coughing, either alone or accompanying with other signs, was the most common complaint (20/22, 91%). Similar observations have been made by other investigators (Dye et al., 1996; Moise et al., 1989), while Corcoran et al. (1995) reported that affected cats may exhibit cough or dyspnoea in a roughly equal proportion. Only two of the 22 cats (9%) were presented in an asthmatic crisis, reminiscent clinically, of marked pleural effusion (Fossum and Relford, 1994). Despite the lack of significance, it is interesting to note that the two cats with asthmatic crisis had not had any coughing episodes in contrast to those with the intermittent disease (n = 5), which presented with only this symptom. Abnormal respiratory sounds were heard on thoracic auscultation in 13/22 cats (59%) included wheezes and crackles; both sounds were detected in three cats and wheezes only in ten. Surprisingly, in nine animals (41%) no abnormal sounds could be heard, a higher figure than has been reported previously (Corcoran et al., 1995; Moise et al., 1989). It is true, though, that several cats with FLAD appear normal on pulmonary auscultation (Johnson, 1997).
Thoracic radiographs revealed no abnormalities in 5/22 cats (23%). Thus a negative result does not eliminate FLAD from the list of diagnostic possibilities (Corcoran et al., 1995; Forrester, 1990; Johnson, 1997; Padrid, 2000b). A bronchial pattern has been reported as being the most common pattern (Dye and Moise, 1992; Henik and Yeager, 1994; Johnson, 1997), and was seen in 16/22 (73%) of the cats, while alveolar and interstitial patterns were recognized less frequently (32%, 23%, respectively). Atelectasis of the right middle lung lobe was seen in only one cat (4%), although, figures as high as 10% have been reported by Dye and Moise (1992) for this change. Lung overinflation and flattening of the diaphragm, on the other hand, were noticed as concomitant changes in 4/22 of the animals (18%), a slightly higher figure than that of the aforementioned report (Dye and Moise, 1992). The absence of significant correlations between the clinical features and radiographic changes in FLAD were not surprising since similar comparisons in human asthma patients (Park et al., 1997; Gillies et al., 1980) did not show any positive correlation, either.
Ten out of 22 cases (46%) showed peripheral eosinophilia, which varies widely in FLAD cases (Forrester, 1990; Moses and Spaulding, 1985) and may not correlate with airway eosinophilia (Corcoran et al., 1995; Moise et al., 1989). Hyperproteinaemia, noted in three cats (14%) is a rather usual finding (Dye et al., 1996; Moise et al., 1989) that could be associated with either chronic immune stimulation or haemoconcentration (Johnson, 1997).
Oxygen supplementation, along with a parenteral short acting corticosteroid and bronchodilator administered to the two severely affected cats are considered the standard method of treating an asthmatic crisis (Henik and Yeager, 1994; Johnson, 1997). In the non-responding cat to which atropine and adrenaline had to be given, there was a marked improvement, thus validating their use as rescue drugs. The long-term use of atropine should be avoided however, because it increases the viscosity of mucus causing further airway narrowing and airflow reduction (Mazzaffero, 2001). Currently, improved results have been obtained in our hospital with metered dose inhalers containing salbutamol administered with the aid of a paediatric spacer device (Padrid, 2000a).
In the 20 chronically treated cats a combination of corticosteroids and bronchodilators was used with relatively good results. Obviously, combination therapy did not make it possible to access the role each medication may have played in the context of the clinical improvement observed. Interestingly, nine animals remained asymptomatic long after they were weaned off anti-inflammatory and bronchodilatory medications, although for the first 6 to 8 months these animals relapsed intermittently. Since the role of treatment in the cure of asthma remains uncertain, it seems that these cats (9/19, 47%) may have outgrown the disease, at least clinically, perhaps the same way almost half of the children with asthma do (Gerritsen, 2002). Notably, one of these cats became permanently asymptomatic only when the owner moved to another city, suggesting a hypersensitivity to a local aeroallergen as the underlying aetiology. Of the remaining ten cats still requiring medication, environmental avoidance, use of an alternate litter and a 10-week dietary elimination trial was attempted by an owner only, although this cat unfortunately relapsed indefinitely. Although a positive correlation was anticipated between the severity or the persistent/intermittent course and the outcome of the disease in the 21 cats with follow-up, such an association could not be demonstrated statistically.