
Abstract
A 7-year-old cat was presented initially with multiple draining sinuses on the metatarsal region of its right hindlimb. Another lesion had appeared at the same time on the fifth proximal interphalangeal joint of the left forelimb. Histopathological examination of a biopsy from the right hindlimb lesion revealed chronic pyogranulomatous inflammation associated with yeast-like bodies and septate mycelia; a fungus was cultured on conventional media but not identified further. Culture of a swab collected from the left forelimb lesion demonstrated a pigmented fungus, also not characterised further.
Although there was initially a favourable response to ketoconazole (Nizoral, Janssen-Cilag Pty. Ltd) and β-lactam therapy, the infection in the hind limb relapsed subsequently, and Fusarium chlamydosporum was cultured from deep biopsy specimens. Clinical improvement followed debridement and itraconazole (Sporanox, Janssen-Cilag Pty. Ltd; 100 mg orally once daily), however amputation of the limb represented the best chance for a cure. The cat made an uncomplicated recovery following surgery and remained well for five months until the lesion on the left forelimb recurred. Amputation of the distal fourth digit was then performed, and the resected tissue submitted for culture. The dematiaceous fungus Microsphaeropsis arundinis was subsequently cultured. The cat remained well for several months, until a further F. chlamydosporum infection developed on the body wall. This was excised 7 months ago, and no lesions have recurred in this area.
Importantly, this is the first reported case of M. arundinis infection in a mammalian host.
A 7-year-old, desexed male domestic short hair cat (4.6 kg) was presented with multiple draining sinuses on the dorsal and ventral metatarsal region of the right hind limb. It also had a focal abscess-like lesion on the left fifth proximal interphalangeal joint region. Empiric treatment with a variety of broad-spectrum antimicrobials including amoxicillin clavulanate (Clavulox, Pfizer; 62.5 mg orally twice daily) and cefadroxzil (Cefa-Tabs, Forte Dodge; 100 mg orally once daily) had little effect. A deep biopsy from the pelvic limb lesion was obtained under anaesthesia. Histology demonstrated chronic pyogranulomatous inflammation with yeast-like bodies and septate mycelia; a fungus was cultured on conventional media but not characterised further. Culture from a swab taken from the left forelimb lesion resulted in a light growth of a coagulase-positive Staphylococcus species (of dubious significance) and a moderate growth of a dematiaceous (pigmented) fungus that did not sporulate on conventional mycological media. Antibiotic therapy was continued and ketoconazole (50 mg orally twice daily) was added to the therapeutic regimen. The left forelimb lesion resolved completely, however there was only limited improvement in the appearance of the right metatarsus.
A second opinion was sought 2-years after initial presentation. The appearance of the distal hindlimb at that time is illustrated in Fig. 1. Results of routine haematology and biochemistry were unremarkable. Immunochromatography tests for FeLV antigen and FIV antibodies were negative. Additional tissue specimens were obtained under general anaesthesia by massaging the affected distal limb, thereby expressing deep representative material from the draining sinus tracts for laboratory investigations. Potassium hydroxide preparations revealed branching, non-pigmented, septate hyphae of uniform width. Crush preparations stained with DiffQuik demonstrated hyphae, macrophages, giant cells and occasional neutrophils (Fig. 2). Pink/orange fungal colonies were observed after 72 to 96 h incubation at 28 °C on Sabouraud's dextrose agar containing gentamicin and chloramphenicol. The plates were subsequently forwarded to a reference laboratory where the organism was identified as Fusarium chlamydosporum. Susceptibility testing was not performed due to the isolate's slow growth habit.

Appearance of the right metatarsal region two-years after initial investigation (prior to itraconazole therapy). Before (a) and after (b) debridement. Note the numerous draining sinus tracts. Two of these are indicated by arrows.
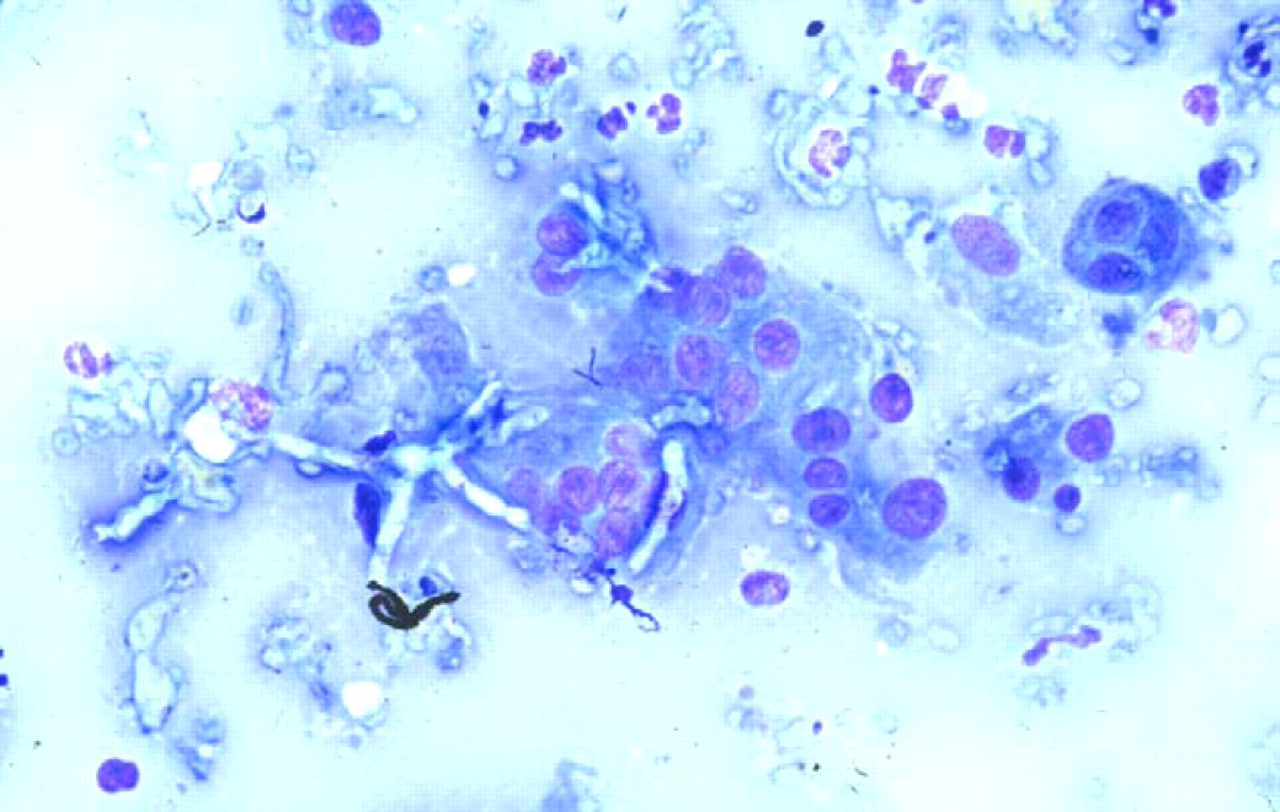
Cytological appearance of F. chlamydosporum. Note the fairly wide branching septate hyphae surrounded by numerous macrophages. DiffQuik original magnification; ×132.
Therapy using itraconazole (100 mg orally once daily) and topical silver sulphadiazine cream (Silvazine; Smith and Nephew) was commenced, following debridement of the affected foot. The foot was subsequently bandaged and cleaned with saline every three to four days. Improvement in the lesions was evident after 14 days (Fig. 3), however despite antifungal therapy draining sinuses reappeared six-weeks later. At this time the reference laboratory reported the precise aetiology of the infection. Review of published information on Fusarium disease in human patients suggested that in general these infections are resistant to antifungal agents both in vitro and in vivo. Thus, we considered that the best chance of permanently eliminating the infection was by amputation of all infected tissues with a wide surgical margin. This decision was influenced in part by financial limitations, which precluded the alternative approach of aggressive surgical debridement followed by a long course of antifungal therapy using agents with reported efficacy against Fusarium spp., such as amphotericin B or voriconazole (Pujol et al., 1997; Reis et al., 2000).

Appearance of the right metatarsal lesion after three weeks of itraconazole therapy. Note the slight improvement in the draining sinuses. Two of these are indicated by arrows.
Histological findings in tissues of the amputated limb were consistent with an invasive mycotic infection. Epidermal ulceration and areas of orthokeratotic hyperkeratosis were present. The underlying dermis had been effaced by large areas of granulomatous to pyogranulomatous inflammation, with sheets of macrophages, giant cells, isolated neutrophils and scattered lymphoid and plasma cells. Silver and periodic acid Schiff (PAS) stained sections demonstrated numerous small tangles of short branching fungal hyphae with a beaded appearance throughout the affected tissues (Figs. 4 and 5).

Microscopic appearance of the tissues infected by F. chlamydosporum. Note the numerous tangles of black hyphae surrounded by macrophages. Silver stain original magnification; ×330.

Microscopic appearance of the tissues infected by F. chlamydosporum. Note the pink stained hyphae in a large granuloma surrounded by a mass of macrophages. PAS original magnification; ×300.
Five-months following hindlimb amputation, the lesion on the left foreleg recurred (Fig. 6). Amputation of the affected digit from the distal end of the fifth metacarpal bone was performed, with the resected tissue submitted for laboratory investigations. DiffQuik-stained smears revealed wide septate hyphae and some ovoid structures (Fig. 7). Large grey/brown fluffy fungal colonies were cultured after three-days incubation at 28°C on Sabouraud's dextrose agar containing gentamicin and chloramphenicol. The organism was subsequently identified as Microsphaeropsis arundinis at a reference laboratory. Based on the previous favourable response, ketoconazole (50 mg orally twice daily for two months) was prescribed in concert with topical terbinafine (1%) cream (Lamisil; Novartis). Testing later suggested the isolate was susceptible to ketoconazole, itraconazole and amphotericin B, so terbinafine cream was discontinued.

Appearance of the recurrent lesion on the left paw (five-months following right pelvic limb amputation). Note the draining sinus tract (arrow).

Cytological appearance of M. arundinis. Note the wide septate fungal hyphae and the surrounding giant cells. DiffQuik original magnification; ×330.
Histological findings were again consistent with an invasive mycotic infection. Inflammatory changes were present from the hair follicles and deeper, consisting predominantly of epithelioid macrophages, with a moderate amount of lymphocytes and neutrophils. Occasional multinucleate macrophages were present. In other areas there are moderate amounts of plasma cells and even multinucleate plasma cells. PAS stained sections demonstrated fungal organisms with variable appearance, ranging from large spherical bodies to septate branched hyphae and chains of smaller yeast-like cells (Fig. 8).

Microscopic appearance of the tissues infected by M. arundinis. PAS original magnification; ×330.
No lesions have reappeared on the distal forelimb in nine-months following digital amputation. At this time, however, another lesion appeared on the right inguinal area adjacent to the pelvic limb amputation site. Subsequent culture of the tissue revealed F. chlamydosporum. A large excision was made around the affected tissue, and antifungal therapy recommenced. Itraconazole (100 mg once a day orally) was given for two–three weeks, then reduced to 50 mg once daily for three-months. Amphotericin B (Fungizone; Bristol-Myers Squibb Pharmaceuticals 5 mg/ml); 0.5 mg/kg diluted in 300 ml of 0.45% sodium chloride, 2.5% dextrose was given subcutaneously on two separate occasions, a week apart. A month following the surgery, no new lesions have recurred.
Discussion
Fusarium species are filamentous fungi found in soil and on plants and have a worldwide distribution. Infections with this agent are known to increase in prevalence during rainy seasons (Boutati and Anaissie, 1997). Fusarium spp. may give rise to hyalohyphomycosis, a term used to describe infections caused by moulds with unpigmented cell walls and branched or unbranched, light-coloured hyphal elements with a mycelial morphology (Vartivarian et al., 1993). Penicillium spp. and Scedosporium spp. are other major causes of hyalohyphomycosis, while infections caused by Aspergillus species are by tradition referred to as aspergillosis.
This case was remarkable because two distal lesions on different limbs were observed in the same patient, attributable to different, rare, saprophytic fungi. Fusarium spp. are a rare cause of human disease and have been reported in only a handful of small animal patients, while Microsphaeropsis spp. infections are very rare, even in the well-documented human mycology literature. Two different scenarios can be suggested to account for physical findings and clinical course observed in the present case. The less likely possibility, in our view, is that this cat suffered from some immunological defect, perhaps affecting inherited neutrophil function or cell mediated immunity, which rendered it at increased risk of developing opportunistic infections with saprophytic fungi normally of limited virulence. The reason why this seems unlikely is that both infections remained localised, and ran a persistent but indolent course, despite suboptimal initial therapy. A more likely scenario was that the cat received penetrating injuries of both distal limbs which were heavily contaminated by saprophytic fungi, either at the time of injury, or shortly thereafter. The number of fungal elements introduced was presumably sufficiently large to overwhelm the innate host immune response, resulting in progressive, locally invasive disease that was sufficiently constrained to prevent dissemination. Initial therapy with ketoconazole was sufficient to tip the host-parasite relationship in favour of the cat, with resolution of the forelimb lesion and improvement of the hindlimb infection, but therapy was insufficiently effective to permanently eliminate fungal cells from the host, ultimately resulting in progressive or recrudescent infection.
Fusarium spp. typically behave as opportunistic pathogens and rarely produce disease in healthy mammalian hosts in the absence of penetrating injury. In immunocompetent patients, Fusarium may produce localised disease following inoculation into susceptible sites. In contrast, immunocompromised hosts may develop severe local disease and/or disseminated infections. Elaboration of mycotoxins, production of specific enzymes and an innate ability to adhere to foreign bodies and synthetic prostheses contribute to the virulence of this organism.
Localised fusariosis results from a degree of local or systemic impairment of host defences, typically caused by a penetrating injury of the skin, for example by a foreign body (Nelson et al., 1994). Common sites of inoculation in human patients include the nail beds, cornea, joints and skin. Two forms of localised disease exist, an indolent form limited to the stratum corneum, and an aggressive form where hyphae reach subcutaneous tissues and thereby incite an immunologic response in the host (Pereiro et al., 1999). Fusarium spp. most commonly implicated in disease in human patients include F. solani (the most pathogenic), F. moniliforme (verticillioides) and F. oxysporum (Segal et al., 1998).
Disseminated fusariosis usually requires a substantial degree of underlying immunologic impairment resulting from conditions such as bone marrow failure, immunosuppressive drug therapy, hematological malignancies or HIV/AIDS (Guarro et al., 2000; Sampathkumar and Paya, 2001). For example, the first documented human case of fusariosis was in a 2½-year-old child being treated for acute leukemia who developed skin lesions, panophthalmia, subcutaneous abscesses and encephalitis due to F. solani (Cho et al., 1973). Even with appropriate antifungal drug therapy, recovery from Fusarium infections may require resolution of neutropenia (Segal et al., 1998).
There are very few reported instances of Fusarium infection in domestic animals and the species isolated from the present case, F. chlamydosporum, has not commonly been reported even from human patients (Segal et al., 1998). Topical miconazole treatment proved unsuccessful in a dog with a corneal Fusarium infection, which later required enucleation to effect a cure (Marlar et al., 1994).
Management of Fusarium spp. infections may involve either surgery and/or antifungal therapy. Localised disease can be cured by excision alone, however in neutropenic or immunocompromised patients, concurrent systemic therapy is mandatory. Ideal therapy typically consists of both wide surgical excision, when possible, followed by systemic antifungal therapy. Thus, for example, wide surgical excision followed by systemic antifungal therapy was successful in a case of localised Fusarium on the plantar aspect of the foot of a man undergoing bone marrow transplantation (Ellis et al., 1994). Specific antifungal agents available include amphotericin B (including liposomal and lipid complex formulations), terbinafine, natamycin, or the azoles (itraconazole, voriconazole and posaconazole). The current mainstay of treatment is amphotericin B used in combination with other agents (Pujol et al., 1997).
There appears to be little correlation between the in vitro activity of many antifungal agents against Fusarium spp. and their in vivo activity in the patient. Thus, predicting the response to therapy is often difficult. For example voriconazole has been to shown to have a poor activity in vitro (Marco et al., 1998), although systemic and topical application of this drug resulted in a full recovery from Fusarium keratitis in one patient (Reis et al., 2000). Voriconzole is approved for primary use in invasive aspergillosis and salvage therapy for serious fungal infections such as fusariosis. Fusarium spp. are intrinsically resistant to glucan synthesis inhibitors such as caspofungin, however in combination with amphotericin B, they might have a synergistic action (Arikin et al., 2000). The new azoles ravuconazole and posaconazole have been shown to have limited activity against Fusarium spp. in vitro, although posaconazole had efficacy in some experimental mouse models (Lozano-Chiu et al., 1999) and in a keratitis and endophthalmitis in a human case (Sponsel et al., 2002).
The genus Microsphaeropsis belongs to the order Sphaeropsidales (Coelomycetes) and comprises nine species (Sutton, 1980). These are dematiaceous fungi, meaning they contain pigment in their cell walls. M. arundinis is principally considered as a pathogen of grasses and has also been suggested as a potential biocontrol agent for the apple scab agent (Venturia inaequalis) and Fusarium head blight (caused by F. graminearum). To date, it has not been reported to cause infections in humans, although M. olivacea has recently been reported as the cause of a rapidly progressing, superficial, maculopapular, erythemic lesion (8 cm diameter) on the shoulder of a 59-year-old immunocompetent women (Guarro et al., 1999); in this patient the lesion resolved completely following a 24-day course of oral terbinafine and topical 1% clotrimazole. A 51-year-old immunocompetent male developed a fungal keratitis due to M. olivacea after sustaining a penetrating injury. The infection resolved after a combination of oral fluconazole, topical natamycin and intravitreous amphotericin B (Shah et al., 2001). These Microsphaeropsis species are similar to other species of Coelomycetes with pigmented conidia that cause infections in humans and other animals, such as Coniothyrium fuckelii or Sphaeropsis subglosa (de Hoog and Guarro, 1995). These coelomycetes are common saprophytic and plant parasites that rarely cause localised invasive disease of mammalian hosts (Punnithalingham, 1979). In tissue they develop hyphae similar to those produced by other filamentous fungi, however in culture they are recognised by their conidiomata. The most common coelomycete causing human infection is Scytalidium dimidiatum (also known by the name of its pycnidial synanamorph Hendersonula toruloidea). It is frequently found causing skin and nail infections in people living in the tropics (de Hoog and Guarro, 1995). Interestingly, coelomycetes seem to have an affinity for keratin.
The present cat represents the first reported case of M. arundinis infection in a mammal. This species should thus be added to the list of saprophytic fungi capable of producing invasive disease in mammalian hosts. Two other human cases of M. arundinis have since been identified, but are yet to be published (Pendle et al., 2003). The first was isolated on the dorsum of a hand in a myelofibrosis patient on concurrent prednisolone therapy. The second was identified from ulcerating lesions in a diabetic patient. Both patients were cured by antifungal therapy and amputation, respectively.
Footnotes
Acknowledgement
Richard Malik is supported by the Valentine Charlton Bequest of the Post Graduate Foundation in Veterinary Science of the University of Sydney. Thanks to the Mycology Unit, Adelaide Women's and Children's Hospital and the Mycology Reference Laboratory, Royal North Shore Hospital for isolating and identifying the Fusarium species. Also thanks to the Orange Agricultural Institute for identification of the Microsphaeropsis species. Thanks also to Geraldine Hunt for performing the final surgery.